
Abstract
Objectives
The paper reports on an empirical study of Health and Wellbeing Boards (HWBs) in England. Established by the Health and Social Care Act 2012, HWBs act as place-based hubs for leaders in health, social care, local government and other sectors to come together to address health improvement and the wider determinants of health.
Methods
We conducted a three-year study of HWBs (2015–2017) in five localities across England. This involved collecting qualitative data from semi-structured interviews with key actors in the HWBs at strategic and operational levels, and focus group sessions with voluntary-sector participants at each HWB.
Results
HWBs have largely followed the path of previous partnerships in terms of a lack of clear aims and objectives, lack of ownership and accountability by partners, and an absence of any significant impact on health outcomes.
Conclusions
Many of the features of unsuccessful partnership working were largely displayed by HWBs. Boards require more executive power and ownership from the bottom up if they are to have any real impact.
Introduction
This paper reports on a study conducted between January 2015 and October 2017, funded by the NIHR Department of Health (now Department of Health and Social Care) Policy Research Programme. The overall aim of the research was to evaluate the leadership role of Health and Wellbeing Boards (HWBs) and how well they were functioning to improve health and wellbeing and reduce inequalities, promote integrated service provision between health and social care, and facilitate collective decision-making, in addition to extending democracy locally.
The focus of this paper is to determine how, if at all, HWBs differ from previous partnerships or if it is case of, as Einstein is attributed to have said: ‘The definition of insanity is doing the same thing over and over again and expecting a different result.’ 1 Working in partnerships is regarded as being central to contemporary public policy, most notably since the late 1990s with the advent of New Labour. The allure of partnership continued under the Coalition government, with Cameron noting: ‘The Coalition government, elected in 2010, continued … with a greater emphasis on joint working as a strategy to reduce public spending.’ 2 The continuing appeal of partnerships lies in the fact that few challenges facing government, nationally and locally, fall neatly within the confines of a single organization, department or sector. This is especially true of the majority of challenges facing health, in particular public health, which are cross-sectoral in nature and embrace multiple policy arenas, organizations and professional groups. 3
The Coalition government’s health care reforms, enshrined in the Health and Social Care Act 2012 (HSCA 2012), entailed major structural changes to the health system in England. With the lead role for public health passing to local government in England, HWBs were designed to act as place-based hubs to ensure effective partnership working and, through the reforms, join up what was becoming an increasingly fragmented system. 4 This paper focuses on the role of HWBs, reviews the evidence on health partnerships and how it was hoped HWBs would learn from this. The paper explores two key questions on the progress and impact of HWBs and how they differ from previous partnership arrangements.
The role of HWBs
During 2010, the Coalition government published two White Papers on the NHS and public health respectively: Equity and Excellence: Liberating the NHS appeared in May, 5 and in December Healthy Lives, Healthy People: Our strategy for public health in England. 6 Part of the first White Paper’s rationale was to strengthen the role of local government in local health services in England and Healthy Lives, Healthy People elaborated on the role of HWBs. The subsequent HSCA 2012 with the decision to return public health to local government, after being located within the NHS since 1974, was broadly welcomed7–9on the grounds that public health would be better placed to tackle inequalities in health and the wider social determinants of health by adopting a strong population focus in place of a narrow one on health service provision.10,11
When they appeared in 2012, HWBs were meant to be a different kind of partnership. 4 And it is certainly the case that they have defining features that make them different from other health-based partnerships. For instance, they are place-based through being located in local authorities and are statutory, which means they are enshrined in legislation and cannot be completely ignored or disbanded (as many other partnerships have been). With the move of public health into local government, this offered a real opportunity for boards to act as a hub, bringing together interests such as public health, housing, planning, social care and education. These were to work together as part of the same organization, operating under the same broad frameworks with scope for strategic and operational linkages for the greater integration of policies and targets to improve local population health.
However, the wider structural changes to the health system arising from the HSCA 2012 caused significant disruption and fragmentation at the time of HWBs’ inception. 4 In an effort to overcome some of these challenges, the HSCA 2012 placed a statutory duty on local authorities to each create a HWB as a committee of the local authority to act as a place-based strategic hub to bring various partners together.
