
Abstract
Objective
School-based health services (SBHS) have been shown to improve access to mental health services but the evidence of their effectiveness on students’ mental health is lacking. Our objective was to examine associations between variation in the provision of SBHS and students’ mental health.
Methods
A cross-sectional analysis of a nationally representative health and well-being survey of 8500 New Zealand high school students conducted in March–November 2012. Students’ mental health is related to data on school health services obtained from clinic leaders and clinicians from 90 participating high schools.
Results
After adjustment for socio-demographic differences in students between schools, increasing levels of services were associated with progressively lower levels of student-reported depressive symptoms (p = 0.002), emotional and behavioural difficulties (p = 0.004) and suicidality (p = 0.008). Services with greater levels of nursing hours (p = 0.02) and those that performed routine, comprehensive psychosocial assessments (p = 0.01) were both associated with lower levels of student-reported depressive symptoms. Greater levels of nursing hours and doctor hours were associated with lower self-reported suicidality among students.
Conclusions
Although a causal association between school-based health services and students’ mental health cannot be demonstrated, these findings support the benefit of such services and the need for a cluster randomized trial.
Introduction
Globally, mental health problems are common and burdensome to children and adolescents.1–3 One avenue for improving access and support for youths is by school-based health services (SBHS). 4 These provide comprehensive and appropriate care, which aims to be accessible and low-cost. While SBHS have been shown to improve access to mental health services, 5 evidence of its effectiveness in terms of students’ mental health is limited.6,7
Studies in this field face methodological and ethical challenges. 8 Randomized controlled trials have not been undertaken and would require cluster randomization. 9 Observational studies face hurdles in matching schools providing health services with control schools to avoid confounding. Those observational studies that have been conducted have ignored variability in the level of health services provided and simply considered the presence or absence of health services. 10 SBHS can vary from occasional visits by a health professional to comprehensive well-resourced clinics with a permanent team of health professionals on-site.
Our aim was to determine whether students in schools with SBHS have better mental health, and to identify particular characteristics of school health services that are associated with students’ mental health. SBHS in New Zealand have a long history as part of public health nursing services. Since 2008, there have been initiatives to improve access to primary health care through partnerships between health and education leading to government funding of SBHS in lower socioeconomic schools. Based on previous recommendations for effective SBHS,11,12 we hypothesize that better student mental health will be associated with comprehensive, well-resourced school health services that are well-integrated within the school and community.
Methods
Participants and study design
Student data were collected as part of Youth’12, an anonymous nationally representative survey of the health and well-being of high school students conducted in 2012.13,14 Sample size calculations for this survey aimed to give reasonable prevalence estimates of health indicators among the four main ethnic groups. 14 The survey utilized a two-stage cluster design, involving a random selection of 125 of the 397 high schools with more than 50 students in year 9 or over, and then, within the 91 schools that agreed to participate, taking a random selection of 20% of the school roll, or in the 13 schools with fewer than 150 pupils, a random selection of 30 students. In total, 8500 randomly selected high school students completed the survey, accounting for 3% of all students.
Apart from a slightly higher percentage of female students, the participating students were similar demographically to the national population of students. 14 Response rates for schools and students were 73% and 68%, respectively. The most common reasons for students not participating were being absent from school or involved in other school activities on the survey day and student refusal.
The anonymous, comprehensive, 608-question multimedia survey was administered using Internet tablets. 15 No keyboard data entry was required; questions and answers could also be heard through headphones, and responses were made by touching the screen. Participants could skip any question or section of the survey at any point. Written consent was required from each participating school and student, while parents could opt to have their child excluded from the survey. Ethics approval was gained from the University of Auckland Human Participants Ethics Committee (ref 2011/206).
SBHS data
Of the 91 schools that participated, one subsequently closed so it was excluded from the analysis. The remaining 90 schools were invited and agreed to participate in a school health services survey after the student survey had been conducted in 2012. A letter was sent to all principals asking for their consent to take part and to nominate a contact in their school regarding the school health services. These nominees were then contacted by phone and asked to fill in an on-line survey on the health services in their school. They were also asked to provide contact information for all health professionals working in the school. The health professionals were then contacted and asked to complete an on-line survey on their work in the school. Of the 90 schools, 11 (12%) reported first-aid only or no health services. In the remaining 79 schools, 129 health professionals were identified of which 113 replied to the health staff survey (response rate of 88%). Health services data were collected within 12 months of the student survey.
