
Abstract
Objective
The United States’ Institute of Medicine recommends that health care providers be aware of sex trafficking (ST) indicators and conduct risk assessments to identify people at risk. However, the challenges among those who conduct such assessments remain largely understudied. The aim of this study was to understand the perceived barriers to ST risk assessment among health care providers in a large health care organization.
Methods
This study used a collective case study approach in five sites of a large health care organization that serves high-risk populations in a Midwestern state. Twenty-three in-depth, semi-structured interviews were conducted with health care staff (e.g. medical assistants, nurse practitioners). Two research team members conducted independent deductive coding (e.g. knowledge of ST), and inductive coding to analyse emerging themes (e.g. responses to ST risk or commercial sex disclosures, provider role ambiguity).
Results
Although staff routinely screened by asking ‘Have you ever traded sex for money or drugs?’, participants primarily described avoiding further discussions of ST with adult patients because they (1) aimed to be non-judgmental, (2) viewed following up as someone else’s job, and/or (3) lacked confidence to address ST concerns themselves, particularly when differentiating sex work from ST. Differences all emerged based on clinical context (e.g. urban location).
Conclusions
There may be missed opportunities to assess patients for ST risk and use harm-reduction strategies or safety plan to address patients’ needs. Implications for practice, policy, and future research are discussed.
Introduction
Sex trafficking (ST) occurs when a commercial sex act is induced through force, fraud, or coercion, or when the person induced to perform such an act is under 18 years of age. Commercial sex acts include prostitution, pornography, exotic dancing, and the exchange of sex for basic needs.1,2 As such, adults who engage in commercial sex acts may be sex trafficked but commercial sex involvement does not equate to ST. Sex workers, for example, include adults who engage in commercial sex by choice, which can be constrained (i.e. would choose alternative means to make money under different circumstances) or autonomous (i.e. choosing voluntarily under any circumstance to sell sex).3,4 Assessing risks among people involved in commercial sex work is important, as negative health consequences of ST include reproductive, sexual, neurological, gastrointestinal, and mental health problems.5,6 Sexual health care providers, particularly in clinics that serve low-income and/or high-risk people, may encounter people at risk of ST who access care for health problems such as (sexual and other) infections, pregnancy testing, and contraceptive/reproductive care. 6
Consequently, the Institute of Medicine in the United States recommends that health care providers should be aware of ST indicators (i.e. red flags), ask initial ST risk screening questions, and conduct further risk assessments as necessary. 7 ST indicators in health care settings can be reproductive (e.g. multiple STIs, pregnancy/abortions, sexual partners, etc.), physical (e.g. history of injury, abuse) or behavioural (e.g. substance use, appearing fearful, accompanied by a controlling partner).8,9 Health care providers should be ‘comfortable incorporating specific questions into their conversations with patients … at risk for trafficking’.10(p446)
Some examples of recommended ST risk screening questions include: 1) Have you ever traded sex for something you wanted or needed (money, food, shelter)? 2) Has anyone ever taken sexual photos of you to put on the internet?
Upon disclosure of a commercial sex act, providers should respect the patient’s wishes to discuss further, particularly if the patient denies victimization or declines assistance. 11 If the patient is willing to discuss further, providers can play an essential role in assessing ST risk. Safety planning using harm-reduction strategies, as well as referrals to behavioural health and/or social services (typically for adults), can be offered.11–13 Providers must additionally follow mandated reporting protocols for minor-aged patients. 14 Key components of sex trade harm-reduction can include education (e.g. accessible outreach materials), empowerment (e.g. fostering autonomy, negotiating skills), prevention (e.g. provision of barrier methods, lubricants, routine STI testing), and care (e.g. accessible physical and mental health care).3,13,15 Sexual and reproductive health care providers have a unique opportunity to engage in harm conversations with patients to mitigate risks and refer to services as needed.
Despite increased funding, resources, and campaigns dedicated to increasing identification of people at risk of ST, the extent of health care providers’ perceptions of assessing for ST remains understudied.5,6 Understanding how providers respond to people at risk of ST who they encounter in clinical practice can inform training and organizational policies to identify this critically underserved population. As such, this paper explores health care providers' perceived strengths and challenges to conducting ST risk assessments in a large, health care organization in the US.
Methods
This study used a collective (multi-site) case study approach 16 to guide semi-structured, in-depth interviews with healthcare providers who had direct contact with patients. This approach involves a common set of research questions at sites that are linked through a common issue, structure, or other similarities. 17 The authors partnered with one large, health care organization that provides sexual health care to people with and without insurance across a Midwestern state. Each of the five sites were selected to explore different contexts, such as region and demographics served, in September 2019–February 2020.