HWBs have a statutory responsibility for the Joint Strategic Needs Assessment, which is used to agree combined action at a local authority level with a statutory responsibility to produce a Joint Health and Wellbeing Strategy (JHWS). 12
After existing for almost two years in shadow form (that is, operating before becoming a statutory legal entity), HWBs became fully operational in April 2013. In an effort to ensure that HWBs would succeed through suitable adaptation to their local contexts, guidance from the centre on what HWBs should look like and how they should operate was kept to a minimum. 4
The evidence on health partnerships
It was hoped that HWBs would learn the lessons from previous and, judging by the evidence, largely ineffectual partnerships and initiatives focused on tackling the wider determinants of health and health inequalities, such as Health Action Zones.13,14 Literature reviews of the evidence on public health partnerships13,14 found there was little evidence to suggest that they led to better health outcomes for local/target populations or reduced health inequalities. Factors in building and maintaining good partnerships in most of the literature include good relationships, gaining trust and having clear aims and objectives to foster desired outcomes.13–16 A rapid literature review highlighted the main determinants of successful public health partnerships and the main barriers to success: 17
Determinants of successful partnerships
Clarity regarding the goals and objectives of the partnership Evidence of goodwill and trust between partners, particularly at the frontline level A clear strategic commitment to performance through robust monitoring and evaluation.
Barriers to effective partnership working
Conflicting agency priorities, which serve to negate or limit the potential of the partnership Lack of vertical as well as horizontal linkages between partners, i.e. absence of ownership Excessive bureaucracy, making participants susceptible to becoming focused on processes rather than outcomes.
HWBs: a different kind of partnership?
Early studies of HWBs suggested that they displayed a number of features that could differentiate them from previous partnerships, namely: involvement and engagement of GPs; wider relations between NHS and local government (not just social care); ensuring local populations can contribute to decisions about their services, partly through the contribution of HealthWatch and the voluntary sector; and opportunities due to the move of public health into local government and better accountability and governance due to being a sub-committee of the local authority.15,16,18
In the light of findings from previous studies, we seek to determine:
To what extent have HWBs operated differently to previous partnerships in tackling the wider determinants of health and how much ownership is there of the JHWS among partners?
In terms of HWBs being different from previous partnerships, given their local government base and links with clinical commissioning groups (CCGs) and local groups:
2. How far have HWBs strengthened collaboration, trust, goodwill and linkages between partners horizontally (across organizations including CCGs) and vertically (with agencies ‘on the ground’ such as HealthWatch and the voluntary sector)?
Methods
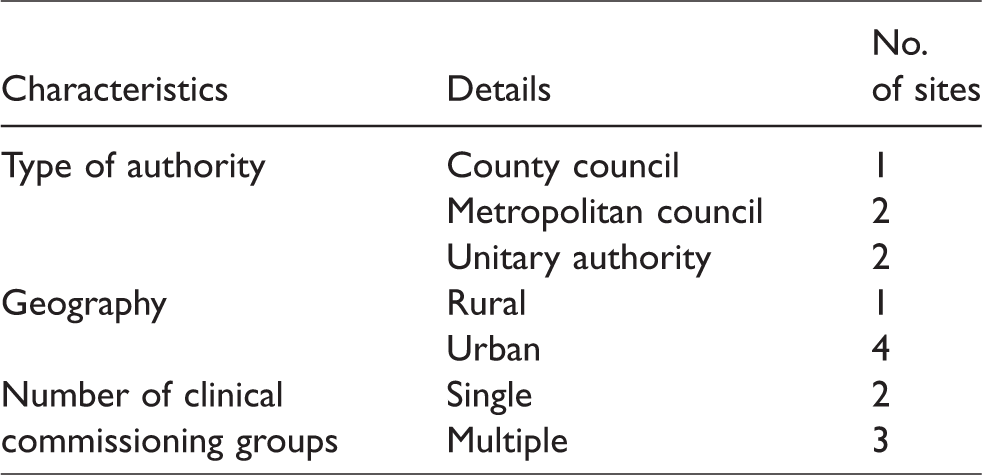
Data were collected from in-depth case-study fieldwork conducted at five local authorities (termed ‘sites’). Sampling criteria for the five case studies included geographic location, type of authority, political affiliation, urban/rural setting, and population size (see Table 1).
Case study sites.
