
Abstract
Objective
To assess which older Australian women had Medicare subsidized health assessments between 1999 and 2013.
Methods
This study used prospective, longitudinal survey data from the 1921 to 1926 birth cohort of Australian Longitudinal Study on Women’s Health (ALSWH) linked with Medicare Australia data on health services use. Over 11,000 Australian women were included in the study. Latent class analysis was used to identify assessment patterns over time, accounting for death, and based on three categories (‘no assessment’; ‘assessment; ‘deceased’) for each year between 1999 and 2013. Further analysis explored the impact of health and sociodemographic characteristics on class membership.
Results
Of the women included in the latent class analysis, 37% never had any assessment and the remainder had had at least one assessment. After a steady uptake from 1999 to 2003, there was decline in uptake from 2003 onwards. A six-class model with sufficient homogeneity and reliable estimation was selected to represent assessment patterns and mortality risk, labelled as: ‘high mortality’ rate with little chance for assessment (12.4%), ‘intermediate mortality, low assessment’ (14.1%), ‘later mortality/low assessment’ (13.1%), ‘later mortality, high assessment’ (7.0%), ‘low mortality, low assessment’ (31.8%), ‘low mortality, high assessment’ (21.6%). Older women with certain conditions (such as diabetes, depression, heart disease) were more likely to be in the low assessment groups, and women with difficulty managing on income were more likely to be in low assessment groups.
Conclusion
Distinct assessment and mortality patterns were seen, with many women not having assessment, in particular those who had certain health conditions, were taking 3+ medications, had difficulty in managing on income, needed help or were in respite care, and had caring responsibilities. The findings point to a need to promote these assessments among older women, and to reduce financial barriers, even within the context of a heavily subsidized health care system.
Introduction
Decline in physical function is a common characteristic of older age, with important consequences for physical health-related quality of life, disability, depression, risk of falls, health care utilization, residential care, and mortality.1–5 Programmes to prevent functional decline frequently use comprehensive geriatric assessment and multifactorial interventions to prevent and manage health conditions, improve health risk behaviours, remove environmental hazards, and provide environmental and social supports.
The evidence for health assessment programmes has been reviewed by Stuck et al., 6 Cole, 7 Van Haastregt et al., 8 Byles, 9 and Elkan et al. 10 with discrepancies reported between studies in terms of the content and duration of the assessment, length of follow-up, and health benefits. Authors have variously concluded that the assessments have no effect, 7 positive effects, 9 , 11 and clinically insignificant effects. 10 Stuck et al. 6 concluded that assessments are effective, but that their effectiveness is dependent on having multiple follow-ups. Beswick et al. 12 concluded that geriatric assessments were associated with significantly better physical function.
Health assessments for older adults were introduced in Australia in 1999, and were subsidized through the Medicare Australia universal health insurance scheme. 13 The health assessments involve a structured, in-depth health check of people aged 75 years and over, to identify health issues and conditions that are preventable or amenable to interventions and may require further management. In addition, the health assessment may identify various factors that influence a person’s physical, psychological, and social functioning. 14 The evidence for establishing the health assessment programme in Australia was based on published findings from Europe and the United States,6–12 as well as a small trial undertaken in Australia, 15 and a large randomized controlled trial funded by the Australian Department of Veterans’ Affairs (DVA). 14 In the larger trial, health assessments were associated with small improvements in quality of life outcomes, but there was no significant difference in the probability of hospital admission or death. 14 It was expected that the assessments would be widely used as an opportunity to identify the health care needs of older people and provide preventive care.
Initial uptake of the Medicare subsidized health assessments in Australia was rapid. According to Wilkinson et al., 16 23% of the eligible population had an assessment within two years of their introduction, with higher use by people in the most socioeconomically disadvantaged quartiles. Gill et al. 17 estimated that 31% of all eligible older Australians had at least one Medicare claim for a health assessment in the first 35 months following their introduction. These assessments were more likely to be used by women, those aged 80–84 years, those living in urban and economically advantaged areas, and those entitled to treatment under DVA arrangements. An evaluation of the early uptake of the health assessments by women in the Australian Longitudinal Study of Women’s Health showed that by 2003, four years after their introduction, 49% of eligible women had received at least one assessment. 18 , 19 This current study aims to assess which older Australian women had Medicare subsidized health assessments between 1999 and 2013.
