
Abstract
Objective
Population health management (PHM) refers to large-scale transformation efforts by collaborative adaptive health networks that reorganize and integrate services across public health, health care, social care and wider public services in order to improve population health and quality of care while at the same time reducing cost growth. However, a theory-based framework that can guide place-based approaches towards a comprehensive understanding of how and why strategies contribute to the development of PHM is lacking, and this review aims to contribute to closing this gap by identifying the key components considered to be key to successful PHM development.
Methods
We carried out a scoping realist review to identify configurations of strategies (S), their outcomes (O), and the contextual factors (C) and mechanisms (M) that explain how and why these outcomes were achieved. We extracted theories put forward in included studies and that underpinned the formulated strategy-context-mechanism-outcome (SCMO) configurations. Iterative axial coding of the SCMOs and the theories that underpin these configurations revealed PHM themes.
Results
Forty-one studies were included. Eight components were identified: social forces, resources, finance, relations, regulations, market, leadership, and accountability. Each component consists of three or more subcomponents, providing insight into (1) the (sub)component-specific strategies that accelerate PHM development, (2) the necessary contextual factors and mechanisms for these strategies to be successful and (3) the extracted theories that underlie the (sub)component-specific SCMO configurations. These theories originate from a wide variety of scientific disciplines. We bring these (sub)components together into what we call the Collabroative Adaptive Health Network (CAHN) framework.
Conclusions
This review presents the strategies that are required for the successful development of PHM. Future research should study the applicability of the CAHN framework in practice to refine and enrich identified relationships and identify PHM guiding principles.
Keywords
Introduction
Population health management (PHM) is increasingly seen as a means to realize a sustainable and more integrated approach to health and care, contributing to the simultaneous improvement of population health and quality of care while reducing cost growth (triple aim (TA)).1,2 PHM strategies seek to address the full range of health determinants (personal, social, economic and environmental) 3 and bridge public health, health and social care and wider public services (e.g. housing, education)1,4 towards building healthier communities. Such strategies are often implemented through place-based PHM approaches. 4
PHM models and approaches range from closely integrated to more informal collaborative adaptive health networks.1,4,5 Examples include the Accountable Health Community model in the USA, which has evolved from accountable care organizations and involves the re organization of service delivery approaches through enhanced clinical-community linkages supporting local communities to address health-related social needs. 6 In England, there has been a move towards more integrated service delivery systems to meet the health and care needs of the local population, with the introduction of new care models and sustainability and transformation partnerships bringing together health and social care locally and having PHM at their core. 7 The Netherlands have introduced a programme of pioneer population management networks, which are developing new payment and service delivery models aiming to accelerate PHM, similar to the ‘Healthy Kinzigtal’ integrated care network in Germany.8,9
However, despite the attraction of PHM as an approach to improve the health of the local population, its actual use in practice remains challenging. This is, mainly, because the implementation of PHM requires a system-wide approach, and although the literature on care integration10,11 and system transformation more widely4,12 has provided some insights into the key ingredients for change, the overall process remains inadequately understood. Implementing PHM, as any complex change, will require changes in the way people and organizations function, and people’s behaviour, in turn, will be determined by the specific circumstances within which they operate.13,14 This requires an adaptive approach to create the necessary conditions to enable stakeholders to work collaboratively in (formal or informal) health networks towards developing PHM.
This study seeks to contribute to the emerging literature on PHM by providing an integrated theoretical overview underlying PHM strategies linking public health, health care, social care and wider public services to achieve the triple aim. It develops a framework highlighting the key components of PHM, each providing insight into (1) the strategies that need to be implemented to accelerate PHM development, (2) the necessary conditions (i.e. contexts and mechanisms) for these strategies to be successful and (3) the theories that underlie the relationships between strategies, contexts, mechanisms and outcomes. The framework summarizes the how and why of PHM development. The integrated overview captured in the framework can help programme managers, policy makers and researchers to design and/or improve and evaluate PHM approaches.