School characteristics
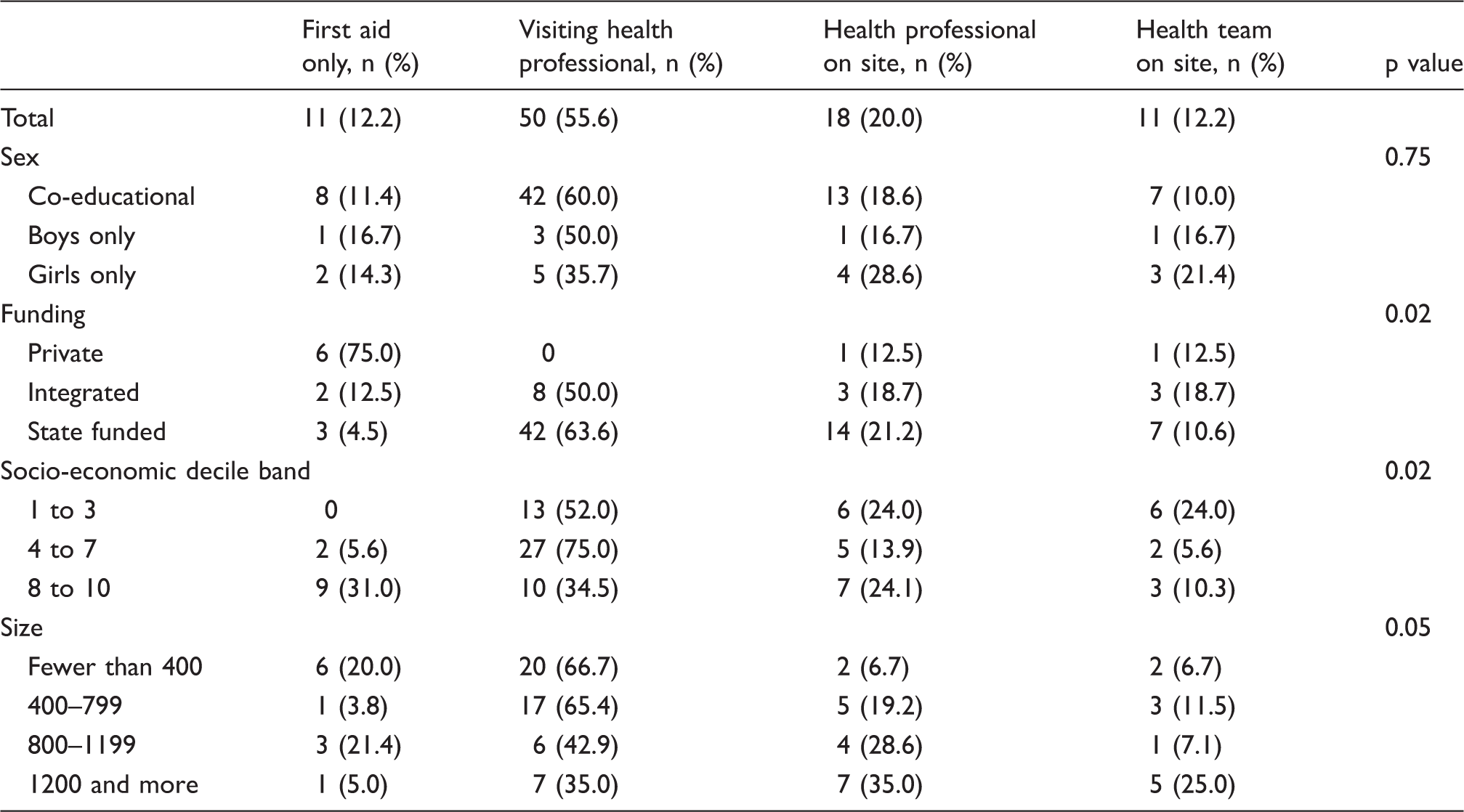
Structural characteristics of schools were obtained from the New Zealand Ministry of Education. Schools were characterized by the sex of students (co-educational; boys only; girls only); school funding type (private; state funded; ‘integrated’); size (fewer than 400, 400–799, 800–1199 or 1200 and more students); and the school socio-economic decile (1–3, 4–7 or 8–10). Integrated schools are former private religious schools that were ‘integrated’ into the state education system in 1975 because of funding problems. These schools receive government funding but retain their religious ethos. The school decile is determined by the Ministry of Education and is calculated from census data. Decile 1 schools represent schools with the highest proportion of students from low socio-economic communities, whereas decile 10 schools are those with the lowest proportion of these students. 16
Variables used to describe school health services
The health clinic leaders or equivalent in each school were asked to complete a questionnaire on level of health service provided, facilities available, use of routine comprehensive psychosocial assessments (for example HEeADSSS assessment at Year 9 17 ), level of collaboration with the pastoral care team within the school, integration of the school health service with the rest of the school, and presence of a relationship with local primary health services (e.g. local General Practice, Independent Nurse Practitioner). Each participating school health professional was asked to complete a questionnaire that sought information on their professional role, hours per week usually worked at the school, and availability and helpfulness of specialist mental health support. School health service questions and response options and student demographic variables and mental health measures are described in Supplementary Appendix 1.
