
Abstract
Objective
To analyse the contribution of participatory action research (PAR) in designing and implementing joint training sessions as a means to improve clinical coordination in a public health care network in Bogotá, Colombia.
Methods
A qualitative, descriptive-interpretative study using semi-structured individual interviews and focus groups with 40 professionals (GPs, specialists, members of the local steering committee (LSC) and network middle managers) involved in designing and implementing joint training sessions to improve cross-level clinical coordination. The intervention consisted of two forms of joint training sessions for GPs and specialists, implemented through two PAR cycles.
Results
The PAR approach in designing and implementing joint training sessions led to greater awareness of clinical coordination problems and helped adapting sessions to the local health care context. Study participants highlighted the role of LSC leadership during the PAR process and the importance of ensuring the necessary resources for adopting the intervention. Limited institutional support and differences between joint training sessions affected doctors’ participation and reduced the time available to conduct the sessions. The use of a reflexive method was essential in enhancing doctors’ participation, along with session duration, the facilitator’s role and session content.
Conclusions
The study provides evidence regarding the contribution of a PAR process to designing and implementing joint training sessions for improving clinical coordination. The findings can inform similar approaches in other health systems.
Introduction
Clinical coordination between health care levels is essential for ensuring quality care and efficient resource use, 1 but it is not widely achieved in fragmented Latin American health care systems, including that of Colombia.2–4 This study followed Longest and Young’s definition of clinical coordination as ‘the harmonious connection of the services needed to provide health care for a patient throughout the care continuum to achieve a common objective without conflicts’. 5 Cross-level clinical coordination mechanisms (CCM) 6 include programming-based CCM, such as standardising skills (e.g. training), processes (e.g. shared clinical practice guidelines and CPG) or outcomes (e.g. health care maps), and feedback-based CCM, such as vertical information systems (e.g. shared electronic medical records (EMR), liaison services (e.g. case manager) or direct communication tools (e.g. phone and email). 7 Some CCM use both, standardisation and feedback, such as joint training sessions, which combine professional training and direct communication.
Much of the evidence on implementing CCM comes from high-income countries.8–10 Most studies of feedback mechanisms focus on the quality of shared information and its impact on clinical coordination,9,10 while studies of programming mechanisms commonly look at shared clinical practice guidelines, training programmes or joint consultations, with a focus on changes in clinical practice and health professionals’ knowledge and skills. 8 There is less evidence on the implementation of joint training sessions (JTS); relevant work has tended to focus on mental health, cancer and diabetes conducted in the United States, Europe and Australia. Evidence suggests that JTS can improve general practitioners’ (GP) knowledge and diagnostic skills,11,12 referral appropriateness13,14 and patient care outcomes 15 and can contribute to better cross-level coordination by means of improved communication between providers for patient follow-up and clinical management and through strengthening mutual trust and collaborative working.16,17
Strategies for enhancing care coordination, such as JTS, are often introduced in a top-down manner without involving frontline staff in strategy development. 17 Contextual factors are also often ignored, hindering their implementation in practice, for example, because of lack of time or interest of doctors, mistrust between health care levels, precarious working conditions and economic disincentives.3,6,18 Failure to adapt to the local context has been associated with reduced adoption and sustainability of otherwise promising interventions. 19 Participatory action research (PAR) has been proposed as a means for systematically considering local needs and problems, thereby fostering stakeholder commitment and enhancing the likelihood of a particular intervention success.20–22 Few studies have actively engaged doctors in designing and implementing JTS to improve health care coordination. 20
This study sought to contribute to filling this knowledge gap. It was set in Colombia in the context of the 2016 Comprehensive Health Care Policy reform, which, among other things, sought to strengthen clinical coordination across health care levels by organising health services into integrated health care networks and introducing a shared EMR alongside existing feedback mechanisms (referral/reply letters, hospital discharge reports and clinical practice guidelines). 23 Available evidence suggests that while there has been greater use of feedback mechanisms to improve clinical information coordination in Colombia, there remain problems concerning the quality of the information being shared and the limited use of standardisation mechanisms.6,24,25 In this paper we report an analysis of the contribution of participatory action research (PAR) in designing and implementing joint training sessions as a means to improve clinical coordination in a public health care network of Bogotá (Colombia) from stakeholders’ perspectives.
