
Abstract

Codman EA. A study in hospital efficiency: As demonstrated by the case report of the first five years of a private hospital. Boston, MA: Thomas Todd, 1918.
Every hospital should follow every patient it treats, long enough to determine whether or not the treatment has been successful, and then to inquire, “if not, why not” with a view to preventing similar failures in future.
1
Although some of these innovations may seem obvious today, we need to remember that all new ideas were created by people working in a particular place and a specific social, political, and economic context. In this instance, the place was early 20th century Boston, and the person was a brash, ambitious surgeon named Ernest Amory Codman.
Codman was, from the outset, an especially promising young man. An 1895 graduate of the elite Harvard Medical School, he became a house officer at Massachusetts General Hospital (MGH) and then joined the hospital staff. From the outset, he pushed the boundaries of clinical care. He was the first person at MGH to diagnose and successfully operate on a patient with a perforated duodenal ulcer, and only three years after the invention of the X-ray machine, he studied the X-ray appearance of human joints. 2
Codman came of age at a propitious time for someone wanting to shake up the medical establishment. He chose to enter the exciting field of surgery. Surgeons, the dominant specialists of the early twentieth century, armed themselves with the new tools of anesthesia and antisepsis and devised new and innovative ways to operate on patients, increasingly within hospitals. 3
Those hospitals were fast becoming essential elements of the health-care system. They grew larger and more complex. How to manage these intricate institutions? Not for the last time, hospital administrators looked for solutions to the business world, emulating systems being used scientifically to manage rapidly growing factories. 4 Perhaps no idea was so important within the factory walls, or to Codman’s efforts within the hospital, as the desire to be efficient, to measure, to use new scientific tools systematically to organize the hospital workplace in general and the operating room in particular. One central idea, Taylorism, originated with the mechanical engineer Frederick Winslow Taylor. 5 Codman’s friends, Frank and Lillian Gilbreth, invoked Taylorism as they tried to standardize operative processes by recording movies inside operating rooms. 6
These management philosophies resonated with Codman’s basic instincts. He believed that high-quality care did not derive from fancy equipment or showy offices. Nor did he place much faith in the self-assessments of his fellow surgeons, who he saw as being too quick to ‘puff themselves up’ as being superb. 7 Codman mocked those who would judge surgeons based on their ‘nerve’, ‘steady hand’ and ‘graceful’ operating style. Better to measure what actually happened to patients after they went under the knife, as embodied in the incisive quote above. The goal of Codman’s system was to cut through posturing and get to the facts. Did the operation actually work?
Codman’s accomplishments, however, were limited by his personal style. He was not a team player. After trying and failing to implement an end results system at MGH on his own, he urged the medical staff to appoint a lay trustee to do so. Because they refused, Codman resigned from the MGH in 1914. 7 He followed his resignation with an application to become Surgeon-in-Chief based on his excellent clinical outcomes – his application was (not surprisingly) unsuccessful. Soon thereafter, Codman came to the Surgical Section of the Suffolk District Medical Society, where he displayed a huge, three-paneled cartoon depicting his colleagues as being more interested in making money (as depicted in golden eggs) than in advancing scientific understanding of the actual outcomes of their medical care. As a result of this display, Codman was forced to resign his faculty position at the Harvard Medical School. 7
Blocked at the MGH, Codman applied the end result system within his own private hospital. (The modern hospital was still in its infancy, and it was not unusual for physicians to establish small hospitals.). Codman described the results in a book that he sent to other hospital administrators, suggesting that they, too, adopt his system. He was not shy about pushing its significance, claiming it to be comparable to anesthesia, asepsis or the X-ray, all signifiers of modern medicine that had played a major role in his career. 7
Codman’s primary goal was accountability for medical care. He was willing to subject himself to the same scrutiny as he sought for others. In his book, he detailed the results of over 300 patients treated in his private hospital, with details about the specific causes of any untoward outcomes. He also listed all patients who died while under his care at the MGH. In other words, Codman was willing to make his personal operative results quite public and to draw conclusions about what went wrong. He argued that all other surgeons should do the same.
Equally important is how Codman tried to analyse information about that care. It is no longer particularly innovative to gather electronic health records or to analyse data with powerful computerized statistical programs. Such tools enable an intensity of analysis simply not possible in Codman’s world. To find the roots of how we use computers to organize health-care data, we only need look to the back cover of Codman’s treatise.
There Codman presented his evidence in a single 33-by-22 inch sheet (Figure 1). On unfolding the thin, flimsy sheet of paper one sees a series of rows and columns referencing details of 337 patients seen from 1 August 1911 to 1 August 1916. The individual patient data were originally recorded on index cards; with this sheet Codman was trying to enable analysis by organizing the information. The rows show the anatomic location, the columns the pathological condition. The size of the sheet simply reflects the maximum size of a manageable piece of paper and the minimum size of legible printing.