Methods
Study design
We performed a scoping realist review following the RAMESES reporting standards (see Online Supplement). 15 We sought to understand causality by linking strategies (S), contexts (C), mechanisms (M) and outcomes (O) (Table 1),16,17 asking ‘what is it about this strategy that works in this context and why does it lead to specific outcomes’? Informed by a literature review of PHM, 2 we used the following working definition: PHM refers to large-scale transformation efforts required for the reorganization and integration of services across public health, health care, social care and wider public services in order to improve population health and quality of care while at the same time reducing cost growth.
Realist evaluation concepts used in this study.

PHM: population health management; SCMO: strategy-context-mechanism-outcome; TA: triple aim.
Identifying studies
We searched the electronic databases Medline and Embase, Global Health, SciSearch and Scopus for English, Dutch and German language papers published between January 2010 and January 2016. This time period was chosen because a prior review of PHM2 showed that it was only from 2010 that the triple aim was increasingly associated with the process of reorganizing and integrating services across public health, health care, social care and wider public services. A comprehensive search strategy was developed to identify studies using the following search terms: health care, health care system reform, factors and mechanisms (general and specific terms) combined with social care, community care, welfare, public health, prevention and governance, accountability and supervision. The search terms governance, accountability and supervision were added because PHM implies changes in the structures and processes as responsibilities for achieving the TA are shared (see Online Supplement Appendix 1 for the detailed search strategy).20,21 Two researchers (BS and HD) independently screened identified studies (peer and non-peer reviewed) for eligibility following a set of exclusion and inclusion criteria and focussing on high-income countries (Online Supplement Appendix 2). 22 Studies were screened independently, with disagreements resolved by discussion within the research team.
Quality appraisal
Articles were quality appraised using the principles of rigour and relevance. 15 Methodological rigour was rated using the Wallace et al. quality appraisal tool, 23 while relevance was assessed by determining whether the extracted data from included studies contributed to answering the research questions.
Data extraction, application of realist principles and synthesis of PHM components
We created a bespoke data extraction form describing each identified place-based PHM approach, extracting information on the general characteristics of the approach (e.g. sectors and stakeholders included). We further analysed each included study for postulated causality between PHM strategies, contextual factors and underlying mechanisms put forward by study authors, and the outcomes of strategies (strategy-context-mechanism-outcome or SCMO configurations), as well as for theories mentioned in papers underlying assumed causal relationships or for alternative explanations of how strategies led to results. We used iterative axial coding 24 to relate SCMO configurations to the underlying theories as postulated in studies and to cluster them. This process was conducted in four cycles and identified a range of (sub)themes that we developed into (sub)components of our final conceptual framework. The (sub)components were defined based on identified theories and contained (1) the (sub)component-specific strategies, (2) the contexts and mechanisms that explained how these strategies led to (sub)component-specific outcomes and (3) the extracted theories that underlie identified SCMO configurations.
Data extraction, analysis and synthesis of the data were performed by two researchers (BS and HD) in a series of calibration exercises, independently comparing data extracted from 10 studies for level of detail, identification of relevant data and identification of SCMO configurations and underlying theories, to ensure consistency in our approach. Further data extraction, analysis and synthesis were conducted by one researcher (BS). The data were regularly shared and discussed within the research team to ensure validity and consistency in the inferences made. The Advisory Committee of the Dutch Monitor Pioneer Sites Population Management, which included scientists and representatives of the Dutch Ministry of Health, Welfare and Sports and of Dutch PHM initiatives, reflected upon the first results of this review. Based on these reflections, no adjustments were needed.
Results
The literature search yielded 3262 potentially relevant studies of which 415 were included on the basis of title and abstract only. Of these, about two-thirds were excluded as they addressed collaboration between fewer than two sectors (n = 281) or implied no change in governance (n = 42). The quality appraisal resulted in the exclusion of further 40 papers that lacked rich descriptions of contextual factors, with an additional 11 studies excluded because they did not discuss the underlying mechanisms. A total of 41 studies were finally included (see Online Supplement Appendix 3).