Methods
This study was set in one of Bogotá’s District Health Department health services networks, which was selected based on the following criteria: the network had to provide a continuum of health care including at least primary and secondary care, to a defined population in a low/medium–low income urban area and be willing to participate in and implement the intervention. The selected network provided health services for 331,664 residents in 2017, of whom the majority (96%) were covered by the subsided insurance scheme, the remainder (4%) having no insurance coverage. 27 The study was part of the research project Equity-LA II, which evaluated the effectiveness of interventions to improve clinical coordination in health care networks in six Latin American countries. 26 It used a controlled before-and-after design involving one intervention and one control public health care network in each country. The project was developed in four phases: (1) a baseline study, (2) design and implementation of interventions, (3) evaluation of the interventions and (4) comparative cross-country analysis.
PAR approach to designing and implementing the joint training sessions
A local steering committee (LSC) was formed which included network representatives (health managers and professionals from different care levels) and the research team. The LSC was responsible for problem prioritisation, intervention selection, supporting intervention design and implementation as well as evaluating the process. Network representatives managed the necessary resources, such as freeing up human resources and securing meeting spaces, while the research team acted as facilitators and oversaw the research methods and network member training.
The process began with the baseline study, which produced evidence on problems regarding cross-level clinical information and clinical management coordination in the network.4,24 The findings were discussed with the network’s health professionals, managers and administrative staff (221 participants) in 24 workshops, leading to a preliminary selection of the most important problems of cross-level clinical coordination in the network. In the second phase, based on an in-depth analysis of the baseline results and using a reflexive approach, the LSC and four health care professionals identified two priority problems: lack of communication and disagreement between GPs and specialists concerning patients’ clinical management. To address these, the LSC selected joint training sessions (JTS) as the intervention, based on the available evidence and considerations about its feasibility and relevance. A working group (professionals’ platform, PP) was then formed by GPs and specialist doctors who had attended the workshops and were interested in participating in the intervention or who had been delegated to do so by the network. Together with the LSC, the PP designed and planned the JTS, including the method, topics, schedule, participants’ roles as well as monitoring and evaluation instruments (3 months). The implementation of the JTS was coordinated by the LSC and ran over 14 months (August 2016 to September 2017). The process involved two PAR cycles with the first 5 months including the setting up, implementing, monitoring and adjustment of the intervention’s content and method, which was followed by a second 9-month implementation cycle.
The intervention itself included two sets of JTS: JTS-PP run by and addressed to the PP (n = 14, 65 participants) and a ‘replica’ JTS (JTS-R) (n = 23, 208 participants). The latter was a short version of the JTS-PP, and run by a specialist in collaboration with a GP of the PP initially in each health centre. Box 1 summarises the main content and process of the JTS, with further details provided in the Online Supplement. Content and process of the joint training sessions. Joint training sessions (JTS-PP) to discuss clinical cases and ongoing training were run by GPs and specialists, who formed the professionals' platform (PP) sessions lasted 4 hours. The JTS-PP was divided into two parts. The first included the presentation of scientific evidence, readings concerned with diagnostic tests and training on treatment indications around the most common chronic conditions. In the second part, JTS participants discussed clinical cases to resolve queries about diagnosis, clinical management and referral to specialists using reflexive methods. This was accompanied by a specialist supporting the GP in preparing a particular case. The specialist presented the scientific evidence, promoted discussion among GPs and concluded with agreement about clinical management and learning during each session. Replication sessions of JTS (JTS-R) were conducted with other health professionals involved in the care of chronic patients in the network (GPs, specialists, nurses, etc). In the JTS-R, a summary of a specific topic was presented and the agreements established in the JTS-PP on the clinical case were discussed, A specialist ran the JTS-R in every health centre with a duration of 2hours. Fourteen JTS-PP were run with 65 health professionals participating (average participation of 15 doctors in the first and 17 in the second cycle). A total of 23 JTS-R were run with 208 health professionals participating (average participation of 20 health professionals in the first cycle and 33 in the second cycle).
Study design and sample
Study participants.