Data analysis
General linear multilevel regression models accounting for the correlation between students from the same school were used to investigate the associations between characteristics of health services at schools and mental health outcomes among the students at those schools. There were no missing data for level of school health services and very little missing data on other school health service variables. Among student-level variables, there was less than 10% missing data for the Reynold’s Adolescent Depression Scale (n = 7802), total difficulties score (n = 8188) and suicidality score (n = 8326). No attempt was made to impute data for missing responses. Two general linear multilevel regression models were used to estimate the associations between school health service variables and students’ mental health (depressive symptoms; behaviour and emotional difficulties; suicidality). The first model was to allow for differing student composition between schools and included student-level covariates: age, sex, ethnicity, socio-economic deprivation and rural-urban location. The second model extended the first model to allow for possible contextual differences between schools and included school-level covariates. Estimation techniques used residual maximum likelihood with Satterthwaite degrees of freedom using the Mixed procedure in SAS version 9.3 (2010; SAS Institute, Cary, NC).
Results
Students
The final sample included 8483 students from 90 schools. The sample was representative of the overall New Zealand secondary school population 14 with 64.6% of students aged 15 years or younger. There were slightly more female students (54.3%) than male students (45.7%). The prioritized self-reported ethnicity of students was Asian (12.4%), Maori (19.9%), Pacific (14.2%), Other (6.0%) and New Zealand European (47.4%). Twenty percent of students were from households experiencing socio-economic deprivation.
The mean score (standard error) for depressive symptoms, total difficulties and suicidality was 19.6 (0.07), 11.4 (0.06) and 1.26 (0.01), respectively. Scores for all three measures were higher among female students than male students (p < 0.001), higher among 15- and 16-year-old students than other age groups (p < 0.001), higher among students living with poverty than those not living with poverty (p < 0.001) and higher among students from small towns compared to students living in larger cities or in rural areas (p < 0.001). Students who did not identify with one of the four major ethnicities reported higher mean scores for depressive symptoms compared to students from the other ethnic groups (p < 0.001). Maori students reported higher mean scores for total difficulties compared to students from other ethnic groups (p < 0.001) and both Maori and Pacific students reported higher levels of suicidality compared with the other ethnic groups (p < 0.001).
SBHSs
Comparison of level of school health service with school characteristics (N = 90).