Data collection
Participant recruitment
Recruitment flyers and emails were sent to all health care providers, including medical assistants (MAs) who conduct verbal assessments and vitals, clinicians who conduct physical examinations (i.e. nurse practitioners, nurses, physicians), and managers (who had dual direct practice and administrative roles). The first author also attended staff meetings at larger sites to introduce the study and answer questions. Potential participants were asked to email the first author, who determined if they met inclusion criteria (i.e. worked at the organization and had direct contact with patients) before conducting the interview. The researchers sought to engage interviewees working in a variety of roles (e.g. clinicians, managers, and MAs) and in a variety of contextual dynamics of sites (e.g. urban and rural).
Interviews
A total of 23 interviews were conducted and occurred in private offices in-person or by phone (as per participant’s preference). Interviews lasted approximately an hour but ranged from 35 to 90 minutes. The interview guide explored (1) knowledge and awareness of ST, (2) roles and challenges in conducting ST risk assessments, and (3) providers’ perceived relevance of ST indicators when assessing for ST. After the interview, participants were asked to complete a demographic questionnaire and were compensated. Revisions were made to the interview guide after the 10th interview, in response to the iterative data collection and analysis process described below. Data were collected until informational redundancy was reached.18,19
Data analysis
All interviews were transcribed by a research assistant or professional company, checked for accuracy, de-identified, and imported into Dedoose (Qualitative Analytic Software). As is consistent with a multi-site case study, the research team analysed data related to individual sites first before making comparisons across sites, 16 which provided holistic integrity to the umbrella organization while viewing the different sites as related to one another. 18 The individual members of the team independently conducted deductive coding based on the concepts and categories embedded in the interview guide (e.g. knowledge of ST, practice experiences) as well as open coding to uncover emergent concepts and categories. Emerging themes, such as varied responses to commercial sex disclosures and provider role ambiguity, were used for focused coding. Discrepancies were discussed within the research team and found to be minimal, relating primarily to differences in wording of labels (e.g. ‘provider ambiguity’ vs. ‘provider uncertainty’). Results reported here focus only on adult patient interactions, as participants described only one minor-aged patient who disclosed sex trading.
The sample’s characteristics are summarized in Table 1. The sample was predominantly White, non-Hispanic female MAs and nurse practitioners (NPs). Approximately two-thirds were from urban locations. Participants held a wide range of years in their current roles as well as years of total work experiences. All reported names are pseudonyms.
Sample information (n = 23). Within locations, interviewees are sorted alphabetically by pseudonym.

aWhite indicates White and non-Hispanic, unless otherwise specified.
bUrban = population >75,000. Small urban = population
NP: nurse practitioner; MA: medical assistant.
Ethics
This study received human subjects approval from the University of Wisconsin-Madison.
Results
Although all MAs ask a ST risk screening question per the organization’s protocol (‘Have you ever traded sex for money or drugs?’), their subsequent responses ranged from minimal acknowledgement of sex trading to using harm-reduction strategies to assess and engage patients. MAs informed NPs of patients’ red flags and commercial sex disclosures (i.e. via electronic charts, face-to-face conversations, or sticky notes). Clinical staff expressed a strong desire to appear non-judgmental, which often prevented further follow-up ST risk assessments. Their roles in assessing ST varied primarily by perceived knowledge and confidence, as well as by clinic size and urbanicity.