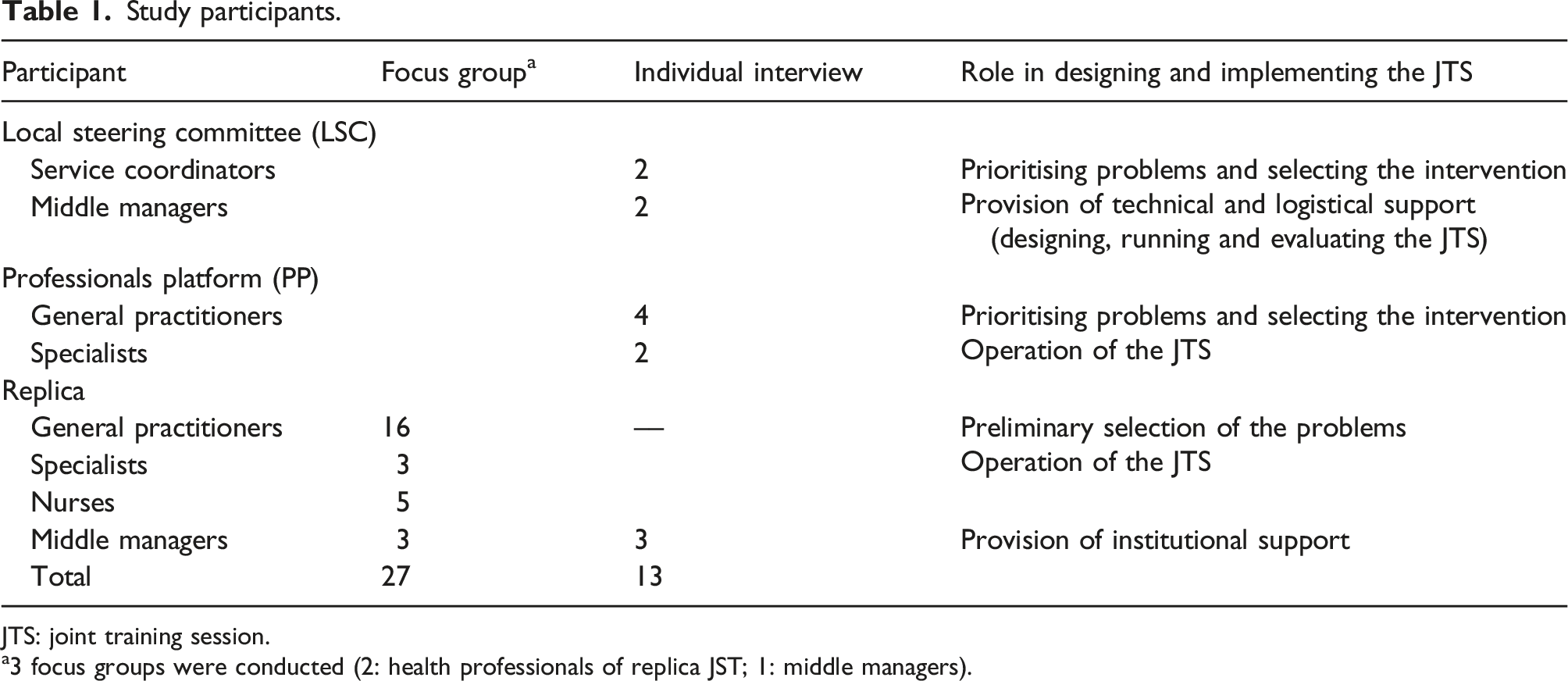
JTS: joint training session.
a3 focus groups were conducted (2: health professionals of replica JST; 1: middle managers).
Data collection
Data were collected using focus group discussions and semi-structured individual interviews. Topic guides explored views on the intervention process, from identifying the problem/s and intervention design, planning and dissemination, monitoring and evaluation, participants’ roles, and the characteristics of the intervention itself in terms of content and methodology. Potential study participants were identified from JTS attendance records and then invited to participate by email and phone. The fieldwork was carried out between November 2017 and May 2018 at participants’ workplaces. Individual interviews lasted around 60 min and focus groups 90 min; they were recorded and transcribed verbatim.
Data analysis
Interview and focus group data were analysed thematically using Atlas.ti 7.5 software. Data was segmented by participant group, type of intervention and phase. We used an inductive approach to data coding, guided by the topic guides and themes identified in this process. Common patterns were established and data regularities, convergence and divergence analysed by constant comparison and returning to the data. 28
Information was triangulated between semi-structured individual interviews and focus groups and contrasted with data from previous studies and discussed with informants. Preliminary findings were presented and discussed with intervention participants, with views taken into account in the final analysis. Furthermore, five analysts (two international and three national) collaborated in data analysis; differences arising during analysis were resolved by returning to the data and discussed until reaching agreement. The analysts had varied backgrounds regarding health and social sciences and in-depth knowledge of qualitative methods, the analytical framework, the research topic and context to ensure that the contextual characteristics of the local health and social system were taken into account.