Methods
Study design
The study involved an analysis of prospective, longitudinal survey data for the 1921–1926 birth cohort of the Australian Longitudinal Study on Women’s Health (ALSWH),20–22 linked to administrative health data using deterministic linkage using personal identifiers and to the National Death Index. Ethics approval for ALSWH, including access to administrative data, was obtained from the human research ethics committees of the University of Newcastle and University of Queensland, and the Australian Government Department of Health. Access to the National Death Index was also approved by the ethics committee of the Australian Institute of Health and Welfare as the integrating authority.
Participants
Women were randomly sampled from the Medicare Australia data base, with deliberate over-sampling from rural and remote areas. 22 Medicare Australia is the national universal health insurer for all women who are resident in Australia. The women were first surveyed in 1996 (aged 70–75, N = 12,432), with follow-up surveys every three years: 1999 (aged 73–78 years, N = 10,434), 2002 (aged 76–81 years, N = 8647), 2005 (aged 79–84 years, N = 7158), 2008 (aged 82–87 years, N = 5561), and in 2011 (aged 85–90 years, N = 4055). Since October 2011, surviving women have been surveyed every six months. By 2013, 5215 older women were still returning six-monthly surveys. A small percentage (5.7%) of women completed surveys but did not provide consent for data linkage and were excluded from this analysis. Bias between ALSWH study participants and the general population is small, with the sample of women broadly representative of the national population of women in the target age groups. 20 , 22
Measures
Health assessments
Use of health assessments was ascertained from the Medicare Benefits Scheme (MBS) dataset (with specific items 700–707, 712, 715, 718, and 719 for 75 + health assessment). Medicare data includes information on date of service, number of claims for general practitioner, specialist attendances, other health services, and investigations subsidized under Medicare. For this analysis, women were classified as having had a health assessment ‘Yes’ for each year from 1999 to 2013 if any of these items were claimed. For each year during this period women who had not had a health assessment were coded as ‘No’.
Deaths
Fact and date of death were ascertained from the National Death Index. 23
Chronic diseases, health factors and medications
Chronic diseases and health factors included doctor diagnosed conditions at survey 2 in 1999 (corresponding to the time of introduction of assessments), coded as ‘Yes’ or ‘No’. These included diabetes, depression, anxiety, high blood pressure, heart disease, cancer, and other comorbidities (arthritis, stroke, thrombosis, low iron, osteoporosis, dementia, etc.).
We further included (i) common symptoms experienced within the past 12 months, such as leaking urine, vision problems, hearing difficulty, sleeping problems, falls or injuries, and any major surgery impacting health; (ii) medication usage, such as using more than three medications per day, taking medicines for nerves, sleep, depression, hormone replacement therapy (HRT), and for other chronic diseases; and behavioural risk factors, including alcohol consumption (non-drinkers and low- and high-risk drinkers); smoking (never, current, former); and body mass index (BMI, categorized according to the World Health Organization’s BMI classification of underweight – BMI <18.5, healthy weight – 18.5 ≤ BMI <25, overweight – 25≤ BMI <30, and obese – BMI ≥ 30). 24 , 25
Factors used to measure health care access and use included: number of visits to the general practitioner (GP) in the preceding12 months (classified as up to four visits, more than four visits), rating the ease to access GP of choice, and days spent in hospital over the last 12 months.
Sociodemographic factors
The sociodemographic factors included were: area of residence (metropolitan, regional, remote/very remote), marital status (partnered, not partnered), managing on available income (impossible/difficult, not too bad, easy), private health insurance, housing status (house/other, apartment, retirement village), needing help with daily tasks, receiving respite health services or other community services (food services, homemaking, home maintenance, counselling, social groups or support and advisory groups), and caring for a person with illness or disability.