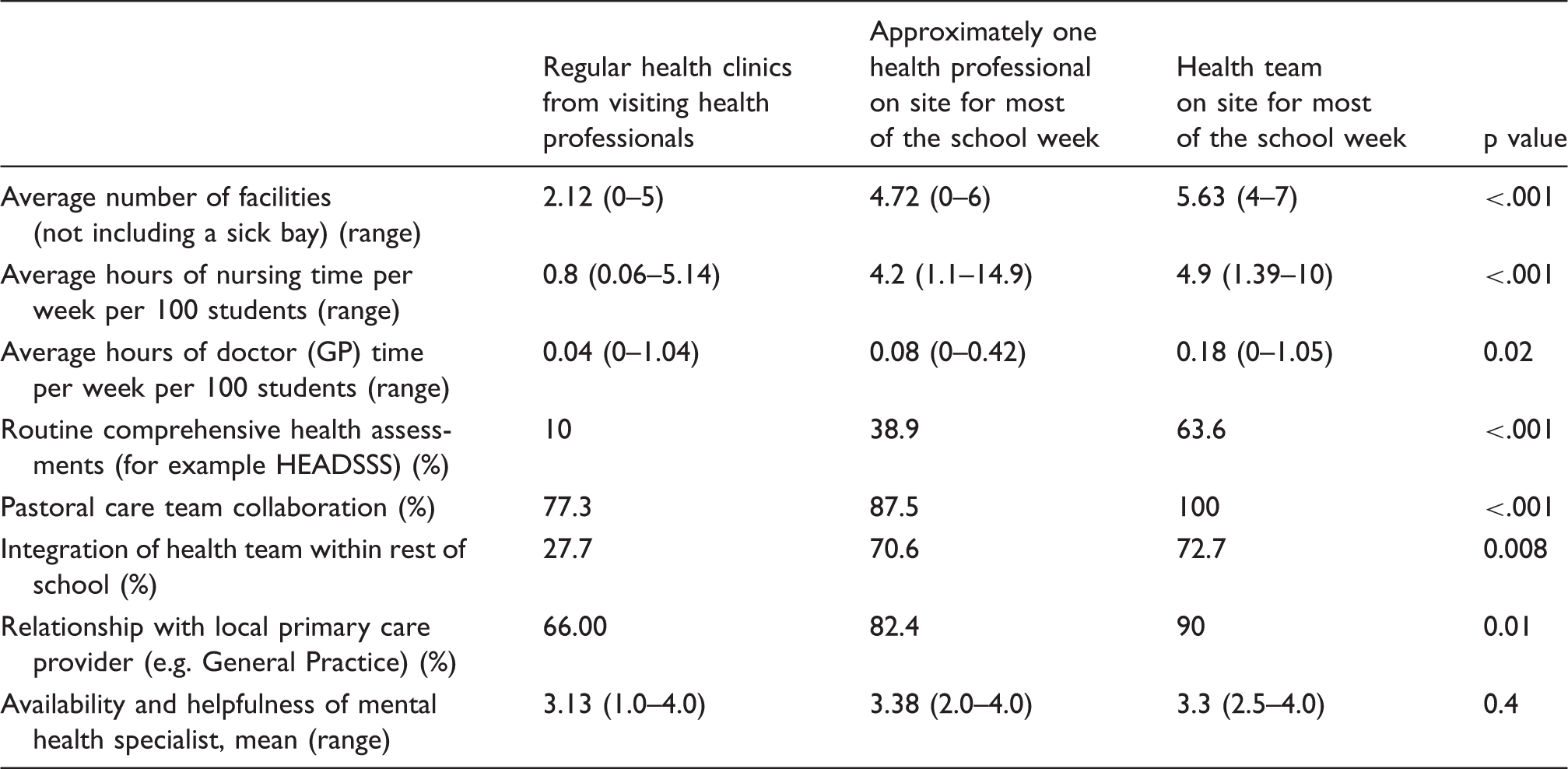
Comparison of school health service characteristics with level of school health services (N = 79).
Associations between school health service and students’ mental health
Comparisons of student depressive symptoms, SDQ total difficulties score and suicidality by level of school health service (N = 7802).
