
Abstract
Objective
In 2014, the Primary Care Plus (PC+) model was introduced in the Netherlands to shift low-complex specialised care from the hospital to the primary care setting. While positive effects of PC+ have been documented at individual patient level concerning health-related quality of life, perceived quality of care and care costs, its impacts on service use at the population level remain uncertain.
Methods
In this observational study, we used retrospective health insurance reimbursement claims data from the largest health insurer in the intervention region to determine service use. We assessed PC+ and secondary care insurance claims (i.e. claims of the regional hospital and claims of other secondary care settings in and outside the region visited by patients from the intervention region) from 2015 to 2018 and compared these to the national level.
Results
The total number of claims related to low-complex specialised care in the intervention region showed an increase over time. The increase in claims was related to PC+. The number of claims related to the regional hospital and other secondary care settings decreased over time. During the same period, a declining trend in claims at the national level was observed.
Conclusion
The introduction of the PC+ model in one region in the Netherlands was associated with an increase in the use of low-complex specialised care. This suggests that the ability of the PC+ model to substitute for specialist care at population level may be limited. Going forward, it will be important to continue monitoring and evaluating service use as substitution effects may materialise only over a longer timeframe.
Introduction
Controlling health care costs remains a major challenge for health care systems. 1 Countries are experimenting with new ways to deliver high-quality care at acceptable costs, with a major emphasis on shifting some care out of hospitals into the community. 2 Such approaches are expected to improve access to quality care and increase the effectiveness and efficiency of health services. Examples include discharge from outpatient to primary care, shifted outpatient clinics, specialist attachment to primary care teams and joint consultations. 3 Existing studies point to positive impacts of related initiatives on the quality of care for many conditions and on patient experience, 4 while evidence on their cost-effectiveness remains uncertain.
In the Netherlands, the creation of regional collaboration initiatives in 2013 aimed to achieve better health care at lower cost by focussing on the substitution of hospital care with primary care. One of these initiatives is Primary Care Plus (PC+), which seeks to shift the care for low-complex and non-acute patients from the hospital to a lower cost-per-unit setting through relocating hospital specialists into a primary care setting.5,6 Existing studies of the effects of PC+ found that patient health and the quality of care were maintained or even improved, 7 while also lowering costs per patient compared to usual care because of lower overheads and resource use. 8
Less is known about the impact of PC+ on service use at population level and this exploratory study aims to help fill this evidence gap. Specifically, we sought to understand the degree to which PC+ succeeded in substituting outpatient hospital care at a population (or regional) level.
Mechanisms for substitution or addition
There are several possible mechanisms by which PC+ could substitute for specialist services. 9 Embedding specialist knowledge into primary care could lead to earlier detection of potential serious disease and reduce the need for referral to outpatient specialist care. 10 Also, moving specialists closer to GPs could encourage interaction and communication, helping GPs acquire more specialist expertise, 3 which could potentially also reduce the need referral to specialist care. 11 On the other hand, PC+ could simply complement the existing service offering, thereby increasing service use and costs. 12 For example, evidence suggests that a considerable proportion of patients seen by specialists in primary care need to be seen again in hospital, 4 thus duplicating service use and, consequently, cost. Also, ready availability of specialist knowledge in PC+ may increase use of these services where GP thresholds for referral are lowered (supplier-induced demand). 13
Methods
Setting
The PC+ intervention investigated in this study is located in the Maastricht-Heuvelland region in the Netherlands. The region’s resident population of around 170,000 is served by 81 GPs (2019) working in 55 GP practices. It is characterised by lower labour participation, higher prevalence of health risk factors such as smoking and physical inactivity, and a higher proportion of people with a only primary education compared to the rest of the country. 14 PC+ was developed within a partnership between the primary care organisation Care in Development (Zorg In Ontwikkeling, ZIO), the Maastricht University Medical Centre (MUMC+), the patient representative foundation ‘Burgerkracht Limburg’ and the health insurer VGZ. Established in 2014, PC+ comprises two independent centres located outside the hospital premises and owned by Maastricht UMC+ and ZIO, where hospital specialists (employed by MUMC) perform consultations for people with non-acute and low-complex health problems (see also Box). GPs in the region are able to refer patients to PC+ in the same way as referring patients to outpatient hospital care. After consultation in PC+, patients are referred back to their GP with treatment advice, which may include referring the patient on to hospital care when further diagnosis and/or treatment is needed.
