
Abstract
Objectives
Health services worldwide are increasingly adopting consumer directed care approaches. Traditionally, consumer directed care models have been implemented in home care services and there is little guidance as to how to implement them in residential care. This study used a citizens’ jury to elicit views of members of the public regarding consumer directed care in residential care.
Methods
A citizens’ jury involving 12 members of the public was held over two days in July 2016, exploring the question: For people with dementia living in residential care facilities, how do we enable increased personal decision making to ensure that care is based on their needs and preferences? Jury members were recruited through a market research company and selected to be broadly representative of the general public.
Results
The jury believed that person-centred care should be the foundation of care for all older people. They recommended that each person’s funding be split between core services (to ensure basic health, nutrition and hygiene needs are met) and discretionary services. Systems needed to be put into place to enable the transition to consumer directed care including care coordinators to assist in eliciting resident preferences, supports for proxy decision makers, and accreditation processes and risk management strategies to ensure that residents with significant cognitive impairment are not taken advantage of by goods and service providers. Transparency should be increased (perhaps using technologies) so that both the resident and nominated family members can be sure that the person is receiving what they have paid for.
Conclusions
The views of the jury (as representatives of the public) were that people in residential care should have more say regarding the way in which their care is provided and that a model of consumer directed care should be introduced. Policy makers should consider implementation of consumer directed care models that are economically viable and are associated with high levels of satisfaction among users.
Keywords
Introduction
Consumer directed care refers to a model of service delivery in which consumers are given greater control over their care. 1 Key elements include person-centred and goal-based care, greater choice, a focus on wellbeing and quality of life, individualized budgets and options for people to purchase additional services where they have the means to do so. 2 Consumer directed care, also referred to as ‘cash for care’ or ‘personal budgets’, in home care has been implemented in a number of countries over the last 30 years, including Australia, England, the Netherlands, New Zealand, and the United States, among others.3–6 Models differ, providing consumers with variable levels of control over their own care. Some research suggests that such an approach may improve satisfaction with care and empowerment. 7
In Australia, the implementation of consumer directed care models has historically involved home care services and all home care packages are now provided using a consumer directed care model. 8 However, when they move to residential care, consumers will experience much less autonomy and control over their care than they have become accustomed to through the consumer directed care scheme in home care. The current funding model for residential care involves the Australian government paying approved providers a specified amount for each resident and the resident has little influence regarding how this funding is spent. The Australian government is currently investigating how the principles of consumer directed care may be applied in residential care. 2
Internationally, the use of consumer directed care schemes within residential care is not well understood in terms of how to best operationalize the model. 7 A 2014 report commissioned by the Australian government scoped the applicability of consumer directed care in residential care through a review of the literature and consultation with key stakeholders from residential care organizations and advocacy groups. 2 The consultation revealed high level support for person-centred care and qualified support for consumer directed care, particularly the control of funds. There were concerns about how the approach could be applied in the current Australian context, which is highly regulated and has a strong culture of risk aversion. Stakeholders predicted there would be complex scenarios where resident choices were in conflict with the health professional’s duty to provide safe care. The report failed to identify models used in other settings that could be directly transferred to the local context.
A small-scale pilot of consumer directed care in residential care in Australia involved six aged care facilities and included, among other things, staff education and training in consumer directed care and the use of a Resident Care Form. 9 Residents were not provided with individualized budgets to manage their care in this pilot. Preliminary findings suggest increased wellbeing among residents following implementation of the training. However, there were minimal changes in staff and organizational measures. 9
A pilot of direct payments in residential care in England identified three main models of funding: providing the resident with the full amount of money to spend; continued payment of the residential care fee by the local authority and providing the resident with some additional funds to spend; and dividing the money between the resident and the local authority, each taking responsibility for some of the payment. 10 The evaluation of this pilot found that users reported some benefits including a greater sense of empowerment and the ability to access different services. Uptake of the scheme was poor within councils and among residents, suggesting that the approach was not particularly desirable for either group. Costs of implementation were considered to be high despite the poor uptake and establishing the payment arrangements was viewed to be time consuming.
Evaluations of consumer directed care in home care settings have highlighted additional concerns, such as that some consumers preferred support in managing their care and found the control of budgets burdensome and isolating.4,11,12 There are further challenges when the person receiving care has dementia or other conditions that restrict decision-making ability and does not have a support network that can help with decision making and care management.
