
Abstract
Objectives
In Canada, the rural elderly population is increasing in size, as is their need for palliative care services in these settings. This analysis aims to identify awareness-associated barriers to delivering rural palliative care services, along with suggestions for improving service delivery from the perspective of local health care providers.
Methods
A total of 40 semi-structured interviews with various formal and informal health care providers were conducted in four rural and/or remote Canadian communities with limited palliative care resources. Interview data were thematically coded using Penchansky and Thomas’ five dimensions of access (i.e. availability, (geographic) accessibility, accommodation, acceptability and affordability). Saurman’s recently added sixth dimension of access – awareness – was also identified while coding and subsequently became the primary focus of this analysis.
Results
Identified barriers to palliative care awareness and suggestions on how to enhance this awareness, and ultimately palliative care delivery, corresponded with three key themes arising from the data: limited palliative care knowledge/education, communication and coordination. Participants recognized the need for more palliative care education, open lines of communication and better coordination of palliative care initiatives and local resources in their communities.
Conclusions
These findings suggest that identifying the barriers to palliative care awareness in rural communities may be foundational to addressing barriers to the other five dimensions of access. A thorough understanding of these three areas of awareness knowledge, communication and coordination, as well as the connections between them, may help enhance how rural palliative care is delivered in the future.
Introduction
Over the past 30 years, various frameworks have attempted to conceptualize health care access, and have explored the meaning and concept of access in a number of ways.1,2 Despite advancement in this area, consensus on a concise universal definition of health care access and the appropriate measures for evaluating its progress have yet to be achieved.3,4 Penchansky and Thomas 5 were among the first researchers to propose a model for access to health care, which they defined as the ‘fit’ between a patient’s characteristics and expectations, and those of their providers or health care system. They theorized that health care access could be divided into five dimensions: affordability, (geographic) accessibility, accommodation, acceptability and availability.
These dimensions are comprehensive, interconnected, and have been used as a guiding framework for a wide range of studies6,7 exploring health care access within various contexts and populations. 3 According to Penchansky and Thomas, all five dimensions should be equally balanced and function in harmony if optimal access to care is to be achieved. It is only very recently that another scholar, Saurman, who considered this framework to be useful but incomplete, identified an additional dimension – awareness – for assessing whether access has been achieved. 8 Saurman evaluated access to an emergency mental health care programme and found that interviewed patients and providers demonstrated a poor awareness of the programme’s existence, purpose and target population, despite displaying sufficient evidence of access in other ways.9,10 Upon reflecting on these findings, Saurman 8 stated that ‘a service maintains awareness through effective communication and information strategies with relevant users (clinicians, patients, the broader community), including consideration of context and health literacy’ (p. 37). Ultimately, Saurman 8 proposed that awareness might greatly improve our ability to enhance health care access for all and should be applied as a sixth dimension whenever the original five dimensions are used to ‘develop, implement, or evaluate health care services and understand issues of access more generally’ (p. 38).
Access to health care is particularly challenging in rural settings. 11 While definitions of rurality vary, for the purpose of the study described below, ‘rural lands’ or ‘rural areas’ are defined by the OECD as geographic areas with a population density less than 150 people per square kilometre. 12 Taking into consideration Canada’s aging demographic, of which a large proportion reside in rural areas, it is no surprise that greater attention has been placed on palliative care services in recent years. 13 Palliative care is generally understood to be a health service that provides symptom and pain management, as well as emotional, social, and spiritual support to terminally ill clients who seek comfort at end-of-life. 14 Unfortunately, access to palliative care is inconsistent across Canada, especially among those residing in rural settings who, unlike urban residents, encounter additional geographical (e.g. distance to facility) and financial (e.g. cost of transportation) barriers to care. 15 As the percentage of the aging population in rural Canadian communities continues to grow, the delivery of high-quality palliative care services in these areas will become a greater priority for health care providers (HCP) and their clients.13,16
The purpose of this paper is to explore HCPs’ perceived barriers to delivering palliative care in four rural Canadian settings and to document suggestions for improvement that they have identified as helping to address inadequate access to palliative care in these regions. Although these HCP perspectives are analysed using Penchansky and Thomas’ five dimensions of access as a framework, this paper primarily focuses on Saurman’s proposed sixth dimension – awareness – to further our understanding of access to care in this area. A greater understanding of awareness as a dimension of access may not only provide new insight into barriers to rural palliative care delivery, but also into how the original five dimensions influence palliative care access in these settings.