As PC+ is located in the primary care setting, specialist consultations are fully covered by health insurance. In contrast to regular outpatient specialist consultations, which requires a compulsory deductible (ranging from €375 to €385 during the study period),
15
no such deductible is levied on PC+ consultations. Reimbursement of a PC+ consultation is on a fee-for-service basis with a fixed price per consultation, regardless of medical specialty. The fixed price is calculated as a weighted average of the price of health care products that have been determined to be suitable for substitution to PC+. In this way, care can be offered at a lower price in PC+ than in secondary care. The reimbursement of care delivered in PC+ differs from the reimbursement of hospital care, for which a detailed hospital product classification system has been used since 2005, in which each patient is categorized into a Diagnosis Treatment Combination (DTC). These DTCs include all hospital activities and services (both inpatient and outpatient) associated with the patient’s demand for care from the initial to the final consultation or examination. Hospitals receive a payment per DTC that has been agreed upon with the insurer.Box 1. Payment for PC+ services
Data
Number of patient visits to PC+ by medical specialty, 2015–2018 (N = 22,136).
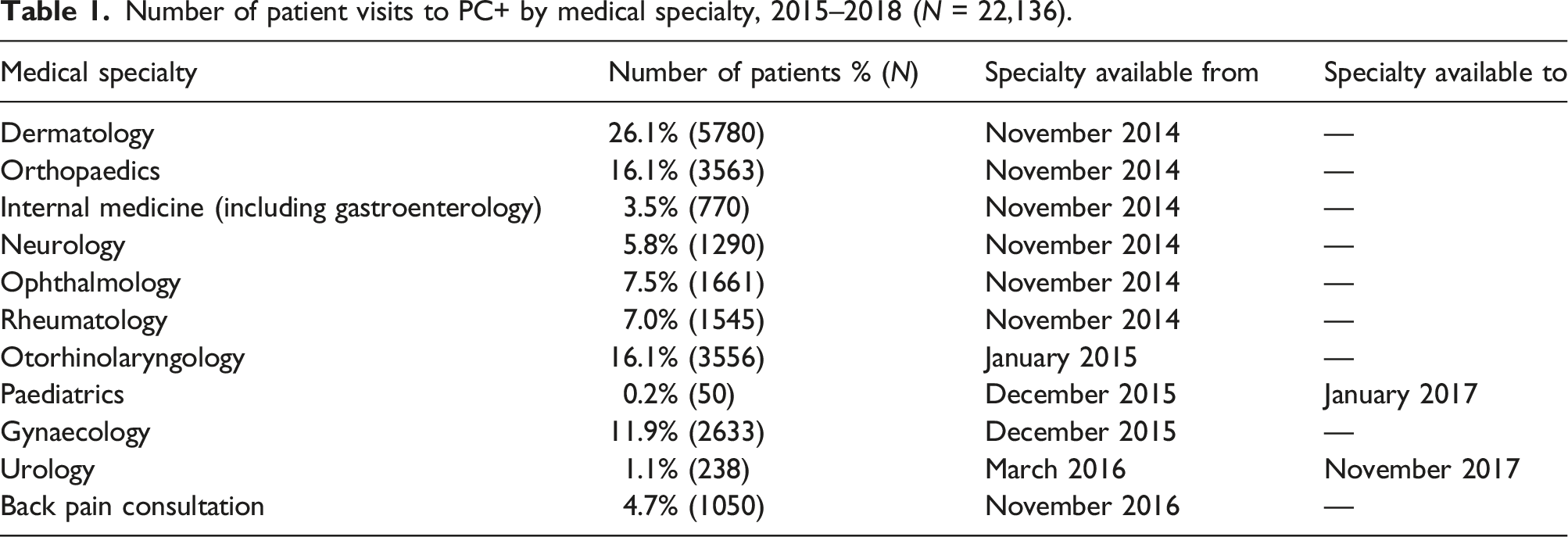
We used retrospective health insurance reimbursement claims data from VGZ to assess PC+ and secondary care utilisation for 2015–2018 and compared these to national data on service use. We included all claims that related to referring GPs in the intervention region. For secondary care use, we included claims for low-complex initial hospital care (usually involving one or two consultations with a medical specialist) suitable for substitution to PC+ based on the DTC system (Box). Only DTCs related to a medical specialty present in PC+ during the study period were selected (Table 1). The annual number of claims was adjusted for the number of registered insured persons to calculate the number of claims per 1000 insured. To compare the number of low-complex specialist consultations in the intervention region with the Dutch average over time, we used VGZ data for the rest of the Netherlands, applying the same inclusion criteria. We further used data from ZIO and Statistics Netherlands to calculate the annual number of residents in the intervention region and the rest of the Netherlands. These figures were then used to calculate the annual percentage of VGZ-insured persons.