In summary, the use of consumer directed care principles in residential care appears to be challenging; existing models have had limited success and cannot be easily replicated. While there is a commitment to more person-centred care overall, it remains uncertain how to strengthen decision making among residents in a shared environment within existing funding models.
This paper describes a citizens’ jury in which these challenges were posed to a group of members of the public who were also asked to generate recommendations which could be used to inform the move towards consumer directed care in residential care in Australia. Citizens’ juries are a deliberative democratic method used to engage members of the public in policy decision making. 13 Policy makers and health system planners in Australia have supported the use of citizens’ juries and the methodology has been used to address a variety of issues including the taxing of soft drinks, immunization of adolescents and prioritization of emergency department services.14–16 Some previous citizens’ juries have led to changes in policy. For example, jury recommendations about safe cycling in South Australia led to new government spending on bike boulevards and changes to cycling laws. 17 However, identifying links between jury outcomes and policy formation are difficult and the ability of juries to directly influence policy has been questioned. A 2014 review of the evidence of citizens’ juries 13 found that a number of juries had not adhered to the traditional model (as set out by the Jefferson Centre 18 ). Lehoux et al. 19 examined what participation of citizens in deliberative processes means to the individual, reporting that people should not be considered simply as representatives based on their demographic characteristics but as people with cultural, relational and cognitive resources who bring their lived experiences to participation in deliberative processes.
Method
This study used a citizens’ jury to explore the views of members of the public on how to increase personal decision making for people in residential care. Citizens (‘jurors’) are provided with a question (‘charge’) and information relevant to the question. The information is presented by a range of topic experts (‘expert witnesses’) who are deliberately chosen to provide balanced information about the topic. Jurors are usually given the opportunity to ask questions of the expert witnesses to ensure that they have the information that they need to make recommendations on the issue. 18 Following the presentations, the jury deliberate and deliver their verdict (answers to the questions) and the information is presented back to the relevant policy or decision makers. This paper describing the jury adheres to the checklist developed by Thomas et al. for reporting community juries. 20 Ethical approval for this citizens’ jury was obtained from the Flinders University Social and Behavioural Research Ethics Committee.
Planning
A steering group involving eight people was convened in November 2015. The group included: one postdoctoral research fellow, one health economist, three research active medical practitioners (two geriatricians and one rehabilitation specialist), two people involved in a dementia research consumer network and one person employed by a dementia advocacy association. The group generated and refined the question and drafted the program for the jury, including identification of appropriate expert witnesses and topics. Expert witnesses were selected based on their knowledge of the issue, familiarity with practical considerations of service delivery in residential care and skills in engaging audiences. The expert witnesses were proposed by members of the steering group as part of their personal and professional networks. The roles of the witnesses are described below. The charge presented to the group was refined in consultation with the facilitator who had experience in conducting citizens’ juries and was presented to the jurors: (1) For people with dementia living in residential care facilities, how do we enable increased personal decision making to ensure that care is based on their needs and preferences? (2) What mechanisms need to be in place?
Jurors
The jury was conducted over two full days in Adelaide, South Australia in July, 2016 and used methods consistent with other citizens’ juries. 13 Participants (the ‘jurors’) were recruited using a market research company and were selected to be broadly representative of the general public in terms of age, gender and socioeconomic status. Three of the fourteen jurors recruited were targeted because they lived in rural areas, reflecting the balance of metropolitan versus regional populations in Australia. People were not eligible to participate if they were currently working in the field of health and aged care or were a primary carer for someone living with dementia, because it was thought they may bring bias from their own experiences. The market research company used a list of verified mobile and home phone numbers to source participants. Participants were sent information about the jury in advance (the nature of the jury question, venue, transport arrangements, information about the speakers). They were not provided with the charge in advance or any additional information which would help them to consider the charge. Jurors were provided with an honorarium (AU$300) in acknowledgement of the time spent attending the jury. Upon arrival, jurors were provided with copies of the presentations of the expert witnesses and blank paper for making notes.