Methodology
Study design
This analysis utilizes transcribed interview data from a mixed-methods pan-Canadian study that identified rural communities in need of additional palliative care services. The first phase of the study refined a quantitative model for siting secondary palliative care hubs (SPCH), designed to assess the suitability of implementing new palliative care services in rural communities across Canada. The model considered the following factors for each community: population (i.e. community size), isolation (i.e. travel time to nearest palliative care service provider), vulnerability (i.e. community residents over the age of 65 years old) and community readiness (i.e. palliative care visibility). 17 The model identified and ranked a total of 20 communities with inadequate palliative care services yet with suitable community infrastructure and interest in developing these services, from which four communities were purposefully selected for the second phase of the study. In this phase, community case studies involving semi-structured interviews with HCPs were undertaken. 18 The purpose of the interviews was to gain a greater understanding of HCPs’ perspectives concerning suitability and responsiveness to SPCH services, as well as their experiences with providing palliative care. The questions featured in the interview guide captured rich qualitative data amenable to several analyses,18–20 including this investigation of barriers and suggestions for enhancing access to rural palliative care.
Data collection
The four communities (see Table 1) were considered ‘rural’ according to the OECD definition and ranked highly in the SPCH siting model results. 12 Forty semi-structured phone interviews were conducted in 2014 (10 per community) with six informal HCPs (e.g. family caregivers) and 34 formal HCPs (e.g. nurses, social workers, programme managers) who delivered or coordinated palliative care. Given that formal and informal palliative care expertise differed between communities, a target ratio for recruitment was not set. Participant recruitment involved sending invitations to existing community contacts, as well as publishing invitations in print and online, through newspapers, newsletters, and bulletins. Throughout the interview process, investigators attempted to recruit voices/sectors that were not yet consulted. To enhance consistency, one investigator was responsible for conducting phone interviews. All recorded and transcribed interviews were imported into NVivo™ qualitative data management software.
Community characteristics.
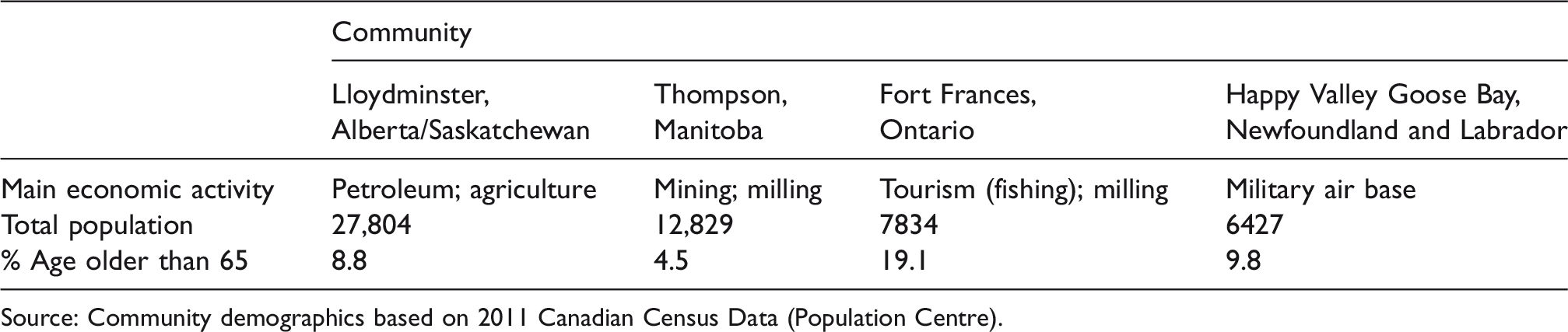
Source: Community demographics based on 2011 Canadian Census Data (Population Centre).
