
Abstract
The importance of external governance of health care processes is well documented.1,2 The inclusion of multiple disciplines throughout health care governance, ranging from doctors and nurses to managers and patients, has enhanced quality assessment, assurance and improvement and, along with hospital managers and politicians, the representation of the lay population has hugely developed from this drive. This is justified, as they are the users of health care.
Lay representation in the governance of health care organizations allows for improved probity, greater appreciation of the public interest and stronger external oversight.3,4 However, the transparency of guidance in the selection of individuals for such positions has led to uncertainty as to whether lay groups represent the views of the general public. 5 There is a paucity of guidelines that outline the eligibility criteria required for this role; indeed, many individuals acting in a lay representative role appear not to represent typical service users. 5 Medical professional associations and related regulatory bodies are a core part of the system maintaining and improving health care 6 ; hence, it is paramount that the opinions of the patients are listened to and carry weight in the deliberations and decisions of such organizations.
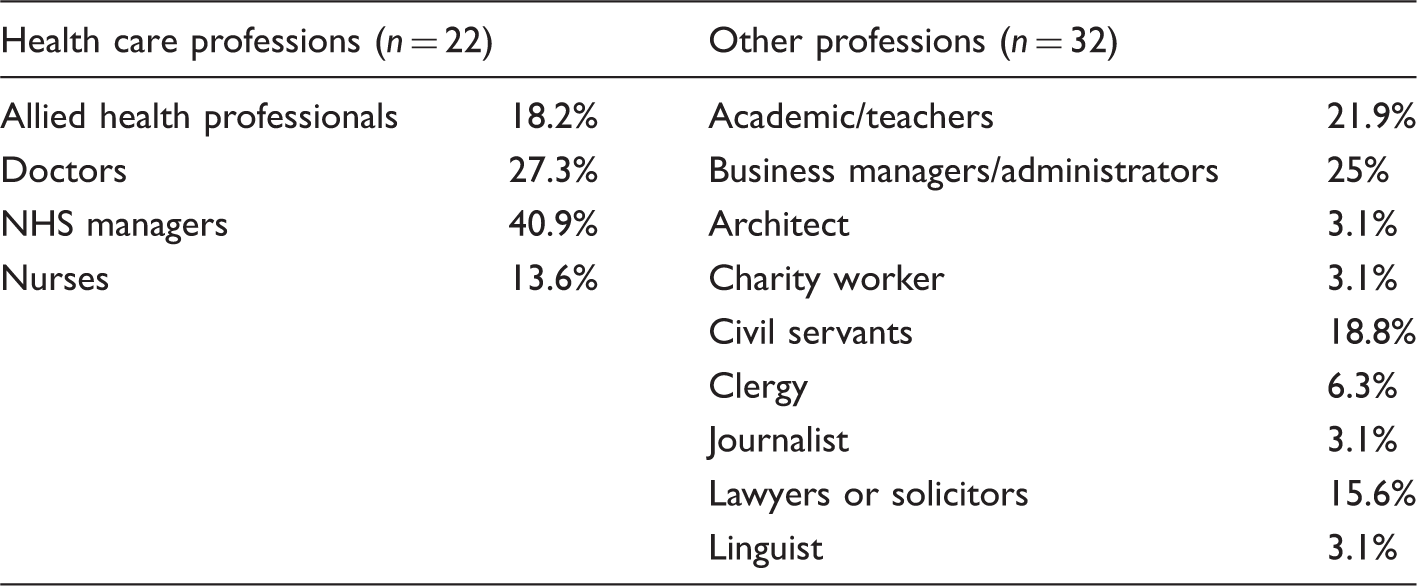
Professions of the lay representatives identified.
There appears to be a similar limited level of public representation in other countries. Of the 10 main medical and surgical associations we contacted in the US, Canada, Australia, India and Germany, only 2 had lay representation: the Australian Medical Association described a ‘limited participation from lay people on its committees and boards’ with lay involvement in its Audit and Risk Committee and Ethics and Medico-legal Committee, whilst the American Medical Association described only one role, for a non-medical external member who is appointed to its Board of Trustees every four years. The Indian Medical Association appears to have no defined role for lay representation, describing only an apparent informal use of various consumer organizations when representation of health care users is required. In Germany, there is no uniform use of lay representation due to the presence of formalized medical self-governance within the country. Yet, the German Medical Association did state that lay members are involved within the arbitration boards of some states (all information obtained via direct communication). Of the remaining associations surveyed who responded, either no lay representation was in place. It would seem that the issues faced in lay representation in the UK are similar internationally.
Other industries and professions have made a major contribution to health care improvement in recent years.7,8 The role of the lay public appears under-developed in medical and related bodies. Other professions and systems appear to be better placed in this regard. For example, the UK legal system provides guidance on lay representation in a variety of roles. For example, the eligibility criteria to become a Lay Magistrate, a public volunteer who acts to hear cases in criminal, civil or family court cases, state that applicants cannot have any conflicts of interest in the role, such as previous employment as a police officer. 9 Once selected, individuals receive formal training on their remit, another factor which was not evident within the health care professional bodies.
In England, individuals who act as Lay Visitors to prisons or prisoners (Independent Custody Visitors) are required never to have been ‘employed in Ministry of Justice … [or] employed by or with direct links to the companies involved in providing custody related services’. 10 Such clear guidance leaves no room for misrepresentation and aligns the role with its objective.
By contrast, there remains a lack of transparency in the selection process for the lay representatives on UK and other countries’ professional health care bodies, leading to a disproportionately large number of individuals in a lay representative position who have a background in health care. Greater guidance in the selection and scope of lay representation for these professional bodies is required. If better representation of the public is to be achieved, suitable guidelines must be developed.
Action is being taken to ensure that the public voice forms a central part in the future direction of health care systems such as the NHS 11 and this should therefore also be true for health care professional bodies. Patients want to be treated as partners by health care professionals and to be informed and involved in the choices made regarding their wellbeing. This should also hold true for professional bodies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.