Ethics approval
The study was approved by the Universidad del Rosario’s School of Medicine and Health Science’s Ethics Committee. Confidentiality agreements were signed with participating institutions. All participants signed an informed consent form. The recordings and transcripts were coded to maintain informants’ anonymity.
Results
Study participants identified the PAR approach and actors’ (LSC and PP) role in designing and implementing the JTS as fundamental elements for adapting the intervention and its penetration in the target network. However, they also identified a range of facilitators and barriers in the PAR process, such as appropriate LSC leadership during each PAR cycle and adequate monitoring and evaluation of JTS, as well as the limited institutional support and dissemination of the intervention in the network. We discuss these issues in turn.
Designing and implementing joint training sessions between GP and specialists
Most study participants considered the design process to be participative since it involved GPs and specialists and reflexive discussion of the challenges around cross-level clinical coordination that were identified at baseline. This was perceived to have led to greater awareness of the selected problems: A diagnosis of medical activity was presented to all the network’s health professionals and we realised that this was how things were; we became aware of these problems… (GP-PP, interview) (Online Supplement Table S1, A1).
According to LSC members and GP-PP, health care professionals’ involvement in designing the intervention facilitated adapting the JTS to their needs. Moreover, there was a perception that doctors involved felt recognised and valued (particularly GPs), leading to greater interest in and commitment to implementing them: Regarding the talks with colleagues, first we felt appreciated, because for the first time they asked the GP; regarding the specialists, equality with them was sought regarding scientific aspects… we felt valued and this was important, that human beings felt recognised. (GP-PP, interview) (Online Supplement Table S1, A2)
LSC members highlighted the importance of having been trained in research methods to facilitate decision-making: It was a very positive aspect for the LSC because, as each stage was developed, training with the research team was carried out regarding the topics included in each stage with the research team. This helped us a lot to know how to support the processes in the most correct way. (LCS member, interview)
Most participants highlighted the openness, dynamism and flexibility of the PAR approach to implementing JTS since it enabled adjusting the method, for example, by including questions to help GPs improve their analysis of clinical cases and contents regarding the needs identified by participating doctors through ongoing monitoring (Online Supplement Table S1, B1).
Study participants also appreciated the LSC’s role in securing space and professionals’ time for the dissemination of baseline results and when implementing the JTS in each health centre, and the preliminary identification of problems and improvement strategies. LSC members considered that the work of the research team on the systematisation and monitoring of the JTS was essential (Online Supplement Table S1, B2-B3). They [LSC] were responsible for moving human resources within the centre; there was definitively a commitment to convene the doctors. So the LSC member was the person who had to do everything; it was up to all of us, but this delegate showed much more commitment to respond to what the project needed. (Middle manager, interview).
At the same time, it was not always possible to secure institutional support and, thus, doctors’ participation. LSC members and managers highlighted that managers’ frequent rotation had led to changes in LSC membership, restrictions on releasing GP-time for participating in the JTS-PP and reducing the time available for implementing JTS-R (Online Supplement Table S1, B4). Likewise, the high turnover of GPs due to contractual constraints (such as being on a temporary contract or working part-time), limited their motivation and participation: Service provision hiring has led to greatly increased rotation of professionals in different institutions and such high rotation rate means that there is no adherence/commitment to different processes, such as training sessions/meetings… thereby hampering this type of process’ traceability. (Middle manager, interview)
LSC members further noted that the limited use of network media, such as the intranet, email or noticeboards, hindered the broader dissemination of the intervention (Online Supplement Table S1, C1).
GP-PP and LSC members commented on the use of qualitative research techniques for monitoring the JTS, which had enabled participants to identify difficulties and address them according to their needs by adjusting the JTS: I think the evaluation was good because everyone gave their perception of the process, as we are doing now. I think it was suitable; the questions led to identifying the difficulties and corrections to be made. I think it was good. (GP-PP, interview)
However, managers and specialist-PP considered that the knowledge acquired by doctors and the changes regarding quality of care should be evaluated (Online Supplement Table S1, D1-D2).