Procedure and scheduling
An independent facilitator with experience in community engagement and conducting citizens’ juries was recruited and worked with the steering group on refining the jury program. Expert witnesses were all from Adelaide, South Australia; they presented on the first day allowing the second day to be dedicated to deliberations. A geriatrician presented information about the consequences of ageing and dementia and described the usual routines and level of involvement in decision making for people in residential care. He spoke of his experiences of complex decision making where there is conflict between different parties and presented case studies where the resident has cognitive impairment and had insufficient capacity to make decisions. The next presenters were senior staff from two different aged care organizations who provided information on the current climate in terms of funding, regulations and some of the perceived benefits and challenges of introducing consumer directed care principles into residential care for older people. They shared stories to illustrate how each resident has individual preferences; residents were de-identified to maintain their confidentiality. Three consumers (one person with a diagnosis of dementia and her husband and the third with experience of caring for someone with dementia) presented their lived experiences. They spoke of some of the difficulties, the possible benefits of consumer directed care and about how they made decisions or would make decisions in the future while enabling the person living with dementia to have as much autonomy and control as possible. Finally, a researcher with expertise in eliciting preferences and measuring quality of life in people in residential care presented information about what contributes to increased quality of life in residential care. Jurors had the opportunity to ask questions of each presenter.
On the second day of the jury, the facilitator started by conducting a ‘muddiest points’ exercise which involved asking the jurors to discuss their reflections and any unanswered questions as a group. Questions were answered by other members of the jury or by the research team. The facilitator directed the jurors back to the questions for the jury and facilitated deliberations in small groups and then as one larger group.
Data collection and management
The primary output from the jury was a list of recommendations drafted by the jurors’ in response to the questions. On the second day, after clarification of the muddiest points, the facilitator divided the jury into small groups. These groups were asked to work together to address the charge and draft recommendations on a large sheet of paper. Once this process was completed, the facilitator asked a representative from each small group to present recommendations to the larger group. The facilitator encouraged discussion about the shared findings and identified commonalities and some differences between groups. The facilitator then worked with the large group to consolidate the small group recommendations into one final list of recommendations. Before finalization of the recommendations, the jurors were all asked to confirm that they felt satisfied that the recommendations reflected the views of the group as a whole.
In addition, all aspects of the jury (expert witness presentations and group discussions among the jurors) were audiorecorded, providing supplementary data. The recordings were transcribed and the scripts were reviewed for quotes from the jurors that validated the final recommendations and provided more information relating to the jury’s thinking behind particular recommendations. These qualitative data were not coded or reviewed for additional themes as it only contained large group discussions and ideas discussed within the small group conversations would not have been captured. Below we use quotes to illustrate jurors’ discussions but because of the nature of the collection of the data, we do not link individual quotes to individual jurors.