ST risk assessments
MAs and NPs reported that patients most often denied trading sex for drugs or money. Staff described feeling conflicted between following up with observed red flags (e.g. patient accompanied by a much older boyfriend, patient making limited eye contact or providing inconsistent answers, repeat STIs) and their desire to be perceived by their patients as non-judgmental. MAs like Hannah would typically move on to the next question, particularly if they perceived that the patient did not want to discuss the topic or thought it was irrelevant: I always have a hard time when I have a feeling about something may be happening. Like, that's the last question we ask in our sexual history questions. And so, like, if I get a ‘No’, I leave it at that, personally. Just because I'm, like, I don't want to force somebody to tell me something or, you know, wrongly assume that somebody is involved in something and, like, put that label on them ‘cause we try to be as non-judgmental with our care as possible. If they've started laughing towards the middle of that, then I'm kinda, like, ‘I know they seem silly, but we just need to double check that everyone's safe.’ … Because you can tell the difference between … I feel comfortable telling the difference between nervous laughter and ‘No, this didn't even occur to me’ kind of laughter. And the reason that we ask is just to make sure that we're doing appropriate testing for you. So we don't want to be overly nosy or seem like we're being judgmental in any way, but I just want to make sure that we're not missing any additional tests that you may need. So a lot of [patients] seem like if you're just doing it because, you're not just asking because you're a nosy parker [overly inquisitive person], but you're asking because you want to make sure that you're getting comprehensive care. When I have the red flag feeling, usually I just move forward with ‘Okay, this this would be your risk, based on what you're telling me. Is there anything else that you want to tell me?’ And I leave it up to them to disclose or not. I don't want to do more harm to them, by digging too far. I ask [the MA], like, ‘When was it [the incident]? Who was it? How did she seem in the room? Do feel like she wants to talk about it more?’ Like, and I feel, like, for the majority of our patients, what they bring up was a while ago and it was maybe one-time, one partner who made them, pressured them to do something uncomfortable or … And they, they tell us because they want to be honest and they're, like, ‘I'm okay. It was one-time thing. I don't need to have a therapy session about it.
Differentiating between sex work and sex trafficking
Both MAs and NPs described challenges differentiating between sex work and ST. These challenges, when combined with the desire to be non-judgmental, often resulted in avoiding further questions when patients disclosed having traded or sold sex. Jane, like other MAs, lacked confidence to non-judgmentally assess for ST and safety plan without advocating for patients to stop engaging in sex work: I would wish that resources were provided for me, for better understanding about differences between sex workers and then how that overlaps – or maybe presents similarly to – human trafficking … I don't know how we can, I guess, best help to distinguish ‘These people are doing this for their own … This is their career and this is what they're wanting to do’ and ‘someone's forcing them to do this.’ How we're able to navigate that and figure out the correct resources for each of them. Because it's someone's job, everyone has to make money. Everyone has to find their own way. Everyone has their own skills that they use. That's all good. But it's the ones forcing them, like, I don't know how to pick that up. I said, ‘Well, I think it's great that you're coming in doing testing.’ I said, ‘Sincerely, I don't care if I see you two times or 202 times. The CDC [Centers for Disease Control and Prevention] recommendations are to do the screening for each new partner, so just know that our doors are always open to do that.’ And we always offer barrier methods. So condoms, dental dams, all that, just for self-protection as far as that goes. I said, ‘If this is no longer something that you want to do, or if you feel like it's something that you want to get out of, let me know and I can try and find some resources to help with that.’ If I have an adult woman, who says that she might be a ‘dancer,’ I will often just kind of go through those IPV [Intimate Partner Violence] questions again, even though they might have been done by the MA before I came into the room. But I’m also respecting her choices to do what she wants to do for her career … I don't feel like I have the training, at this point, to make the assumption that she's being sex trafficked, you know? I feel very comfortable asking about safety and the violence but then if I were to suggest ST, that would … Because I don't have a great tool and have any training to really know how to really ask those questions. Yeah, that makes me feel like maybe I failed this person. This is the most important thing and it takes practice. But, without a hint of judgment in your voice, you very neutrally say, ‘Hey, well can you tell me a little bit more about that?’ Or, ‘Is it okay if we talk a little bit more about that?’ And then usually the person either says ‘Yay’ or ‘Nay’. If they say ‘Yes’ be, like, ‘Okay, so take me through this. Is this people that you know? Are these friends that you know?’ You try to get more information about how that's happening. And so [one patient disclosed] that, yes, that she's dope dating [exchanging sex for drugs]. It wasn't exactly … It wasn't ST, it was just dope dating with folks who are dealers or have access to whatever that she wanted to access. Because they're testing the waters and they're testing our judgment. As long as you're neutral, then talking about harm reduction, about, ‘Okay, so are you using condoms?’ ‘No, because you can't get them to use condoms.’ ‘Okay, let's talk about the female condom because that's something you can insert.’ And you can have control over and give you some protection. Talking about that as an option. If they're interested, giving them that information. Talking about continuums of risk as far as sexual activities to help them to sort of understand that it's obviously … It's significantly riskier to engage in anal sex unprotected. So then we talk about using lubricant to reduce the chances of having there be tears, things like that … So just really having a very specific harm-reduction conversation. It's important not just for, obviously, reducing the risk of infection. It starts to begin to build this locus of control that is tiny when you're either sex trafficked or domestic violence or engaging in dope dating, where you just don't feel like you have much control over anything at all. And it starts to build a little bit of that locus of control. And in very small ways that the patient can start to take those steps. I think that there's this tendency for us to want to swoop in and be like, ‘This patient … rescue them and have them immediately stop whatever behaviour they're engaging in.’ But that is not how it works. It has to be their choice. We need to give them options … We have a lot of people who come back to us because they know they can talk to us about it, you know. And, if at the end of that conversation, they're still gonna decide to engage in dope dating that's their choice to make. But at least you gave them some options. Follow this quote with this text on a new line before the next section: “Tess emphasized how she perceived centring patient choice and autonomy as key to ensuring patients will continue seeking care.”