Study characteristics
The majority of the included studies were set in the USA and the UK (Table 2 and Online Supplement Appendix 4). Organizations involved were national, regional or local governments, research institutes, patient-client representative organizations, and voluntary organizations. Almost all studies concerned transformative changes at the regional-local level or large community initiatives. Twenty place-based approaches focussed on reorganizing and integrating services across public health, health care, social care and wider public services. Twenty place-based approaches have been in operation for more than five years.
Key characteristics of included studies.

Note: ACO: accountable care organization; AF4Q: Aligning Forces for Quality; CCG: clinical commissioning groups; CMS: Centers for Medicare & Medicaid Services; CSSS: Health and Social Services Centres; GP: General Practitioner; IT: information technology; PCT: primary care trust; POPP: Partnerships for Older People Projects; SHA: Strategic Health Authority; VISN: Veterans Integrated Service Network.
aThe list of references is provided in Online Supplement Appendix 3.
bThe duration of the research project that has monitored the initiative-approach.
cNA: no available information if the approach is still ongoing or if it ended.
Identified components and subcomponents
Iterative axial coding of the SCMO configurations and the underlying theories identified eight components considered to be key for the acceleration of PHM development: social forces, resources, finance, relations, regulations, market, leadership and accountability. Each component contains three or more subcomponents, with a total of 37 subcomponents identified (see Online Supplement Appendix 4 for further detail). We discuss each identified component in turn (Table 3). An overview of all configurations of applied PHM strategies identified in this study and the contextual factors and mechanisms that explain the outcomes of these strategies is available from the authors.
The CAHN framework’ components and examples of underlying SCMO configurations.

PHM: population health management; SCMO: strategy-context-mechanism-outcome.
Social forces are anchored at the institutional level and consist of three broad types that provide guidelines for what generally does happen (cultural-cognitive), what should happen (normative) and what must happen (regulative) (Table 3 and Online Supplement Appendix 5). Our review found that in order to change what generally happens, four successive groups of strategies need to be implemented. These include making sense of new, uncertain or ambiguous situations related to PHM development. For example, strategies such as a new vision and goals underpinning the given collaborative partnership helped stakeholders’ understanding of a new identity as they could identify with the new PHM identity in a way that did not downplay or replace their own identity.25,26 Furthermore, knowledge exchange opportunities associated with new working models changed stakeholders’ existing beliefs and working patterns by enabling ongoing discussions, which helped them getting a better understanding of how professionals from other disciplines interpreted different health concerns and how they valued and trusted particular approaches.27,28 In addition, stakeholders became aware of the potential benefits of bridging boundaries between sectors, geographies, professions or structures (e.g. incompatible information technology systems). 29
Resources refer to the demand and supply of resources and technologies that enable place-based approaches to create continuous improvements for the services delivered. SCMOs showed that successful PHM strategies that aimed to implement a learning environment did so through establishing contexts that reinforced continuous improvement.30,31 Examples include hands-on training in multidisciplinary settings in the use of integrated health information system.29,32 These contexts in turn motivated professionals across stakeholder organizations to achieve better integrated performance.