Results
Population and low-complex specialised care claims in the intervention region and nationally, 2015–2018.
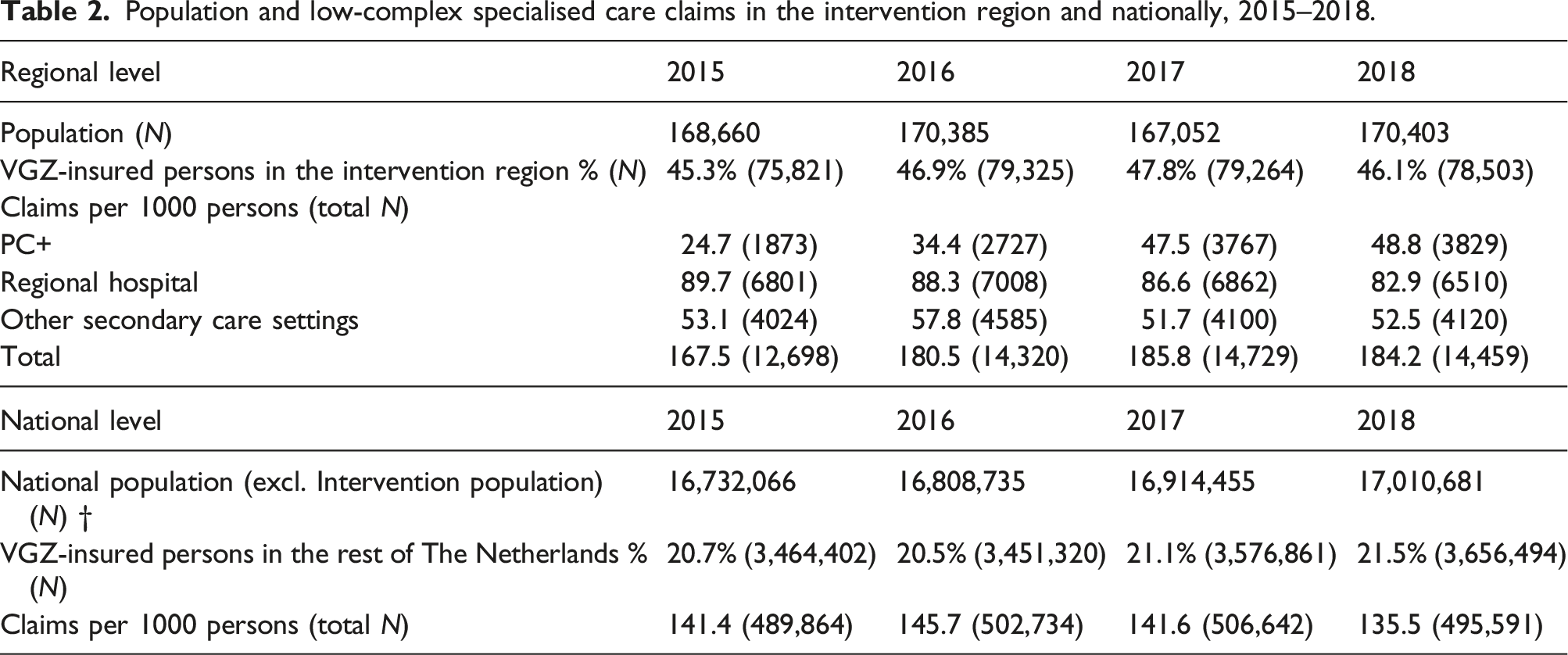
In the intervention region, the total number of claims per 1000 insured for low-complex specialised care rose from 167.5 in 2015 to 184.2 in 2018. This is in contrast to the rest of the Netherlands, where the total number of claims fell from 141.1 per 1000 insured in 2015 to 135.5 in 2018. The observed increase in the intervention region was due, in large part, to PC+ consultations, which doubled during the study period, from 24.7 claims per 1000 in 2015 to 48.8 in 2018. At the same time, claims for regional hospital care fell from 89.7 per 1000 in 2015 to 82.9 in 2018 while those for other secondary care settings remained fairly stable.