Urbanicity
In cases when patients in small urban clinics disclosed sex trading, MAs reported routinely choosing to document the patient’s response and then verbally informing the NP, on the assumption the NP would follow up. MAs, like Isabelle, who work in small urban clinics, indicated that following up with a patient’s disclosure was outside the scope of their role, in part because of their perceived sense of (lack of) expertise. Isabelle described her reluctance to further assess a patient’s self-reported experiences with ST: One [question] was, ‘Are you afraid to ask your partner to use a condom?’ and she said ‘Yes.’ And then we finally say, like, ‘Okay, why do you feel like you're afraid?’ And then she would stop and say, ‘Well, I'm being forced to have sex,’ is what she said. So then I don't want to go into too much detail because I don't, I don't have experience with that as an MA. But then … say it to the nurse practitioner and then she'll talk to you. I don't believe that I would say anything. I would let the nurse practitioner know … The nurse would get more in depth with that. I'm just interviewing … Because there have been employees, not at this centre, but at other centres that I've heard went into depth and they weren't supposed to. You know, they would like, ‘No, no, no, that's not your job. That's not your, that's beyond your realm of what you are supposed to be doing.’ You just have to tell them that if they ever need to talk or if they ever want resources, they could have them. I offered the same programme for the nurse examiners and I offer the Rape Crisis Center information or [name of IPV organization]. I said something like, ‘We usually give this [out] for people anyway, so if you know someone who might need this would you mind passing it along?’ She was like, ‘Oh yeah, sure. I'll pass it along if I know someone. I would say, probably, the time constraints, because even if we had additional resources and training … because we've had training on other things. One was about birth control counselling, and it was this really wonderful training about, ‘Here's all the things that you should do to help someone choose the best birth control method for them.’ And that was when my manager said, ‘You're taking too long with patients.’ I basically just stopped doing everything that they taught us in the training, so that I could get in and out … We have time limits on how much time we're supposed to spend with a patient, but if someone spends longer than that with someone or a really long time, if we come out and say, ‘They had positive IPV,’ or, ‘They're at risk,’ that's definitely an excuse or will be … It's okay if you spend longer with a patient because of that. That's one rule. I don't know. It can be really difficult. I don't know how everyone does it, because like I said, I'm always just concerned, do they feel safe? It's like any business. Even if it's not for profit, you're looking at numbers and how many clients you serve and how quickly you do that, because the trend in life is that all the critiques matter and what they say on surveys. So, if somebody wants someone back then we need to start working to get people back quicker and invite them back at every possible time. How quickly are you getting people in and out the door? You're being rated on that. Yet when it comes to training, it's about talking. You're supposed to ask open-ended questions, like, ‘How does that make you feel?’ or ‘What do you think?’ ‘What does that mean to you?’ So it’s always that dichotomy.
However, MAs regardless of urbanicity also noted their own perceived lack of skills in assessing for ST. This was best noted by Gabby who said, ‘I don't necessarily think it's just the time constraint. I don't know that staff would really have the knowledge of how to screen for ST risk.’
Discussion
This study’s findings provide insight into how health care providers assess for ST and the resulting challenges that emerge in clinical practice. There may be some missed opportunities to assess patients for ST risk, and to use harm-reduction strategies or safety plan to address patients’ needs. Providers’ well-intentioned concern for appearing non-judgmental, role confusion, and lack of clarity between sex work and ST all contributed to minimal follow-up with patients at risk. Consequently, there are important implications for policy, training, and clinical practice resulting from this study.