Statistical analysis
Latent class analysis (LCA) was used to identify different assessment patterns, which are not usually observable in the data. In such cases, a mixture model is used which is a probabilistic model for representing the presence of unobserved subpopulations within an overall population. Finite mixture models are used to model the probability of belonging to each unobserved group, to estimate distinct distribution in each group, to classify individuals into the groups, and to draw inferences about how each group behaves. 26 LCA is a specific finite mixture modelling technique which identifies latent (underlying and unobserved) subgroups within a population based on individuals’ responses to one or multiple observed variables. 27 For our analysis, we used responses from one observed variable over multiple time-points; this approach is called repeated measures LCA. Results from the LCA model also provide the prevalence of each latent class and error associated with observed variables used in identifying the latent classes. 27 Based on three observed categories –‘no health assessment’, ‘health assessment’, and ‘deceased’ – for each year 1999 to 2013, women were assigned to classes that represented the dominant pattern over the observation period. Six latent class models were conducted (fitting two to seven latent classes) and results were compared. The selection criteria for the optimal, baseline model and, therefore, the best classification of the women into assessment patterns, were based on the principle of best model fit, parsimony and conventional fit statistics: Akaike’s information criteria (AIC), Bayesian information criteria (BIC), and entropy. 27 Labels were assigned to each latent class using the ‘item response probability’ and ‘latent class membership probability’. 27 Each latent class was graphically summarized using stacked bar charts to provide a simple and comprehensible way to visualize the class membership and validate the assigned labels. Class membership based on maximum posterior probability was retained; class allocation was treated as a known variable and then used in subsequent analysis and interpretation. Latent class analysis included 11,118 women who (i) survived to November 1999 (when assessments were introduced); and (ii) did not deny consent to data linkage under opt-out consent provisions.
To examine the impact of health and sociodemographic characteristics on latent class membership, analysis was further restricted to 9718 women who responded to survey 2 in 1999, and who did not have missing data on explanatory variables. Survey 2 variables were then incorporated in the latent class model using a ‘LCA with covariates – two-step approach’. 27 In the first step, variables were included as separate/univariate predictors in the latent model using a logistic regression framework, and producing an estimate of effect for each latent class in comparison to the reference latent class. 27 In the second step – the overall model – variables, which were statistically significant in step one (p ≤ 0.05) were added to the overall latent model. These two models (with and without covariates) were then compared by means of a likelihood ratio χ 2 test with the level of significance at p ≤ 0.05. The class ‘low mortality, high assessment’ was selected as the reference category as it represented the ideal pattern for older women.
SAS 9.4 was used to carry out the LCA procedure, which was developed by the Methodology Centre, Penn State University. 28 , 29
Results
Of the 11,118 women included in the latent class analysis, 4124 (37%) women never had any 75+ health assessment while 6994 (63%) women had at least one health assessment from November 1999 to 30 December 2013. Approximately 887 (8%) women had their first health assessment in the first year of its introduction, with a steady increase in the uptake of health assessments in the first two years. After 2002, there was a decline in the uptake of health assessments, with only 701 assessments in 2003 and 478 in 2004. There were only 142 and 103 assessments in 2012 and 2013, respectively.
Patterns of health assessment over time
An optimal six class model was chosen to adequately represent the data after considering the results of model fit statistics from seven possible models (see Table 1). Other models lacked sufficient homogeneity and reliable estimation based on values of AIC, BIC, entropy, and G2.
Model fit statistics for baseline latent models for evaluation of patterns of uptake of 75+ Health Assessment among 11,118 women born between 1921 and 1926.

AIC: Akaike’s information criteria; BIC: Bayesian information criteria.
Parameter estimates from the final, full prediction model for the patterns of the 75+ health assessment uptake for 9718 women, with ‘low mortality, high assessment’ class as the reference category for ‘LCA with covariates’.