There were initial interviews (n = 57) primarily with HWB members conducted between October 2015 and August 2016, and follow-up interviews conducted between November 2016 and February 2017 (n = 22). Focus groups (n = 5) were conducted with voluntary-sector organizations at each site.
In terms of analysing the data, initially this was undertaken by visual and diagrammatic methods, which were used alongside text-based methods, to assist in mapping local configurations and roles in HWBs. This process took place during five one-day workshops involving all members of the research team to undertake analysis of one case study site per workshop. Analysis of the data was also conducted using NVivo. A framework analysis approach was adopted, which identifies key issues and concepts through a thematic approach to the data analysis, informed by the interview schedule and subsequent analysis of the interview transcripts. 19
The analysis was first conducted at a within-case level to integrate and triangulate data in order to holistically describe the composition and function of the HWB within each site. Cross-case and longitudinal comparisons (constant comparisons) were then conducted across the sites to illuminate key contextual factors that shape the likely impact of HWBs as system leaders in facilitating health improvement, as well as whether and how these factors have changed over time.
Results
This section reports on the findings from the five case studies and is structured around the two questions listed above.
To what extent have HWBs operated differently to previous partnerships in tackling the wider determinants of health and how much ownership is there of the JHWS among partners?
Looking first at whether HWBs have operated differently from previous partnerships, respondents at all five sites argued that partnerships needed clear goals on what was to be achieved, with buy-in at all levels, from the strategic level downwards. However, respondents said that in practice this was predominantly not the case, with very little buy-in or commitment to strategies and goals. Rather, agencies had their own priorities, characterized by HWBs lacking strategic direction. The HealthWatch Chair in site 2 and a Director of Public Health in site 5 considered the lack of focus and poor system leadership in these terms: I think this thing of lack of direction runs throughout. Different people have different ideas and we don't have a single idea of what the board is. The board is … not itself a system leader … I wouldn’t describe [it] as being itself focused, the place where system leadership happens. I really do think that there hasn’t been a clear strategy for a while for the board, and what we had wasn’t enough to give the board purpose. There’s work being done in a new strategy; however, that was always intended to happen at the health and wellbeing operations group but appears to have now been pulled together by public health, and then passed through again. So, actually, even the strategy now is being done elsewhere with a few individuals and coming back to the health and wellbeing board to get signed off. What’s its added value, what’s its governance? People report in and say, ‘Oh, we’re doing this, that and the other, so what difference does it make, because most of that was going to happen anyway.’ It’s not that the board has added something to it or has more accountability. Because of the way it’s set up, it’s not going to do that. We've got the wellbeing … strategy. In the year that I've been attending the board, we have not once referred to it. Nothing that's come has been linked to it. Give us some good existing stuff that you’re doing that we perhaps as a wider partnership need to be aware of, that we’re not aware of, that we need to categorize more on, or we need to scale up citywide or whatever, as well as saying there’s a huge gap here. One huge gap, to give you an example, it might not directly fit in with our priorities and it’s not unique…I think most public agencies probably fail some pretty vulnerable teenagers. … it's all motherhood and apple pie. You know, we want people to eat well; come on, what we going to do about it? Let's have safe pavements/no drinking after midnight strategy. Let's have a sugar tax in our supermarkets. We've got a low alcohol initiative but has that really been landed well? So I think the purpose of the Health and Wellbeing Board should be to take that strategy document and make it real.
It was argued that there was difficulty engaging partners such as the acute trust, who were dealing with their own priorities. Links with education, housing and the police were also seen as requiring improvement. It was observed that Children’s and Community Safety Partnerships were struggling with a systems approach to partnership working in site 3.
In addition, the JHWSs across the sites had not engendered ownership by partners As this HWB Development Lead Officer in site 2 discussed: I don’t think they [the HWB] engage enough with the … strategy … other than through if you like semi-briefings from … [the Director of Public Health] in their more formal structures, and I actually think that collectively we could offer a lot more.
Overall, the study sites had largely followed the same process as previous partnerships and had not capitalized on having good attendance from board partners. Previous health partnerships had been characterized by a lack of commitment from key players.
13
With all key partners attending HWBs it was hoped that more progress could have been made. As observed, across the sites the impact of boards on tackling the wider determinants of health and reducing health inequalities through the JHWS was viewed as insufficient.