The observed changes over time are further illustrated in Figure 1, which shows the trend in the number of claims per 1000 insured for low-complex specialised care in the intervention region and the rest of the Netherlands. This suggests that the rise in the total number of claims in the intervention region increased more strongly in the first two years following the introduction of PC+ and appeared to stabilise towards the end of the study period. This is mirrored by a stronger increase in the number of PC+ claims from 2015 to 2017, and subsequent levelling off. The fall in the number of claims per 1000 insured for the regional hospital appears to follow the national trend, while claims for other secondary care services first rose and then fell again, to be on par with PC+ claims at the end of the study period. Trends in low-complex specialised care claims per 1000 VGZ-insured persons from 2015 to 2018.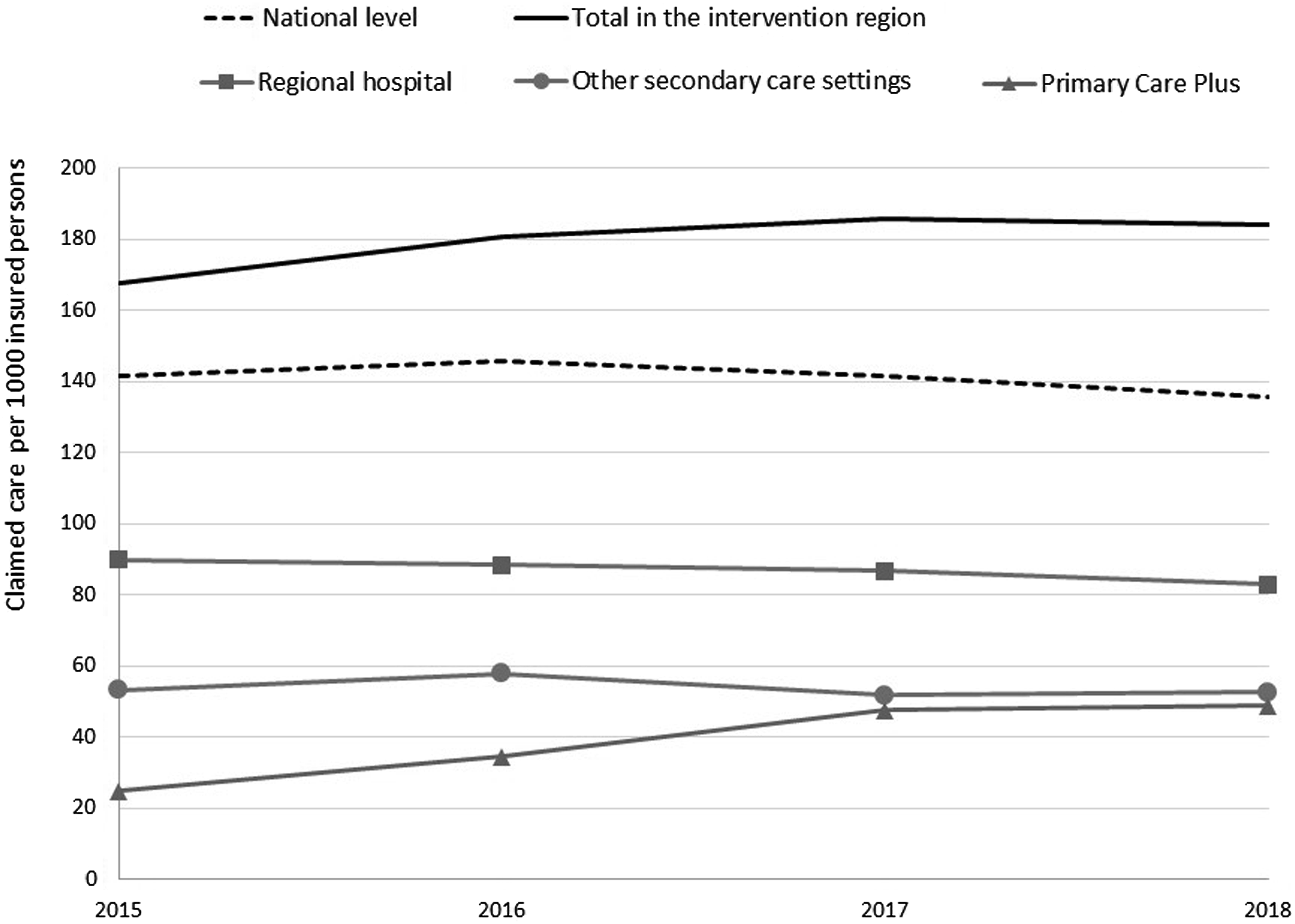
Discussion
This study found that the introduction of the PC+ model in one region in the Netherlands was associated with an increase in the use of low-complex specialised care. This suggests that the new model, which sought to move more specialised care into the community, was only partly able to substitute for hospital care. Rather, our observations seem to suggest that PC+ constitutes a complementary offering for secondary care services in addition to those provided by the regional hospital and other secondary care services in the intervention region.
Strengths and limitations
Our analysis is based on health insurance claims data, which have well documented limitations in that they were not originally acquired for research purposes. 16 We were unable to trace medical specialty referrals from the PC+ claims data and it was therefore not possible to assess trends in consultations by medical specialty or to adjust for changes in the composition of medical specialties during the study period. We would expect that these differences will affect the number of consultations in PC+; indeed, we found that four specialties were responsible for 70% of the patients seen in PC+ (Table 1). This suggests that different medical specialties may be more or less suitable for substitution of care to PC+, which might also affect service use. We were unable to link the data with other sources to investigate this issue further because of data confidentiality.
In addition, we only used claims data from PC+ and secondary care. It would have been illustrative to also consider primary care claims data given that the majority of patients referred to PC+ would be referred back to their GP following PC+ consultation. We would expect PC+ to also affect service use in primary care, and the increasing service use associated with the introduction by PC+ may be underestimated in this study.