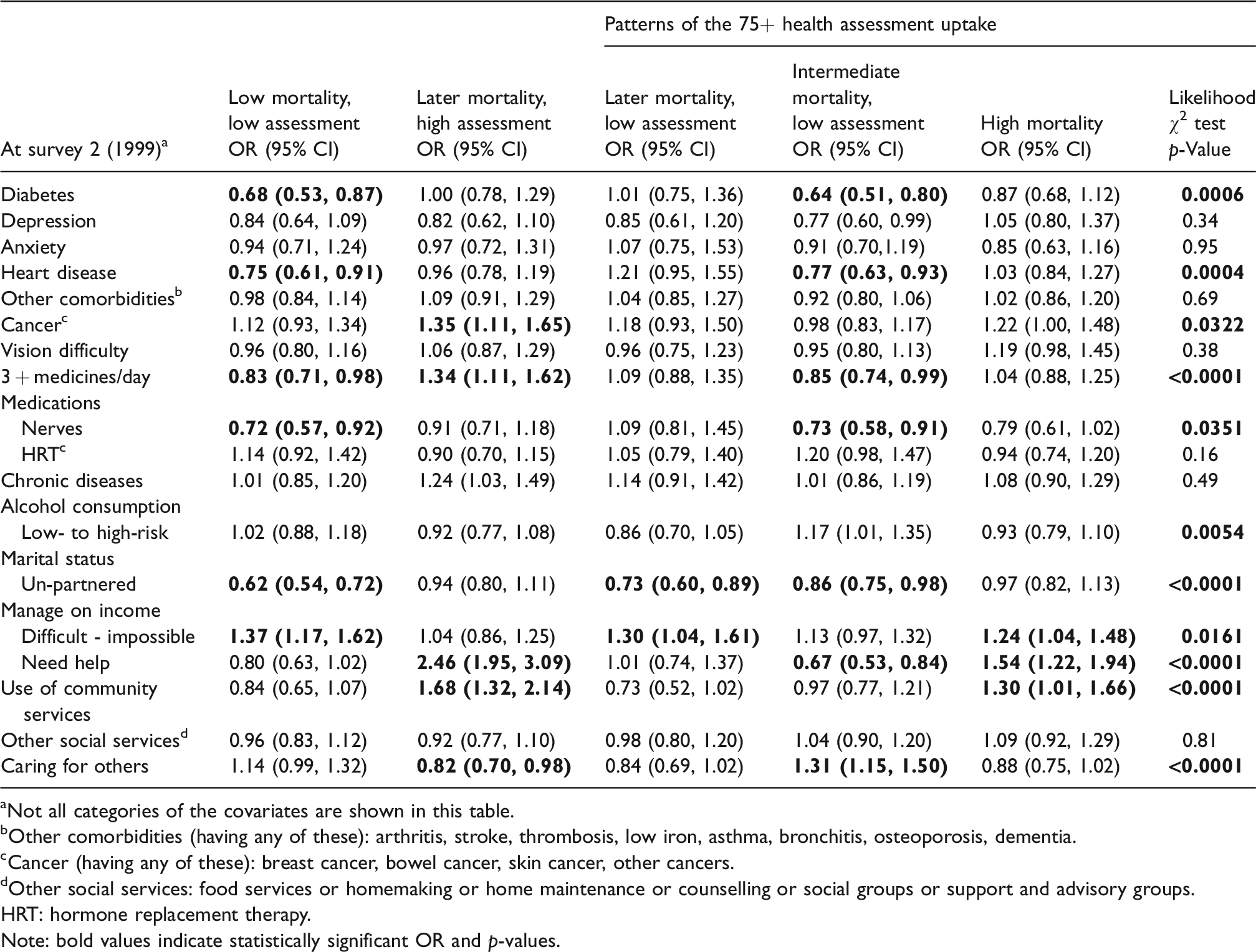
aNot all categories of the covariates are shown in this table.
bOther comorbidities (having any of these): arthritis, stroke, thrombosis, low iron, asthma, bronchitis, osteoporosis, dementia.
cCancer (having any of these): breast cancer, bowel cancer, skin cancer, other cancers.
dOther social services: food services or homemaking or home maintenance or counselling or social groups or support and advisory groups.