Characteristics of the joint training sessions of GP and specialists
There was agreement among study participants that the approach used by the JTS-PP, that is, discussing clinical cases based on doctors’ reflection on their own practices, worked better than that used in the replica JTS. It was felt that the former promoted interaction and trust between doctors, thereby facilitating knowledge exchange and progressive increase in GP participation: I think that the problem-based learning methodology was very enriching because it elicited experience from/for the doctors, and when one learns through experience, as in clinical casuistry, then one learns much more. (Specialist-PP, interview) (Online Supplement Table S1, E1-E2)
There was a perception that in the replica JTS there was less opportunity to adopt a reflexive approach due to a combination of less time available and the larger number of participants; this was seen to have limited interaction between doctors and their participation in the discussion of clinical cases (Online Supplement Table S1, F1-F2).
The progressive increase in participation in JTS-PP and, to lesser extent, the replica JTS was attributed to the JTS providing an opportunity for a cross-level group of doctors to share the same space, thereby promoting interaction and confidence in voicing their concerns: One feels a certain fear when expressing doubts, but when these are expressed during team or group sessions then one can do so more calmly and feel the solidarity of other professionals and begins to talk, and when someone talks, then the others reflect on or remember other thing and this triggers a chain reaction, leading to very good participation in the end. (GP-PP, interview)
However, replica JTS were often incorporated within administrative meetings, which occasionally delayed the start and influenced doctors’ interest in participating fully, mainly because of administrative issues, such as renewing contracts or reducing salaries (Online Supplement Table S1, F3).
There was widespread agreement about the importance of the facilitator’s role in the JTS, which was seen to motivate GP participation. The facilitators’ communicative and paedagogical abilities, knowledge of the chosen topic, empathy and mutual respect were seen to be essential for the suitable use of the reflexive method and interaction among doctors during the JTS (Online Supplement Table S1, G1).
While the length of the JTS-PP was generally considered to be appropriate, that of replica JTS was seen to be less so, particularly by the end of the second PAR cycle. There was a perception that the latter only permitted synthesising a particular topic or clinical case to be discussed, followed by a very short discussion regarding the conclusions and agreement concerning the clinical case (Online Supplement Table S1, H1). GP-PP noted that insufficient time had been allocated for preparing a given clinical case and that they usually had to prepare them outside their normal working hours (Online Supplement Table S1, H2-H5).
Most participants found the topics discussed in the JTS to be pertinent and relevant. Those initially selected were in line with the network’s morbidity profile and these were later adapted to other needs expressed by GPs regarding clinical management and follow-up of chronic patients in primary care: The most frequently occurring diseases - hypertension, diabetes, chronic obstructive pulmonary disease – are those which we see every day, which one sees frequently during consultation and where we experience difficulties concerning managing them and follow-up. (GP-PP, interview)
Finally, there was some concern about the limited participation of other network specialists’ in the JTS, which was attributed to lack of allocated time allowing specialists join. This was seen to have limited discussion of more complex clinical cases, which require input from a broader range of specialists (Online Supplement Table S1, I1).
Discussion
This study provides evidence contributing towards the design of and introducing joint training sessions to improve clinical coordination between health care levels in Colombia and elsewhere. The findings highlight the importance of involving key stakeholders in designing and implementing joint training sessions for GPs and specialists using a participatory approach, which allowed for adaptation of the intervention to the health care network context. However, challenges such as limited institutional support and different approaches to delivering the intervention (JTS-PP and replica JTS) influenced the participation of GPs, while the characteristics of the intervention itself, such as session duration, the role and abilities of facilitators along with the content were seen to be fundamental for using the reflexive method and ensuring GP participation. Limited involvement of other network specialists reduced the scope of JTS to also analyse more complex clinical cases.
The findings suggest that involving frontline doctors in the design, setting up and evaluation of JTS created favourable conditions for implementing the training sessions, generating greater interest and commitment among GPs, as has been shown elsewhere.20–22 The study also highlighted the crucial role of institutional support for releasing doctors’ time for participating in the intervention’s design and implementation.21,29 Doctors’ precarious working conditions, such as temporary or part-time contracts, restricted their full involvement in JTS. This may have reduced the impact of joint training on communication and on agreement on clinical management between care levels as identified in previous studies.6,24
The findings further highlight the importance of appropriate leadership (here: research team and institutional representatives) to orientate each PAR cycle and acting as mediator between institutional managers and health professionals. This type of leadership is particularly important in an institutional setting characterised by (frequent) organisational change due to wider policy changes. The cycles of action, ongoing monitoring and adjustment facilitated the adaptation of the JTS method and content to emerging needs identified by participating doctors, thereby enhancing the ability of JTS to achieve their objectives and sustainability in the health care network.