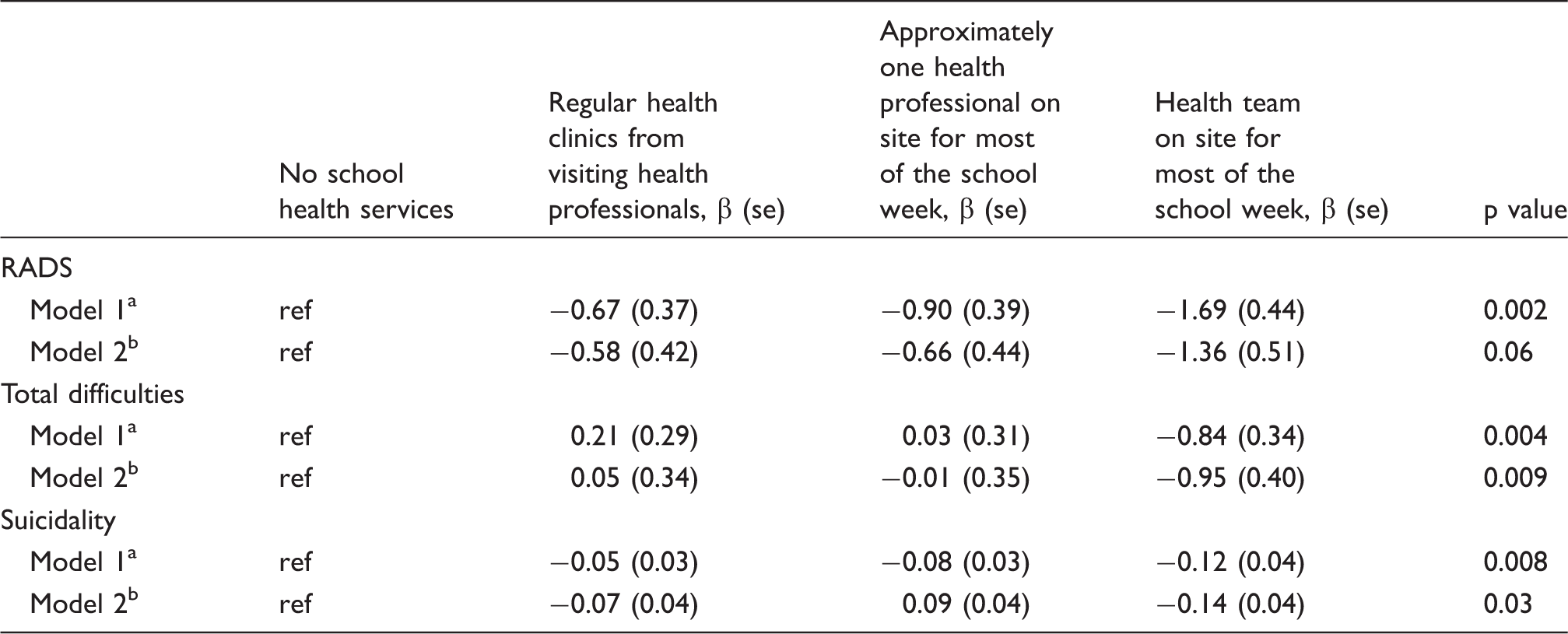
Fixed effect estimates from multilevel model adjusted for individual covariates (age, sex, ethnicity, socio-economic deprivation and urban-rural location).
Fixed effect estimates from multilevel model adjusted for individual covariates (age, sex, ethnicity, socio-economic deprivation and urban-rural location) and school-level covariates (school gender, funding, school decile and school size).
Fixed effect estimates of school health service characteristics for models of predictors for depressive symptoms, SDQ total difficulties score and suicidality (N = 7802).