Data analysis
A thematic analysis was conducted, where interview data were coded and grouped to identify emerging patterns and themes. 21 Prior to coding, study investigators agreed to using the five dimensions of access as a framework for guiding the analysis. During the coding process, a sixth dimension emerged – awareness – and the team reconvened to discuss the inclusion of a novel sixth dimension. During this time, Saurman’s paper 8 on this additional sixth dimension (awareness) was published. In considering the established literature on the utility of Penchansky and Thomas’ five dimensions of access, we were led to focus on exploring whether ‘awareness’ had applicability in our study. To assess its applicability and enhance qualitative rigour, four transcripts were selected and reviewed independently by three team members. Once consensus on applicability and interpretation across investigators was achieved, the thematic analysis was undertaken. The first author was responsible for leading the coding and analysis process and had regular consultations with other team members for feedback and guidance. While participants provided much insight into Penchansky and Thomas’ five dimensions, our specific interest in exploring the suitability of Saurman’s recently added sixth dimension of ‘awareness’ encouraged a more thorough analysis of data coded into this theme.
Research findings
Findings of this analysis revealed three themes, which highlight HCPs’ perceived barriers to rural palliative care delivery, and suggestions for enhancing delivery via awareness: (a) palliative care knowledge/education; (b) palliative care communication; and (c) palliative care coordination.
Palliative care knowledge/education
Participants with varying levels of palliative care knowledge and expertise aspired to meet the needs of their palliative care clients/family members/friends. However, inadequate access to palliative care support within all four communities has cultivated knowledge gaps and poor awareness in palliative care among participants despite having responsibilities to provide or manage this type of care. Furthermore, many participants recognized that educational and training opportunities, which could enhance palliative care knowledge, were limited and often involved travel. As a result, formal HCPs would rely on each other for support, as one participant described: There hasn’t been a lot of education with regards to palliative, like we usually draw on each other you know, either one has a strength with palliative, someone else is cardiac, someone else is [paediatrics], so you know we just rely upon each other whenever there is a palliative client. (Happy Valley-Goose Bay participant) When I first arrived here I was trying to find access to … services … kind of … a guide where it says, you know, like what kind of services are being offered and there really doesn’t seem to be anything like that. (Fort Frances participant) We definitely need more people trained in palliative care itself cause a lot of people are afraid of it I think, like they go in and somebody’s really sick, oh I don’t want to look after them cause they’re dying, you know what I mean, we need more training I believe. (Happy Valley-Goose Bay participant)
Communication
While participants felt that strong communication between HCPs, their clients, and health care administration was an essential component of palliative care awareness, effective lines of communication were currently lacking within their communities. Communication between HCPs was often considered inadequate and inconsistent, especially between providers who delivered care in different settings. Miscommunication and poor feedback between providers often resulted in poor continuity of care for clients who travelled out of town for palliative services. One participant shared: I think it’s just the whole communication between providers who are working for different organizations or agencies; it’s a big challenge kind of figuring out or knowing who is doing what and who is responsible for what and who communicates when you know the patient’s condition changes or if they’re hospitalized and then discharged you know? Do the home care workers know that that happened or not? Yeah, so it’s communication, [it] is a big challenge even in smaller communities. (Fort Frances participant)
Participants observed that communication between formal and informal HCPs and clients was often the strongest when a long-term relationship was established. Some participants noted that providers who delivered general care to a specific client for at least a few years prior to switching to specialized palliative care, fostered an open and honest communication line between their clients about the care they delivered: The familiarity with, with us, I mean people, or patients have been with us from diagnosis through to the end you know…and they’re comfortable with us…. (Happy Valley-Goose Bay participant)