Findings
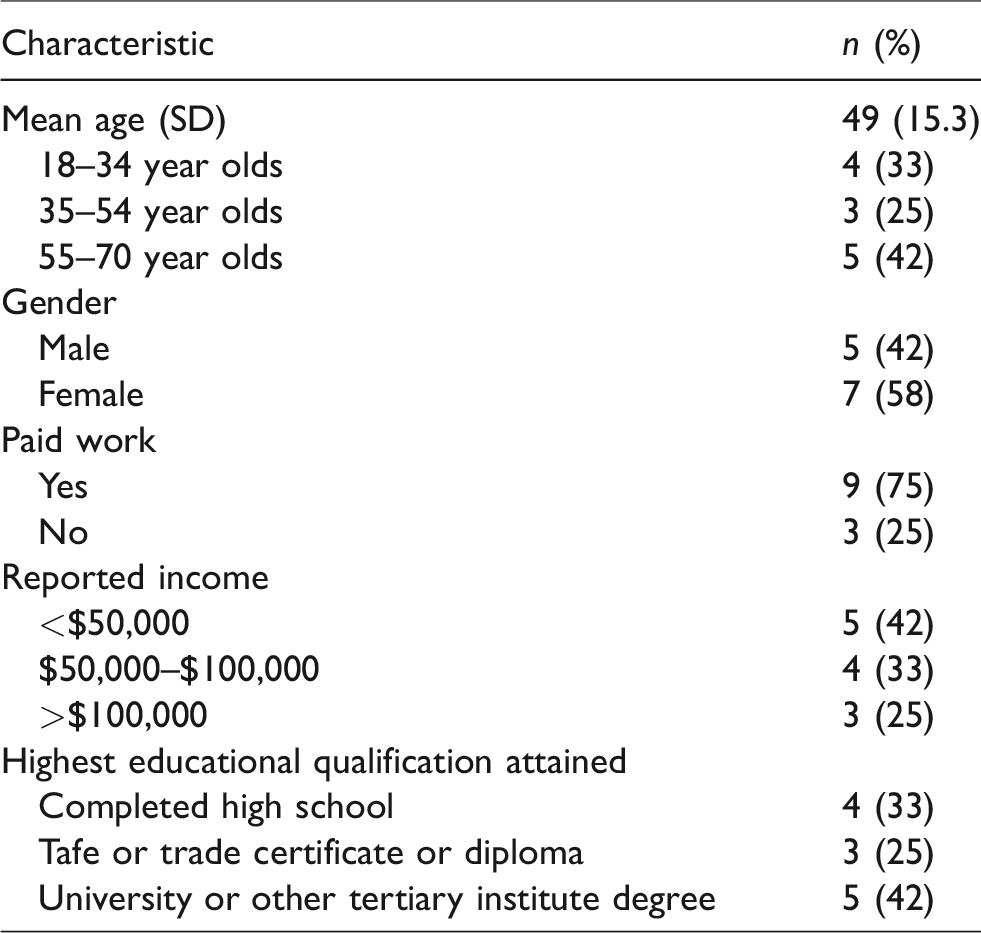
Fourteen jurors were recruited. Of these, one withdrew in the week leading up to the jury and one person did not attend on the day; the final jury consisted of 12 jurors who attended for the full 2 days. Juror demographics are presented in Table 1.
Demographic characteristics of the jurors.
The jury presented a number of recommendations in response to the first question (“For people with dementia living in residential care facilities, how do we enable increased personal decision making to ensure that care is based on their needs and preferences?”). They provided some additional recommendation in response to the second question (“What mechanisms need to be in place?”) while acknowledging that there was overlap and some of the ‘mechanisms’ (from question two) had been outlined in response to the first question. Thus, the key recommendations for both questions are combined and presented here in Table 2.
Citizens' jury's key recommendations for enabling increased personal decision making in residential care to ensure that care is based on needs and preferences.

The jury agreed that while there were benefits in residents having more choice and control, the residential care facility should still have responsibility for ensuring that peoples’ core needs were met (i.e. health, nutrition and hygiene) and as such should be funded and regulated for providing these services.
So we’ve all thought that there should be a base level of care that is not negotiable because the lack of it could be safety, would come to safety. So if I don’t want anyone to clean my room that could then become a safety issue.
So the essentials we’ve got cleaning, health, GP, physio, podiatrist, nursing care, your medicine, your food obviously, your routine such as your shower, getting laundry done.
It was agreed that beyond these core services, the person should have the ability to choose discretionary services which addressed their social, leisure, spiritual or other needs.
And then obviously you’d have your additional services, level of services available. The facility must be able to accommodate these external services and on non-negotiable services there need to be some level of choice. So with your meals, so just say one of the non-negotiables might be your meals. However, I can choose what I want to eat at what time but the facility still has to provide you that meal. The facility would have to have some duty of care in regards to these additional services.
Residents should be encouraged to continue to have the ability to pursue their hobbies and their interests and be creative and getting joy out of those choices. And also, of course, a choice of services that add quality to their life. That can be anything from going to the football to wanting to have a special hairdresser.
In addition, residents with financial means could pay for additional services; the jury acknowledged that this was already the case to some extent.
Person-centred care was considered to be the foundation of care and should take into account the person’s identity, values and preferences. This, the jurors felt, can be achieved through staff that are trained to be decision facilitators. In addition, the person should have more control over their routines and environment including choices around clothing, meals and the timing of activities. The jurors agreed that people should be able and supported to access outdoor areas when they desired.
Innovation in the sector was seen as a potential benefit and the jurors discussed the benefits of a marketplace in which service providers need to differentiate themselves from others and offer high quality services in order to survive. They drew parallels with the education system in Australia and the opportunity for boutique providers and organizations with areas of expertise.