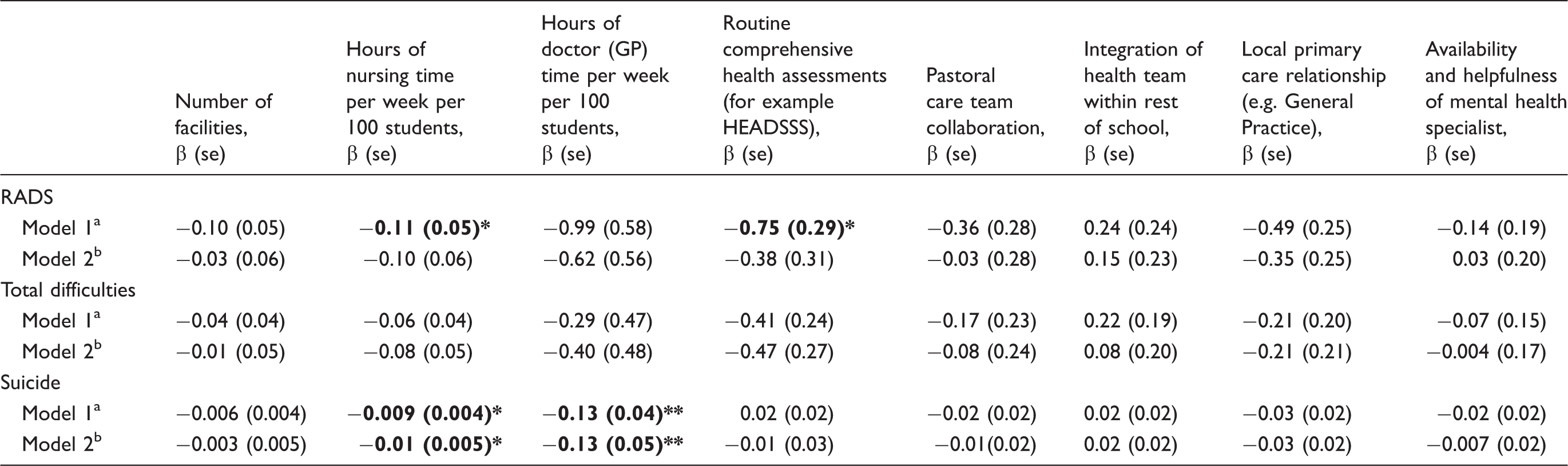
p < 0.05.
p < 0.01.
Model adjusted for individual covariates (age, sex, ethnicity, socio-economic deprivation and urban-rural location).
Model adjusted for individual covariates (age, sex, ethnicity, socio-economic deprivation and urban-rural location) and school-level covariates (school gender, funding, school decile and school size).
Discussion
Main findings
Once demographic differences between schools are accounted for, higher levels of SBHS are associated with better student mental health. Furthermore, some specific health service characteristics are positively associated with better mental health among students, namely increased nurse and doctor (GP) time per week per 100 students and the provision of routine comprehensive psychosocial assessments. Identifying and supporting students with mental health concerns requires asking the right questions in an environment whereby the student has trust in the clinician and the clinician has time to support and follow-up issues causing the student distress. The HEEADSSS method of interviewing is a well-known comprehensive psychosocial assessment designed to elicit mental health issues as well as other risk behaviors. 17 While it has been widely utilized in youth health settings, there are only a few studies evaluating its impact. 18
Previous studies of SBHS have only compared the presence or absence of school health services,6,10 or compared users or non-users of school health services. 8 Our study identifies particular characteristics of SBHS associated with mental health, including the amount of doctor and nursing time provided and the provision of routine comprehensive psychosocial assessments. While other characteristics of higher level services did not reach statistical significance in their association with student mental health, trends suggest a synergism where more comprehensive, better resourced services are better able to manage the broad range of youth mental health needs.
Limitations
This is a cross sectional study showing associations, so conclusions about causation cannot be made. It may be that school health services have been concentrated in schools with students experiencing low rates of mental health problems, but this seems unlikely given the targeting of school health services to low socio-economic schools. A further limitation is that the analysis is based on the provision of SBHS in schools rather than student utilization of those services. It may be that schools that provide SBHS have other characteristics that are associated with good mental health among students. Further researches, ideally randomized studies, are needed to assess the causal role of SBHS.
The study sample is drawn from students attending New Zealand high schools on the day of the study. This excludes those absent from school and those no longer enrolled at school; groups of young people who are known to have higher rates of mental health concerns.19,20 It may be that health centres have been established in schools with higher absenteeism and drop-out rates, but research suggests that users of school health services have better school attendance 21 and retention. 22 The evaluation of mental health problems relies on self-report questionnaires, without parent or teacher sources of information, which may introduce bias by over- or under-reporting.
Implications
As the associations observed cannot establish causality, cluster-randomized trials alongside quantitative and qualitative process evaluations are needed. In the meantime, these findings are useful for policy makers and clinicians working in school health clinics as they demonstrate that well-resourced and comprehensive SBHS are associated with better mental health among students. In particular, sufficient staffing levels in SBHS and routine comprehensive health assessments, such as HEADSSS, appear to be important components of high quality and effective SBHS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Youth’12 project was funded by the Ministries of Youth Development, Social Development, Health, Education and Justice; the Department of Labour; Families Commission and the Alcohol Advisory Council of New Zealand.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.