Finance refers to the management of financial arrangements and contains three elements: financial strategies, contractual relationships and contractual scope and requirements. Our review found that social relationships between contracting parties (as reflected in socio-legal theories 33 ) played an important role in establishing new financial arrangements such as value-based payment models.34,35 The transition to a new relationship style was reported to be challenging in cases were stakeholders had had relatively long histories of ‘arm’s-length’ negotiations between contracting parties primarily about the financial terms of their contract. For example, moves to value-based or performance-based payment models in the USA and the Netherlands required openness between contracting parties to jointly identify shared interests, aims and performance targets.34,36 In England, commissioning (strategic purchasing and contracting of health services) was also described as being dependent on prior relational work with flexibility and reciprocity between commissioners and providers as crucial contextual factors for redesigning and reducing costs of transactional services.35,37
Relations refer to how cultural change is enacted at an interpersonal level. In addition to the seven constructs defined by Lanham 38 (trust, mindfulness, heedfulness, respectful interaction, diversity in perspectives, social and task-relatedness and communication channels), we identified an additional construct ‘the history of personal relationships’.34,39 SCMOs showed, for instance, that in case of cross-sector collaboration, lack of a personal history between professionals with different expertise from different organizations negatively influenced organizational change and learning. SCMOs also showed that conditions that strengthen social interaction between these professionals, e.g. by locating them in the same building or room, offered openness to others’ ideas, provided new meaning to differences in perspectives or facilitated trust in others’ ability.40,41
Regulations refer to health policies and related laws and regulations, problems that need political attention, political influence and the political agenda. SCMOs revealed, for instance, that leaders tried to influence the regional political agenda by connecting regional and provincial-state-national problems and by engaging with strong allies (payers, politicians and knowledge institutions).40,42,43 Integrating regional (state, province) and national health problems into a new regional vision and its alignment with stakeholder support across institutional networks (e.g. to verify the policy content), political levels and regional or national payers strengthened the receptiveness of governmental bodies for policy change. These contextual factors created a sense of urgency and a broad awareness of and credibility for the health problems and the policy content, which contributed to securing political power and support and financial resources.
Market refers to the establishment and continuation of partnerships between stakeholder organizations and the structure and dynamics of the regional setting in which organizations operate. Our review found that in addition to factors that influence collaborative working between organizations in a geographical area44 (e.g. trust, agreement on purpose and needs; see Online Supplement Appendix 4), historical relationships between stakeholders and their respective leaders also influenced the establishment and continuation of collaborative initiatives.25,31 For instance, initiatives’ leaders who aimed to align stakeholders’ interests to further develop the place-based initiative used their knowledge of past regional working relationships and developments to put these into a future regional perspective, as such they presented themselves as neutral and credible forums within the regional setting where organizations’ interest would be protected. This appeared to foster respect and positive attitudes in the region, which in turn helped to attract new stakeholders, even among organizations whose activities partly overlapped with that of the place-based approaches.
Leadership refers to leadership structures, processes and styles that provide support and direction for the development of PHM across organizations and sectors. The review pointed, for instance, to the importance of distributed leadership whereby leadership is conceived as a collective process involving multiple participants within the place-based initiative. SCMOs showed that PHM strategies, which sought to enable the building of common ground across stakeholders, created distributed leadership roles across stakeholder organizations with legitimacy, decision-making and resources available within these roles.43,45 This was seen to enable leaders to gain credibility for their roles, allowing them to exert influence to bring about change across the different stakeholder organizations in the initiative.
Accountability refers to who (which parties) can be held accountable or hold others accountable, the domains and processes of accountability including formal and informal procedures, for instance, for adherence to PHM goals and specific performance thresholds. The management of competing accountabilities was seen to be particularly challenging because of the many stakeholders involved who operated in different sectors and different contexts and had different perspectives on what accountability meant. PHM strategies that implemented governance structures, which represented key leaders of stakeholder organizations and who were recognized for their expertise, commitment and credibility, were seen to help manage competing interests, reduce confusion about the initiative’s purpose among participating organizations and resulted in stakeholders meeting their responsibilities.31,45
The CAHN framework
We brought together the eight components in the form of what we termed the CAHN framework (Figure 1). The name of the framework seeks to reflect that place-based approaches are regional networks in which stakeholders from different sectors that operate in different contexts establish a (formal or informal) collaborative health network with the purpose of developing PHM. This requires an adaptive approach in terms of PHM strategies’ resources or incentives to bring about the necessary changes for stakeholders to work collaboratively for developing PHM. The eight components are interdependent, with the outcome of one component strategy forming the (pre-)context for another component in the chain of implementation steps. For instance, our review found that strategies to develop a learning environment (resources) resulted in data sharing, performance metrics and patient attribution between contracting parties. This created a new context, which formed the basis for negotiations on the financial terms of contracts (finance).