Providers who work with high-risk patient populations will inevitably need more time to build rapport, gather information, and assess for multiple sexual health related issues, including ST. It is essential for health care providers, particularly in busier clinics, to have flexible policies regarding time spent with high-risk patients. Such time is needed to build rapport and assess ST risks, particularly given the stigma of sex trading. 20 Although increasingly more medical providers receive ST training,10,21,22 it is likely that training that further differentiate between sex work and ST would be helpful to health care providers. Training should address a continuum of choice, agency, and victimization 4 as well as how to use harm-reduction strategies to engage patients at risk. 3 In addition, this study found that MAs or clinicians may experience some role confusion in assessing for ST and following up with red flags. Clarifying staff roles for any follow up ST risk assessments in cases of commercial sex disclosure or appearance of red flags, particularly in large organizations, may help to avoid missed opportunities to assess for ST.
Medical providers who conduct ST risk assessments should take a few steps to address the complex dynamics of sex trading and ST before assessing and safety planning. A useful approach is detailed in Table 2. Providers should begin by normalizing the spectrum of agency to victimization in sex trading before asking a question, as patients may have a range of sex trading experiences (by choice, circumstance and/or coercion). 23 Normalizing may help providers to posit a non-judgmental attitude to patients rather than suggesting that providers are not intending to be nosy. Potential ST risk screening questions include, ‘Have you ever exchanged sex for food, money, shelter drugs, hormones or anything else?’, ‘Has anyone asked you to have sex with people to make money?’, as well as general violence questions that might serve as helpful starting points, e.g. ‘Has anyone ever threatened you or your loved ones?’Adapted from 21(p584)
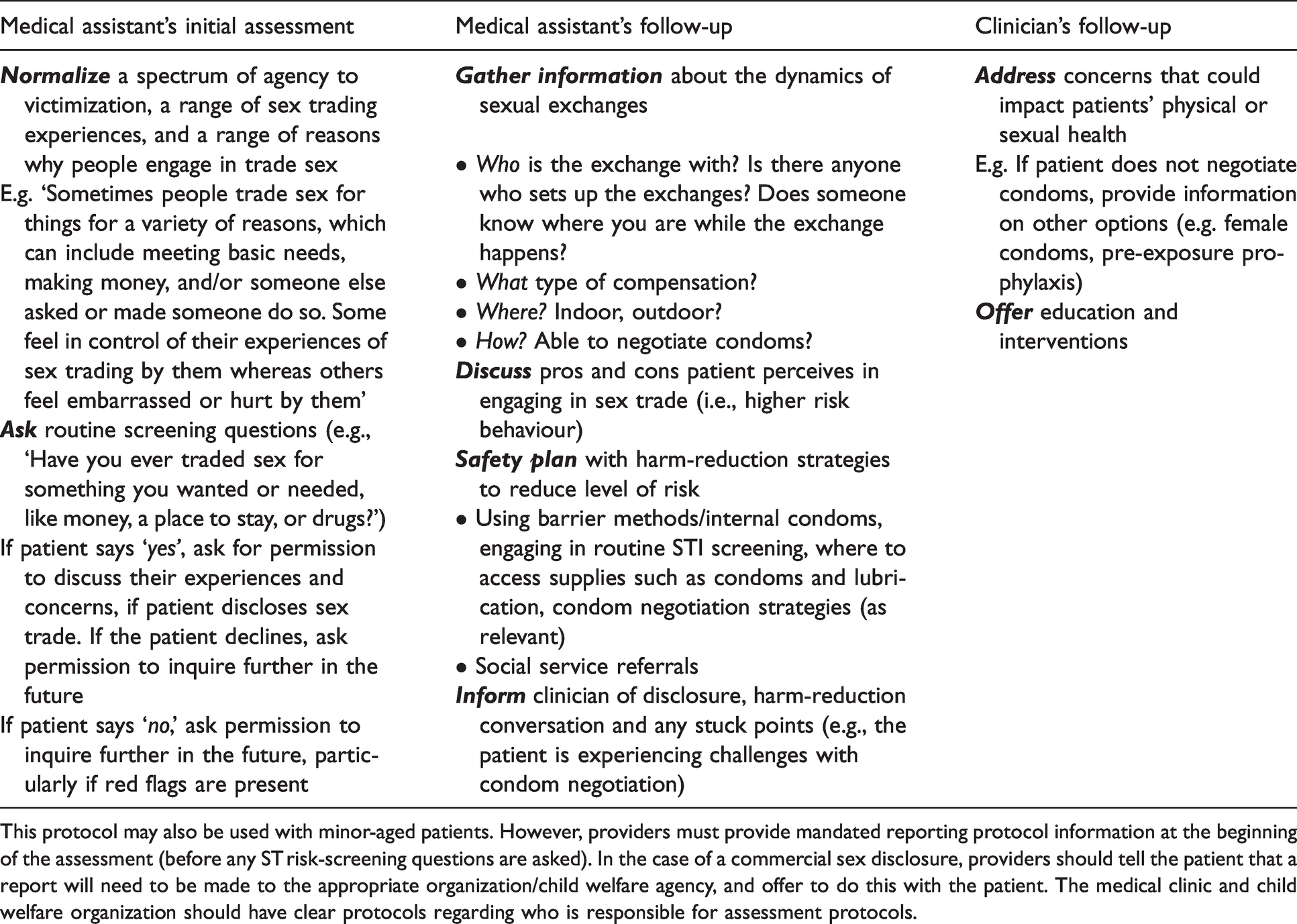
This protocol may also be used with minor-aged patients. However, providers must provide mandated reporting protocol information at the beginning of the assessment (before any ST risk-screening questions are asked). In the case of a commercial sex disclosure, providers should tell the patient that a report will need to be made to the appropriate organization/child welfare agency, and offer to do this with the patient. The medical clinic and child welfare organization should have clear protocols regarding who is responsible for assessment protocols.