2. How far have HWBs strengthened collaboration, trust, goodwill and linkages between partners horizontally (across organizations including CCGs) and vertically (with agencies ‘on the ground’ such as HealthWatch and the voluntary sector)?
Although trusting and good relationships had developed to varying degrees and in various areas in all five sites, among different partners, their development was patchy. In site 3, as noted, where they had built successful partnerships in terms of integration, the HWB Chair highlighted the importance of trust: Right throughout this whole experience for me, it's all been about relationships and building trust and being open and honest with each other. And I think if there's one secret, I would say that's the secret of what we've achieved. I think Health and Wellbeing Boards need to focus on that and understand what that can achieve for them. I think historically it’s fair to say that the primary care trust did not have a good relationship with the local authority. And that the local authority did not have a good relationship with the primary care trust … there was I think blood on the floor at times.
The Vice Chair of the HWB at site 2 encapsulated a common theme in the responses, that of boards not being able to hold partners to account: The problem, as I see Health and Wellbeing Boards, is they’re not accountable. And if you’ve got no kind of controls, and you can’t hold people to account, apart from through having a good relationship and a conversation, actually, it means they’re not terribly effective. The left-hand side [of the page] is the high level outcomes, what we’re trying to achieve. Nice and clear on that. The right-hand side was, well, what are the specific measures, targets and who’s accountable for them? We weren’t so good at that. If you sort of step back and ask, where was the decision made? It wasn't at the Health and Wellbeing Board because all of the information and intelligence and critical thought that enables the decision was offered elsewhere and the decision was taken elsewhere. And what the HWB did was to say ‘Yes, we agree, carry on.’ But is that decision making? Some people would say, ‘No, that's rubber stamping.’
In regard to working with agencies at street level, such as the voluntary sector and HealthWatch, there was a concern that such agencies generally had little influence on HWBs and were somewhat of an afterthought. A member of a community organization in one of the voluntary sector focus groups was critical about decisions being made elsewhere, not by the HWB, and about how the voluntary sector was not meaningfully involved: I do think as a community engagement organization, there is a point at which we need to say, ‘Do you know what, we’re not going to collude with the circus anymore.’
With HWBs in our study sites largely having no clear vision and purpose, coupled with a lack of accountability and weak system leadership evident in two of the sites, there was very little in the way of what study participants themselves determined as tangible outcomes – namely, achieving targets and goals set by boards, largely through the priorities of the JHWSs and other means such as health and social care integration. A HWB voluntary sector representative in site 4 discussed the lack of outcomes in terms of health inequalities: I suppose the other thing is anything to do with health inequality which tends to be mentioned. So we’ve had several presentations about the difference in life expectancy between people in the far south of the city and the far north. But there’s never any plan for tackling that in any way. Well, on paper it seems to have achieved things, and it’s signed off quite a lot of strategies … But I couldn’t say confidently that therefore things are getting implemented.
Respondents’ thoughts on the future
What sort of future, if any, awaits HWBs? During the study, Sustainability and Transformation Plans (STPs) were introduced by NHS England on the back of the Five Year Forward View. 20 These are intended to help drive transformation in health and care outcomes between 2016 and 2021, with NHS providers, CCGs, local authorities and others coming together to form 44 geographical STP ‘footprints’ across England. The plans were renamed Sustainability and Transformation Partnerships and the subsequent establishment of Accountable Care Systems, and latterly Integrated Care Systems (ICSs) and/or Partnerships, in order to deliver the STPs. 20
In our study, respondents expressed concerns that HWBs and partnerships at a local authority level would become increasingly irrelevant and at risk of being subsumed, or simply bypassed, by STP boards. As a Consultant in Public Health in site 4 stated: ‘We are in grave danger of the STP process effectively side-lining even more … the Health and Wellbeing Boards … it just seems to me you might as well just get rid of them [HWBs], or make them more powerful, but at the moment it does feel like a lingering death. That’s my view.’
These concerns appear to be reinforced by the NHS Long Term Plan, which reaffirms the commitment to ICSs and accompanying partnerships, but which makes only one fleeting reference to HWBs. 21 There is certainly no mention of HWBs being system leaders located at the heart of the new place-based arrangements that are advocated.