Insert for Codman study in hospital efficiency.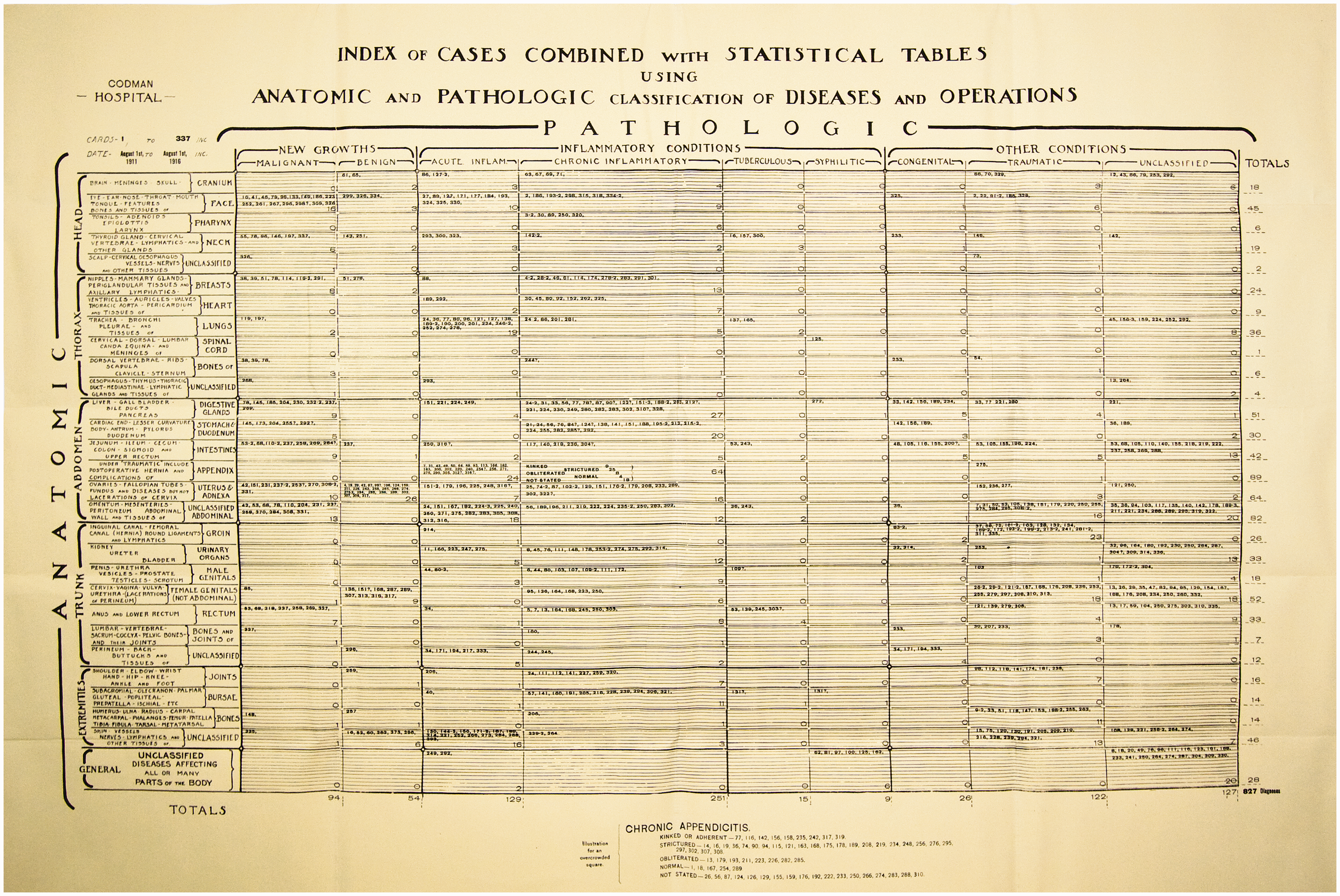
This sheet resembles nothing so much as today’s electronic spreadsheets. A computer-generated spreadsheet is an imaginary sheet of paper essentially infinite in all directions. We use it to manipulate data in ways that Codman could not even imagine. But the very concept of systematically organizing outcomes data, first on index cards and then on a large folding sheet, while unimpressive by today’s standards, was a significant innovation. Codman’s approach fits with the general desire to systemically organize all manner of activities (including hospital care) in the early years of the 20th century. Computers are remarkable tools, but decisions have to be made about how to write programs to analyse data, and our current use of spreadsheets for health services research started with Codman, index cards and a large sheet of paper.
We are well past Codman’s pen and paper technique for assessing the quality of health care. We can manipulate multiple variables and account for confounders. However, we still lack an essential element of Codman’s dream, which was to follow the end result for every patient. Accountable care organizations move us in this direction, as does the monitoring of readmissions. But we still need greater use of patient reported outcome measures related to quality of life and functioning. 8 In the US, the National Surgical Quality Improvement Program (https://www.facs.org/quality-programs/acs-nsqip) and Michigan Surgical Quality Collaborative (http://www.msqc.org) have taken up the charge to measure and disseminate surgical end results.
We fall short of Codman’s ideal world in at least one other dimension. He wanted doctors to be central to quality improvement but today many remain passive recipients of quality and outcome measures rather than active participants in responding to these measures. Despite our current emphasis on quality measurement, most doctors lack Codman's intense personal and systematic commitment to tracking outcomes. Doctors tend to take a strong interest in their best and worst outcomes but relatively few measure and report the outcomes of all their patients as Codman did.
As we reflect on Codman’s landmark book nearly a century later, it should not be surprising that we have ceased to see as remarkable Codman’s most profound innovation – how he chose to sort outcomes. This is often the case for the truly important inventions. It has been observed that ‘The most profound technologies are those that disappear. They weave themselves into the fabric of everyday life until they are indistinguishable from it’. 9 So it is with the systematic sorting of patient outcomes. A century on, Codman stands as a brilliant, irascible and ultimately prescient pioneer in the field of quality measurement and improvement.
Footnotes
Acknowledgements
The authors would like to acknowledge the assistance of Christina Camilli-Whisenhunt in preparation of the figure.