HRT: hormone replacement therapy.Note: bold values indicate statistically significant OR and p-values.
Figure 1 presents the item response probability of ‘having health assessment’, ‘not having health assessment’ and ‘death’ each year from 1999 to 2013, for each latent class. Of the 11,118 women, 1376 (12.4%) of women were classed as ‘high mortality’, with these women deceased by 2004. Very few of these women had health assessments in any year. Women classed as ‘intermediate mortality and low assessment’ (n = 1574, 14.1%) died between 2005 and 2007, but fewer than 20% of these women had an assessment in any year. The group classed as ‘later mortality, low assessment’ (n = 1462, 13.1%) died after 2008 and had a low probability of assessment, whereas the group classed as ‘later mortality, high assessment’ (n = 770, 7.0%) had a similar mortality rate but a much higher assessment rate. Women classed as ‘low mortality, low assessment’ (n = 3528, 31.8%) had consistently low probability of having health assessments from 1999 to 2013, with few deaths up to 2013, while women classed as ‘low mortality, high assessment’ (n = 2408, 21.6%) had a higher probability of health assessments.

Patterns of uptake of 75+ Health Assessments from 1999 to 2013 for 11,118 women born between 1921 and 1926.
Impact of health and sociodemographic factors on class membership
Prevalence of chronic diseases, health, and sociodemographic factors for the 9718 women with data for survey 2 are shown as per class membership in Appendix 1, Table S1 (online only). Table 2 presents the results of LCA with covariates, using ‘low mortality, high assessment’ as the reference group, women were less likely to be in the ‘low mortality, low assessment’ group if they had diabetes, heart disease, took more than three medications, and if they were unpartnered. They were more likely to be in the ‘low mortality, low assessment’ group if they found it difficult to manage on income. Women were less likely to be in the ‘later mortality, high assessment’ group if they had cancer, needed help with daily tasks and used community services; and less likely to be in this group if they were caring for others. They were more likely to be in the ‘later mortality, low assessment’ group if they had difficulty managing on income. Cancer, difficulty managing on income, needing help with daily tasks, and use of community services were all associated with being in the ‘high mortality’ group.
Discussion
This study identifies patterns of the uptake of Medicare subsidized health assessment items over a 14-year period (1999–2013) for Australian women born between 1921 and 1926, accounting for differences in assessment use over time, and survival. Around 12% of the women had a relatively high mortality rate and, therefore, would have had less opportunity to have health assessments compared to other women. Comparing women with similar mortality profiles shows few baseline differences between those with higher and lower assessment rates.
This work builds considerably on previous research,16–18 which reported uptake rates of 23% to 49% for the 75+ health assessment in the first 24 to 48 months after its introduction. Data from the ‘45 and Up Study’ 30 showed that 41% of their sample of men and women aged 75+ years had received a health assessment in the year following their entry into the study (between 2006 and 2009). Also, health assessment occurred less frequently for people with higher educational attainment and household income, but more frequently for those of older age, with more comorbid conditions and greater physical limitation. 30
Our findings indicate a much lower rate of health assessment uptake (7.9%) by women in the first year of its introduction. Recent work by Hamirudin et al. 31 reported that people aged 75–84 years were more likely to take up the assessments compared to those 85 years and over. However, the current study did not specifically examine assessment rates for women of different age categories.