Participants often considered communication between HCPs and health care administration to be complex and bureaucratic, particularly when urban, provincial or federal priorities did not line up with rural, local or regional priorities. Open communication was frequently cited as necessary for resolving the apparent disconnect between, for example, community and provincial priorities: [O]ftentimes … the capital of the province doesn’t always understand the needs of being in northern communities and in rural communities …there has to be a lot of open communication and dialogue in trying to understand the needs of those who live in the north and really people who live here are the ones who can best describe what, what needs to be here…. (Fort Frances participant) The fact that we’re on the Saskatchewan/Alberta border, the hospital [is] in Saskatchewan, so there’s a lot of arguments between the two [provincial] ministries to decide where the money goes and how they pay…. (Lloydminster participant)
Coordination
To participants, improving awareness about palliative care also meant there was a need to create effective coordination of knowledge, services and resources. Doing so would compel HCPs to share palliative care expertise, identify and address palliative care gaps in their community, and ensure that clients receive palliative care in their environment of choice. However, many participants believed poorly coordinated services in their respective community had removed a client’s ability to choose their preferred place of death. HCP networks bridging palliative care specialists and allied health professionals were broadly stated to be inadequate or non-existent. As a result, a fear of delivering or receiving care at home, where palliative care equipment and services were more difficult to access than in hospital settings, was identified as a concern: ‘I think people are fearful to have someone who’s dying come home and afraid that, you know, they might speed up that process by having them discharged from the hospital’ (Thompson participant).
Participants across all four sites viewed having a palliative care coordinator to organize services, arrange palliative care training and education sessions, and run palliative care programmes as one way to prioritize palliative care in their community. Although a palliative care coordinator was currently located in all four communities, albeit with varying responsibilities and scopes of practice, some participants acknowledged past challenges in identifying a palliative care focal point when coordinators were absent. Some participants thought efforts to improve palliative care awareness could be cultivated with reference to a physical structure, such as a hospice, with centralized palliative care resources, whereas others believed that an individual who could take the lead on palliative care initiatives was required.
Participants indicated that inadequate coordination between local HCPs and the health care administration has led to several programmes addressing similar or overlapping objectives. Moreover, federal and provincial mandates on palliative care were thought to rarely consider unique community contexts, and have left participants feeling frustrated and disconnected. One participant described a few jurisdictional differences within Labrador clearly: … I mean every community is different, even the challenges on the north coast as I said with the community health nurses being under the Nunatsiavut government [self-governing Inuit regional government] as opposed to all the staff, the health care, the regional nurses being under Labrador-Grenfell Health [regional health authority] is completely different than in the south of Labrador where both the community health nurses and the regional nurses are all under Labrador-Grenfell health, so different pockets have different I guess strengths and weaknesses and different things that they need to overcome. (Happy Valley-Goose Bay participant) … people need to be brought together both from the areas and the regions and the funders to hear if they really want to know what people feel serves the communities best then they should be meeting at least regionally with the clients they hope to serve…. (Thompson participant)
Discussion
Participants in our study discussed similar access barriers to rural palliative care – according to Penchansky and Thomas’ five dimensions of access (i.e. availability, (geographic) accessibility, accommodation, acceptability and affordability) – as those identified in past literature.22–24 However, the focus of this analysis was on Saurman’s newly identified sixth dimension: awareness. Our analysis of awareness in the context of palliative health care access reveals thematic findings that suggest palliative care knowledge, communication and coordination are key components for creating palliative care awareness. These three components resonate with Saurman’s definition of awareness – communication and information – as well as previous studies implicitly highlighting how awareness, specifically in rural palliative contexts, can influence access to care.23,25,26 For example, one study exploring the personal and familial experience of rural palliative transitions found that clients felt ill-informed due to limited and insufficient communication between themselves and providers. 25 Optimizing these three components of palliative care awareness may improve provider competence in delivering care, as well as client expectations when receiving care.