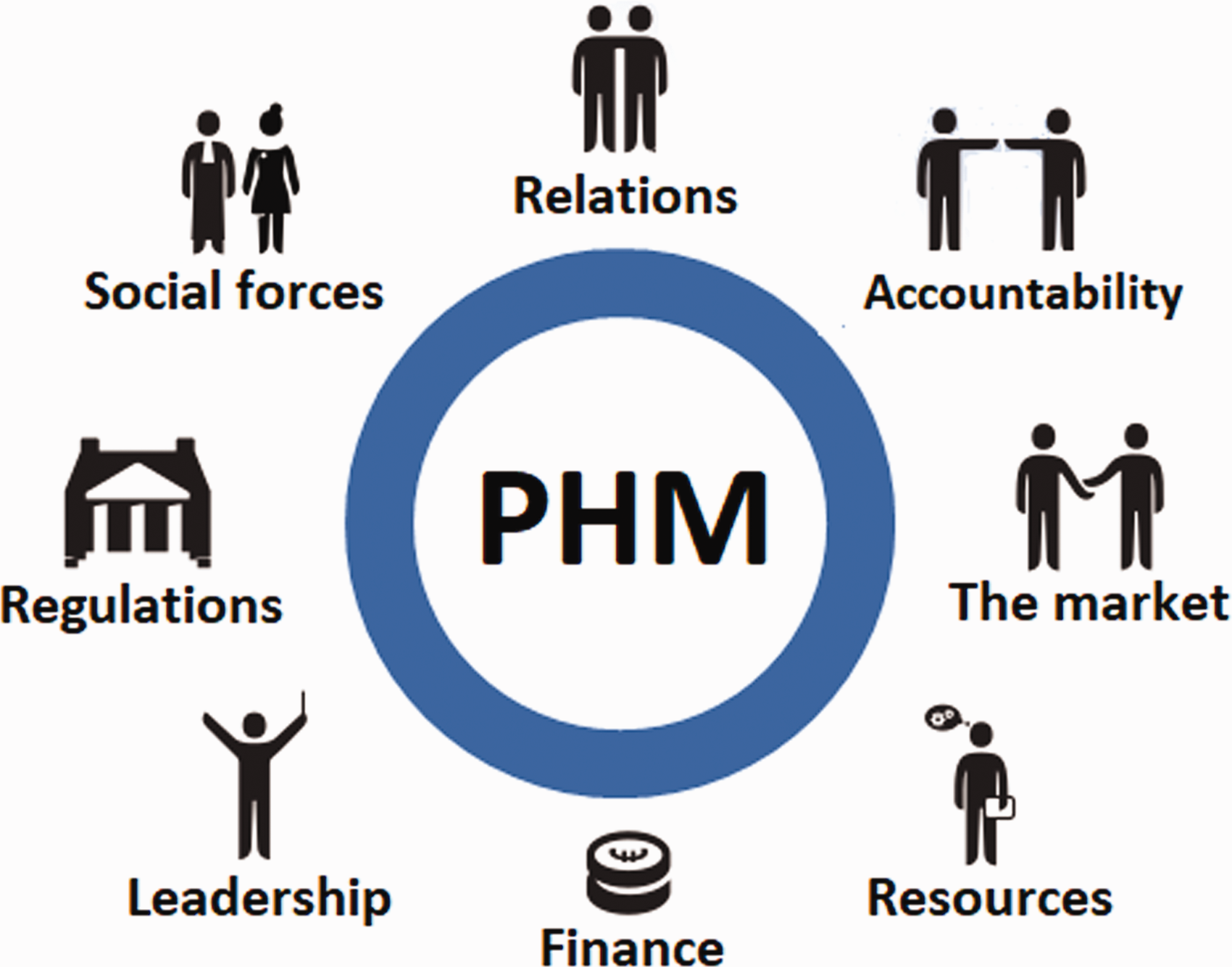
Collaborative adaptive health network (CAHN) components for successful PHM development. PHM: population health management.