An important observation was that the JTS-PP appears to have had greater impact on GPs’ interaction and confidence than the replica JTS. This was attributed to better implementation of the reflexive method in JTS-PP, leading to greater GP participation as it allowed them to analyse their own clinical practice and consolidate as a group, thereby promoting greater collaboration.14,17 This was limited in replica JTS due to shorter duration, greater group size and sessions being incorporated within broader administrative meetings, thus reducing their effectiveness. These findings highlight the importance of group size and the allocation of protected time to programming, in terms of duration and space, to optimise delivery and enhance participation. Similarly important are the actual session content and the skills of the facilitator to ensure participants maintain an interest and actively contribute, which is likely to further promote the effectiveness of joint training.12,17
The limited involvement of a diverse group of specialists is likely to have reduced the effectiveness of JTS, in that specific clinical areas that are important in the primary care setting, such as complex multimorbid patients, were less likely to be addressed, or not addressed in great depth. Similarly, although there was institutional support to protect doctors’ time to participate in JTS, preparing for sessions in terms of presenting a specific clinical case usually had to be performed in the GP’s own time, that is, outside working hours. This further reinforced the need for strong institutional and wider system support to free up doctors’ time for appropriate activities, which in the current context of managed competition in Colombia, is often challenging, requiring health care providers to prioritise doctors’ time for clinical activities.6,24
The findings strongly suggest that the effective use of participatory action research in the design and implementation of joint training sessions to improve care coordination require frequent and direct communication with management to ensure that the necessary resources are being made available. Effective strategies must be identified to ensure that those involved (managers, service coordinators and doctors) will have their time protected to ensure their effective participation in interventions, orientated by a leadership having the necessary technical knowledge for implementing the approach and act as a link between health care staff and management. Suitable conditions must be maintained for implementing JTS effectively, considering meeting duration, group size and the space for their development. JTS content must be updated and relevant and reflexive learning methods used.
Study limitations
Managers and LSC and PP members’ turnover prevented study participants from developing a complete experience regarding designing and implementing JTS and, in some cases, of the latest phases of the process. Although this limitation was addressed by carrying out interviews with participants of each phase, this could have had repercussions on the depth or completeness of the data collected for example, the adjustments made to the JTS may not have been clearly identified.
Conclusions
This study contributes towards filling a gap related to PAR’s contribution to designing and implementing interventions for improving clinical coordination between health care levels. We found that involving doctors in designing, implementing and evaluating the interventions is an essential element for its adaptation to local context and needs for sustainability. It highlights the importance of LSC leadership and of institutional support to facilitate PAR implementation and ensuring that the necessary resources are available for adopting the intervention. The findings can inform similar approaches in other health systems.
Supplemental Material
sj-pdf-1-hsr-10.1177_13558196221094676 – Supplemental Material for Implementing joint training sessions of general practitioners and specialists aimed at improving clinical coordination in Colombia: Contributions from participatory action research
Supplemental Material, sj-pdf-1-hsr-10.1177_13558196221094676 for Implementing joint training sessions of general practitioners and specialists aimed at improving clinical coordination in Colombia: Contributions from participatory action research by Heisel León-Arce, Josefina Chávez Chávez, Amparo-Susana, Mogollón-Pérez, Ingrid Vargas and María-Luisa Vázquez in Journal of Health Services Research & Policy
Footnotes
Acknowledgements
The authors are most grateful to the LSC, PP, professionals and middle managers of the network and research team who participated in the study and generously shared their effort, time and opinions for improving the quality of the health care being provided. The authors thank Jason Garry for the English version of this article and the European Commission for funding this research. This article was produced within the framework of the Doctorate in Department Paediatrics, Obstetrics and Gynaecology, Preventive Medicine and Public Health of the Universitat Autònoma de Barcelona, Spain.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by European Commission Seventh Framework Programme (FP7/2007–2013) under grant agreement number [305197].
Ethics approval
Universidad del Rosario’s School of Medicine and Health Science’s Ethics Committee, approval number CEI-ABN026-000173.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.