Our participants noted that rural HCPs tend to be generalists, fulfilling a wide range of responsibilities with occasional assistance from specialized colleagues when needed; this has also been found elsewhere. 23 Despite receiving advice and guidance from palliative care specialists, many participants felt uncomfortable and ill prepared to deliver palliative care, and cited an absence of local training opportunities in palliative care as justification for their lack of competence. Both our participants and previous research have indicated that palliative care workshops, delivered locally and tailored to the social and cultural context of each community, will help meet this need and ultimately improve palliative care awareness among providers. 27
Study participants also acknowledged the power of communication and its ability to influence the level of palliative care awareness among clients and providers. Our findings suggested that inadequate communication not only hindered a provider’s ability to inform clients of palliative care services but also prevented knowledge sharing between colleagues. Our thematic analysis in this area suggested that frequent and clear communication was an important component of awareness, and necessitates that HCPs are listening to client requests, collegial feedback and the palliative care vision of their community.
Finally, participants believed that efficient coordination between HCPs, their clients and health care administration would help address many long-standing gaps in access to rural palliative care. While this is not a unique challenge facing rural palliative HCPs, many participants in our study hoped to see greater emphasis placed on acknowledging the physical, social and economic contextual factors that make rural settings and their residents different from their urban counterparts. Moreover, inadequate coordination can complicate administrative procedures, particularly when dealing with multiple or overlapping jurisdictions, as was the case for Lloydminster. Participants suggested that streamlining services into a connected and coordinated system could help identify community strengths, facilitate administrative duties (i.e. paperwork and transferring medical results), and organize local resources; their recommendations were congruent with those found elsewhere.22,24
Our findings suggest that ‘awareness’ is an important dimension when evaluating access. According to our findings, community awareness may increase if palliative care knowledge is provided (e.g. workshops, courses, peer support). Communication between providers and their clients can facilitate the transfer of palliative care knowledge, and allow clients to share their palliative care needs and how to address them. It is through clear communication that effective coordination of palliative care services can then take place. In a sense, by increasing palliative care awareness through knowledge sharing/training, communication and coordination, HCPs and the institutions they work for may have a greater capacity to address barriers to the other five dimensions of access. For instance, enhancing palliative care awareness may facilitate the efficient distribution of physical and financial palliative care resources in the community, and make these services more acceptable and physically accessible to clients. Given that Saurman’s study was recently published, very few studies have evaluated the newly proposed sixth dimension – awareness – within the context of the original five dimensions,10,28 and none have been conducted within a rural palliative care context. Thus, additional research applying ‘awareness’ along with the other five dimensions of access to different palliative care studies would meaningfully contribute to our understanding of rural palliative care access.
It is interesting to note that while this study featured a variety of formal and informal HCPs, there were no consistent similarities or differences among shared perspectives according to participant role. At the same time, this study did not seek to provide a comparative analysis across participant groups or study sites. As a result, our ability to examine participant insights according to their role is limited. It is also possible that other participant groups, if recruited, may have provided additional perspectives that differed from those shared in this study. Although this can be considered a limitation of any qualitative study, it also presents the opportunity for future research to confirm or expand these findings with other stakeholder groups (e.g. health care administrators).
Conclusion
While access to health care is considered a basic human right, 29 it is not always guaranteed. Maintaining good health towards the end-of-life without accessible and effective palliative care is a challenging endeavour, not only for rural Canadian communities but for international rural communities as well, and thus calls for innovative solutions. Our findings indicate that HCP perspectives on barriers to, and suggestions for improving, palliative care awareness are helpful for increasing our understanding on access to palliative care services in these settings and, therefore, strongly support Saurman’s proposition that ‘awareness’ be integrated into Penchansky and Thomas’ theory of access. Our findings also highlight the importance of prioritizing palliative care awareness within rural communities, alongside the original five dimensions, to better address barriers to palliative care delivery in these settings. Formal and informal rural HCPs, along with health administrators and policy-makers, who consider the implications of palliative care knowledge, communication and coordination in their practice, programmes and policies may possess a good understanding of what is available in their community and how best to meet the needs of their clients. Thus, future research should explore initiatives that bridge the gap between these three components of awareness, in hopes of achieving palliative care access for all.
Footnotes
Acknowledgements
The authors gratefully acknowledge the research participants who made invaluable contributions to this study, as well as the constructive feedback and comments provided by those who agreed to review our manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.