Discussion
Our research shows that the potential benefits of HWBs have not been realized. With the partial exception of one site, site 3, the HWBs in this study largely resorted to the default setting and operated much as earlier public health partnerships had done. Previous cultural and relational factors were seen by respondents to be influential in shaping HWBs’ development and there remained tensions between the agencies and personnel on HWBs and the dynamics between partners were important in shaping, if not determining, the effectiveness of boards. In contrast, site 3 decided to invest time, energy and commitment to establishing partnerships which, in terms of the integration agenda, made a tangible difference in respect of there being a large pooled budget and the co-location of social workers. A key message from the research, therefore, is that partnerships require a deep commitment, space and time to develop, and a clear recognition of what they are trying to achieve while remaining attentive to changing circumstances.
When focusing on whether HWBs had established partnerships which strengthened collaboration and organizational linkages, including ownership of the JHWS, it was found that in the majority of study sites there was an inclusive membership with a high level of representation from the key partner organizations. However, high trust and sound relationships were not a key feature. Also, membership did not automatically translate into a HWB that made decisions and acted in a strategic manner due to partners having their own priorities and agendas; there being no clear strategic direction or agreement for what partners were responsible for in terms of elements of the JHWS; and, even where there was evidence of such a responsibility, there were no clear mechanisms in place for holding partners to account.
In the majority of study sites there was a clear lack of evidenced outcomes. Insufficient accountability, lack of strategic focus and weak or non-existent monitoring were cited as key factors. Instead, process issues were largely cited as outcomes. Yet there remains an opportunity for HWBs to be viewed as the key local partnerships as part of a larger STP place-based footprint. But for this to happen, a number of concerns need urgent attention. Most importantly, what has largely not been achieved in previous health partnerships, or with HWBs, is to communicate to those at the front line the strategic aims of the HWBs in relation to their area of work, why they are important, what goals are to be achieved (both short- and long-term), and how those engaged in the work can contribute to these in order to ensure ownership of the JHWS and its aims.
Conclusions
Partnerships in health and social care are difficult to make work at the best of times, but in the current policy landscape of fragmentation and constant policy churn, joint working has become more critical and challenging.
In addition, several of the HWBs in our study had either not learnt, chose not to, or were unable to, learn the lessons of previous partnerships. This was because they did not clearly identify what the partnership was for and what it wanted to achieve. Yet HWBs are the only body possessing a statutory legitimacy and democratic accountability that is able to connect with, and respond to, local communities. They are therefore well placed to act, in the words of one of our study respondents, as ‘the beating heart’ in coordinating efforts to improve population health in a community. They are also the one place where the system can come together. Unfortunately, in their present form, HWBs lack the power to hold partners to account and truly act as system leaders.
It is only through working from the bottom up and across partner organizations within a clear strategic framework that the opportunity can be created to prevent agencies focussing predominantly on their own priorities. This would also build in accountability with a sense of ownership and purpose across the system while, at the same time, displaying bottom-up and top-down system leadership. The role of HWB sub-groups and workshops is one way to ensure all key stakeholders are engaged at all levels. HWBs also need specific accountable implementing structures, perhaps as part of public health teams in local authorities, in partnership with ICSs, to ensure STP/HWB plans and strategies are co-ordinated in a bottom-up manner so they can have an impact on population health. 22 Above all, boards need some strategic steer and joined-up thinking from government which, having shaped a policy landscape characterized by fragmentation, duplication, choice and competition, is now seeking to create a different landscape characterized by collaboration and joined-up whole systems thinking.
HWBs could have a positive future but only if they are given statutory powers in order to pursue and drive the policy agenda through being able to hold partners to account. While ‘soft’ power and being able to influence the actions of others are still important aspects of their work, without statutory powers to hold partners formally to account for their actions HWBs will remain weak and easily disregarded. This would be regrettable when HWBs are in many respects well-placed to lead the radical upgrade in public health called for in both the NHS Five Year Forward View and Long Term Plan.19,20 In the absence of such reform, HWBs stand to wither on the vine.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by a grant from the National Institute for Health Research Policy Research Programme Project PR-X03-1113-11007. The views and opinions expressed in the article are those of the authors and do not necessarily reflect those of the NIHR PRP or the Department of Health.