I sort of wonder if all facilities can offer the same sort of services or it should be that certain facilities often specialise in different areas. I’m not saying you’re taking away the person’s right but, you’re just trying to make it easier. Instead of making every facility exactly the same
Going back to the education model again, all schools all get the same funding from the government. But that’s the seed funding so they’ll get x thousands of dollars to have a student go through the education system. Plus, schools can then charge whatever they want on top. Some of the better services, this is where private schools take over. So you have your not for profit type of private schools that all go well, here’s your incentive, A, we’re going to charge you this much but we’ll offer you specialist music, we’ll offer you specialist this and it’s your choice to come to us….
The jury had concerns about the level of existing staffing and other resources within the residential care system. There were anecdotal reports from the jurors of visiting family or friends noticing few staff available and that most staff were care workers and not nursing staff. They were concerned that the introduction of consumer directed care may cause more problems in terms of organizations being able to offer long-term staffing positions and predictable work hours.
My friend who works in aged care, she said the pressure they are under to provide care to very vulnerable but very complex and time-consuming patients or residents is phenomenal.
Concerns were also raised about the vulnerable nature of the residents and that ‘unscrupulous’ goods and service providers could take advantage of this vulnerability with people who were unable to make informed decisions about the potential benefits, harms and costs of the goods or services. There were also concerns about the transparency of arrangements and that it needed to be clear that goods or services purchased were actually provided. Mechanisms such as online portals, mobile phone text messages and scanners for tracking services were suggested as methods which may enable greater transparency.
We looked at our overall concerns and our concerns were for dementia patients, a fear of change, a lack of core services, conflict of interest, the transparency of the delivery of service, resident safety in reference to their choices and residents with no family or friends. So we came up with a couple of ideas that could address those concerns and one was that an ombudsman be appointed to do with the care packages and the changes in the implementation of how patients are cared for.
There were deliberations regarding the need to avoid bureaucracy and micromanagement of budgets. The group hypothesized a scenario in which family members may visit and assist with feeding the person lunch and agreed that the resident or family member should not be compensated for providing this task. The sentiment being that introducing greater transparency in the costs of care should not detract from the overall goal of care workers, families and friends providing the best possible care for residents.
Discussion
In this study, we report on a citizen’s jury which explored the views of members of the public on how to increase personal decision making for people in residential care in Australia. The jury involved 12 jurors who were provided with information from expert witnesses regarding the potential challenges and benefits of introducing a model of consumer directed care into residential care in Australia. The jurors engaged with the information and queried the witnesses in an informed manner, demonstrating their understanding of the complexity of the issue. Overall jurors felt that person-centred care should be the foundation of care for all people in residential care regardless of funding mechanisms. In addition, the jurors felt that the current scenario, in which residents have little choice or control, requires improvement. They agreed that mechanisms needed to be in place in order to operationalize choice and control and that some restrictions would be necessary. These findings echo the views of stakeholders involved in the 2014 scoping report commissioned by the Australian government into consumer directed care in residential care. 2
Stakeholders involved in the scoping report were representatives from leading aged care providers and advocacy groups such as Alzheimer’s Australia, with extensive experience in advocacy and the aged care system and potential conflicts of interest (although these were not declared in the report). For the citizen’s jury reported on here, jurors were excluded if they worked in the health or aged care system or who were primary carers for someone with dementia. We excluded these people because they could have brought biases based on their experience and they could have dominated discussions with other jurors because of their expertise. More importantly perhaps, citizens’ juries as conceptualized here are to provide the perspectives of people who have been largely unaffected by the issue under discussion and are thus expected to bring different questions, ideas and contributions to the policy issue.
Members of the jury were as concerned about risk management strategies as stakeholders consulted for the governments’ scoping report and both groups were committed to the delivery of person-centred care. The citizen’s jury provided a critical perspective that aligns with those of the stakeholders and can further inform policy in the Australian context, in addition to the findings from a pilot trial within Australia, 9 and the learnings from implementation of consumer directed care in home care packages.4,11,12 This study may also inform policy development in other countries that are looking into moving to consumer directed care in residential care.
The model of funding recommended by the jurors (a split between core and discretionary services) has some similarities to one of the models trialled within the pilot of direct payments in residential care in England described earlier. 10 The evaluation of the program found that this particular model of funding was however more difficult to implement than the other models and, as noted, that costs of establishing the scheme were high as was the administrative work involved in managing payments and organizing activities for all models. Uptake of direct payments in the English pilot program was poor and residents will be less likely to choose this model of care if it is associated with considerable administrative costs. Policy makers will thus need to consider how to best streamline processes given the limited amount of resources in the aged care system and large number of service users.