This cohort of older women was the first to become eligible for the annual health assessments. The findings from this study show that regardless of women’s health status or sociodemographic characteristics, overall assessment rates tended to be low. Soon the ALSWH 1946–1951 cohort (mid-age cohort) will also reach the health assessment eligibility age of 75 years. However, a recent ALSWH report on health services use indicated that middle age women (the future ‘old’ cohort) will have patterns of health service utilization similar to the current ‘old’ cohort when they reach older age. 30 , 32
Some health conditions were associated with class membership. Women with certain health conditions (for example: diabetes, depression, anxiety, heart disease) were more likely to be in ‘low assessment’ groups. These women may have more contact with their family physician, and therefore more opportunity to have an assessment, as well as a greater identified need for comprehensive assessment of their health care needs. In our earlier study, 18 we found a significant association between the number of visits to GPs and health assessments. This finding is in line with other work that found that often people who came to assessments were healthier than those who were unwilling to have assessments in a clinical setting. 33 , 34 Physicians may recommend the health assessments to patients with existing health issues or those who are in respite care or need any help, to benefit from these systematic health assessments. 35
Financial issues may also be a major factor determining some women’s uptake of health assessments. 34 In Australia, although health care costs are subsidized through the Medicare universal health insurance scheme, many practitioners charge above the scheduled fee, with patients paying out-of-pocket costs. The Australian Bureau of Statistics’ Patient Experience Survey 36 reported that cost is a reason that many people may delay seeing doctor.
This finding points to an opportunity to promote health assessments among older women, and through their doctors, with the potential to improve health outcomes in later life. Comprehensive assessment and multifactorial interventions to prevent and manage health conditions, improve health risk behaviours, remove environmental hazards, and provide environmental and social supports have been found to be effective in maintaining physical function and reducing admission to hospital and residential care. 12 The effects are also most pronounced for ‘young–old’ people and those with a low risk of death, and are dependent on multiple follow-ups. 6
Strengths of this study are the large sample size and the study’s ability to link baseline data on mortality, health and sociodemographic characteristics for each woman. We have provided a new dimension to previous studies by examining patterns of uptake over a 14-year period, assessing women’s use of these assessments as they aged. These effects could not be ascertained from cross-sectional data. A limitation of this study is that some women did not provide consent to data linkage. However, this proportion is small. We were not able to assess the role of practice nurses or GPs in carrying out these assessments. We were also not able to compare the uptake of assessments by gender.
Conclusion
Across a large sample of women, there are distinct patterns of assessment uptake, with many women not having health assessments. Few other factors differentiated between groups, although women with certain conditions were less likely to be in the low assessment groups, and women with difficulty managing on income were more likely to be in low assessment groups. The findings point to an opportunity and need to promote health assessments among older women, and to reduce financial barriers, even within the context of a heavily subsidized health care system. Visits to the family physician can be an opportunity to promote regular health assessment as a key means of reviewing health and care needs in later life.
Supplemental Material
Supplemental material for Patterns of geriatric health assessment use among community dwelling older Australian women over a 14-year period
Supplemental Material for Patterns of geriatric health assessment use among community dwelling older Australian women over a 14-year period by Tazeen Majeed, Meredith Tavener, Xenia Dolja-Gore, Balakrishnan Nair, Catherine Chojenta and Julie Byles in Journal of Health Services Research & Policy
Footnotes
Acknowledgement
The research on which this paper is based was conducted as part of the Australian Longitudinal Study on Women’s Health by the University of Queensland and the University of Newcastle. The authors are grateful to the Australian Government Department of Health for funding and to the women who provided the survey data. They also acknowledge the Department of Health and Medicare Australia for providing the MBS data. They acknowledge the Australian Institute of Health and Welfare (AIHW) as the integrating authority for these data. They acknowledge the assistance of the Data Linkage Unit at the Australian Institute of Health and Welfare (AIHW) for undertaking the data linkage to the National Death Index (NDI). The authors would also like to acknowledge and thank the support of Priority Research Centre for Generational Health and Ageing and Hunter Medical Research Institute in providing the infrastructure and support for this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
Ethics approval was granted for each stage of the study by the University of Newcastle and the University of Queensland. Approval was also granted by the Department of Health and Ageing for the use of the MBS data, and the AIHW ethics committee approved the creation of data linkage keys.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.