If a patient discloses sex trading, providers should then ask for permission to discuss their experiences and concerns further. If the patient declines, the provider can ask the patient for permission to inquire further in the future (and document accordingly). Asking permission to discuss sex trading is consistent with several evidence-based techniques, such as motivational interviewing, which can help build rapport while reducing risk of harm. 24 Providers should also verbally acknowledge the patients’ perceived benefits of higher risk behaviour (e.g. place to stay) along with any concerns or challenges patients may be face (e.g. higher risk of STIs). As demonstrated by Tess, potential questions include: ‘Who is the sex exchange with?’ ‘Is there anyone who sets up the exchanges?’ ‘Does someone know where you are while the exchange happens?’ ‘Where does it take place?’ ‘Are you able to negotiate condom or other contraceptive use?’
Such questions can be followed up with concrete strategies to help minimize risks. This can include using barrier methods, engaging in routine STI screening, advising the patient where they can access supplies such as condoms and lubrication, and advising the patient how they can negotiate condom use with their sexual partners (and what to do if partners refuse to use condoms).
Finally, our findings suggest that providers ranged in comfort level when discussing sex and sexuality broadly, which is a critical and necessary skill for health care providers (regardless of position type) in sexual health and related medical fields. Any training that includes ST risk-assessment protocols should also be part of extensive, comprehensive training and skills practice sessions (i.e. role plays) to enhance providers’ conversations of sex and sexuality with patients. 10
Limitations
First, this analysis only focused on providers’ experiences with adult patients. Assessing minor-aged patients is an important area of future research, as mandated reporting procedures may alter patient interactions and harm-reduction strategies may differ. 25
Second, it is possible this study’s participants were not comfortable disclosing situations with particularly difficult or negative experiences or situations where they skipped ST risk-screening questions altogether. However, efforts were made to prompt for clinical practice examples in order to enhance the descriptions and normalize the challenges of conducting patient assessments.
Third, although the researchers attempted to diversify the sample in terms of clinician type, race, and gender identities, the sample was predominantly White, cisgender MAs and NPs, and not physicians. It is possible that increased diversity in the sample would have led to additional variation in experiences. Furthermore, this study examined perceptions of health care staff only. Future research should explore perceptions of patients at risk of ST and/or analyse provider interviews with mock or actual patients to address the limitations of this study and expand this work to a different state’s context, particularly outside of the Midwest.
Conclusions
Our study illuminates the challenges of ST risk assessments in clinical practice. Future research should estimate the extent to which providers ask ST risk questions and safety plan accordingly. This study’s findings should inform policies for patient-provider ST risk assessments and training to enable health care providers to practice assessing and safety planning (including using harm-reduction strategies) with ambiguous case examples. Doing so may enhance identification of an under-served population - ST survivors.
Footnotes
Acknowledgements
The authors are deeply grateful to the participants of this study for the work they do every day and for taking their time to share their challenges and successes with us. We also thank out community partners, who wish to remain anonymous at this time, for their deep commitment to this study and for assistance with its logistics.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This work was approved by University of Wisconsin-Madison Institutional Review Board, 2018–0756-CP003.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Wisconsin Alumni Research Foundation and the Women & Wellbeing in Wisconsin and the World’s Innovation Award. The project described was also supported by the Clinical and Translational Science Award (CTSA) program, through the National Institutes of Health’s (NIH) National Center for Advancing Translational Sciences (NCATS), Grant UL1TR002373. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.