The jurors discussed issues concerning proxy decision making on behalf of people in residential care with cognitive impairment, finding the need to support family and friends acting as decision makers to be important. This component was not identified in the governments’ scoping report. 2 Jurors also strongly felt that better methods of communication were required for transparency (such as online portals). Such an approach would be challenging to implement in most residential care facilities where records are highly confidential and access is restricted to staff. Yet, transparency and enhanced communication would no doubt be welcomed by consumers and the Australian Government is investing in this in the form of My Health Record. 21 Most health records are now electronic and so consideration should be given to providing families with access to some of this information. This could enhance transparency and result in more informed family members which may lead to improvements in care.
The jury frequently compared the proposed model of consumer choice in residential settings to the education system in Australia, in which all children are entitled to public schooling but families can choose to spend more resources to send their children to private schooling. This market for education services means that schools may distinguish themselves from others by their facilities or specialist programs. Jury members envisaged that residential care facilities may pursue a similar path and market their services for people with particular values, interests or preferences. While this raised some concerns about equity, it was also felt that enhanced competition between providers could result in better quality care options for residents.
There appeared to be rapid knowledge development among the jurors. On the first morning of the jury, several of the jurors reported feeling somewhat nervous about making recommendations regarding an issue they were not yet familiar with. But by the next day, they noted to feel more capable of making recommendations and they had few final questions of the facilitator or research team. The jurors were observed to have asked insightful questions of the expert witnesses and project team. This can be seen to illustrate: the investment of the jurors in the deliberations; the relevance of the presentations and engaging speakers; and, the experience and skills of the facilitator. Some of the jurors spoke of the complexity of the issue, their previous naivety into the aged care sector and the great responsibility they felt in making recommendations. This can be seen to demonstrate their sense of accountability and commitment to the process and their insight into the challenges in policy making.
One of the strengths of a citizens’ jury is its deliberative nature. 22 The recommendations of this jury were formed by people who had attended a full day of presentations on the topic and heard from a variety of experts in the field. Following this, a full day was dedicated to discussion, deliberation and achieving consensus. One of the main questions of the usefulness of citizens’ juries is whether they involve tokenistic consultation without subsequent changes in actions or policy. 13 The recommendations stemming from this jury are in line with the thinking of stakeholders suggesting widespread support for consumer directed care. However, most of the changes will require additional funding to instigate the changes. While the main recommendation relates to redistribution of existing funding to core and discretionary funding, there will be administrative costs in establishing this as found within other programs. 10 As there are issues around risk management, extensive work would need to be undertaken to detail the rights and responsibilities of the provider, the resident and their families.
Although changes to funding and service delivery can be difficult, it is often more challenging to change human behaviour which is typically based on established routines and practice. 23 Staff in residential care facilities use routines to manage workload and there is often little flexibility to accommodate resident preferences. 24 A review conducted by Low et al. 25 revealed that changing practice in nursing homes was difficult and that change was less likely to occur if it involved global practice change (rather than just a specific task such as improved oral hygiene practices). Significant changes would need to occur if the resident chooses what they would like and when.
In conclusion, the jurors’ recommendations were relatively conservative and were generally consistent with the views of stakeholders sourced in other contexts. This broad consensus suggests that implementation of the recommendations would be widely regarded as a positive change in service delivery.
Footnotes
Authors’ note
Availability of data and material: Data were captured via written notes, audiorecording and photographs. The data that support the findings of this study are available from the authors upon reasonable request but restrictions apply to ensure the anonymity of the research participants.
Acknowledgements
We wish to gratefully acknowledge the members of the steering group: Ron Sinclair and Jane Thompson. We wish to thank Dr Anne Johnson who assisted in refining the question and agenda and facilitated the jury.
Ethical approval
Ethics approval and consent to participate: This study received ethical approval from the Flinders University Social and Behavioural Research Ethics Committee. All participants provided written consent.
Consent for publication
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Health and Medical Research Council (NHMRC) Partnership Centre on Dealing with Cognitive and Related Functional Decline in Older People (grant no. GNT9100000).