We used claims data from only one health insurer. Although VGZ has the largest market share in the intervention region, it only covered about half of the resident population, and it is not clear to what extent the study population is representative of the total population in the intervention region. The same applies to the population in the rest of the Netherlands, where the share of VGZ-insured persons is lower than in the intervention region. Claims data from a wider range of health insurers might increase generalisability. However, because of the complexity of linking multiple data sources, only data from one insurer was used. 16
We noted earlier that the population in the intervention region had a worse health profile than the rest of the Netherlands, 14 and this might explain the higher overall level of service use in the intervention region. As this was an exploratory study, we were unable to adjust our analysis for population characteristics such as age, gender, or health or socio-economic status. Further (qualitative) research is needed to understand what is actually occurring in the region. Finally, this study only considered service use and further research should also investigate associated costs. While use of low-complex specialised care may have increased in the intervention region, the lower cost per patient in PC+ may still lead to cost savings at population level.
Implications and recommendations
This study highlights the importance of continuous evaluation of interventions such as PC+ at population level to help inform service development and intervention modification if necessary. 17 Such evaluation is the more important given the time it takes for integrated care interventions to demonstrate effectiveness, 18 frequently requiring complex cultural and organisational change to deliver care differently. 19 Longitudinal dynamic evaluation over a longer period of time to assess the impact on outcomes, such as costs of care, health care use and health-related outcomes, may be needed. 20 The follow-up period in this study might have been too short to demonstrate whether PC+ resulted in a substitution of care; 21 the slightly decrease in service utilisation in the intervention region in 2018 points to likely substitution.
Conclusion
The evidence presented in this study suggests that the ability of the PC+ model to substitute for specialist care at population level may be limited. Going forward, it will be important to continue monitoring and evaluating service use as substitution effects may materialise only over a longer timeframe.
Footnotes
Acknowledgements
We acknowledge employees from health insurance company VGZ for their contribution in providing us with data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Medical Research and Ethics Committee of Maastricht University Medical Centre (METC 14-4-136).