Discussion
This review presents a theory-based framework drawn from the available evidence on PHM strategies that reorganize and integrate public health, health care, social care and wider public services to achieve the triple aim. It identified eight components considered to be key for the acceleration of PHM development: social forces, resources, finance, relations, regulations, market, leadership and accountability, with a total of 37 subcomponents. The review captured a wide range of theories including sociology, political science, cultural science, organizational science, economics and system dynamics. As such, the (sub)components that make up the CAHN framework summarize the insights into how and why PHM can be successfully accelerated. We believe this to be the first study presenting an overview of the components identified to be key for PHM development using a realist methodology. It goes beyond conceptualizations of integrated care, as for example summarized in the Development Model for Integrated Care 11 by capturing the continuum of public health, health care, social care and wider public services and theories underlying the reorganization and integration of services across the continuum. It provides insight into strategies and the relevant contextual factors and mechanisms to better understand why specific strategies reached specific outcomes in specific circumstances.14,46
The strengths of this study rest on the realist methodology, 18 describing the causal relationships between strategies, contexts, mechanisms and outcomes of PHM development and their underlying theories. The framework suggests routes for designing and implementing PHM strategies and creating the structures and processes needed to effect change in the contexts in which initiatives operate in such a way that most likely stimulate progress on PHM.
This review has a number of limitations. First, most included studies are set in the USA and the UK, which limits the generalisability of our findings to other settings and national contexts. At the same time, some features around organizational values and cultural norms that we identified are likely to be applicable to a wider range of health systems. Second, identifying what caused something to happen in open systems such as place-based approaches is complex. The conditions, that is, the changed context and the mechanisms that make the outcomes possible, are also often poorly described, affecting the quality of the evidence on identified SCMOs. Third, we argue that the eight identified components are interdependent, but the extent of this interdependency remains unclear as does the relative importance of individual components in different settings.
To gain further insight into the conceptualization and operationalization of PHM, more research is needed. Using the CAHN framework, future research could investigate the further development of PHM in the countries captured in this review; there is also a need to study other systems and settings to enable refining and enriching the components and testing the validity of the framework. In addition, future research should investigate how the different components of the CAHN framework relate to each other and their relative importance in different systems and settings. There is also a need for the further refinement of specific components, in particular leadership and accountability, which were not underpinned by theories or models as these were not provided by the included studies. Finally, there is need to investigate the PHM guiding principles for future initiatives.
Conclusions
This review identified eight components considered to be key for the acceleration of PHM development and which form what we described as the CAHN framework. We provide an integrated overview of the strategies that are required for the successful development of PHM, the necessary contextual factors and mechanisms to achieve specific outcomes and the theories that were extracted from the included studies and that deepened the understanding of these relationships. Future research should study the applicability of the framework in practice to refine and enrich identified relationships and identify PHM guiding principles.
Supplemental Material
HSR907359 Supplemental Material - Supplemental material for Reorganizing and integrating public health, health care, social care and wider public services: a theory-based framework for collaborative adaptive health networks to achieve the triple aim
Supplemental material, HSR907359 Supplemental Material for Reorganizing and integrating public health, health care, social care and wider public services: a theory-based framework for collaborative adaptive health networks to achieve the triple aim by Betty Steenkamer, Hanneke Drewes, Kim Putters, Hans van Oers and Caroline Baan in Journal of Health Services Research & Policy
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute for Public Health and the Environment (RIVM).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.