
Abstract
Objectives
Pharmaceutical incentivisation of physicians for profit maximisation is a well-documented health system challenge. This study examined general practitioners’ (GPs) reactions to pharmaceutical incentivisation offers in one region in Pakistan.
Methods
We used the Standardised Pharmaceutical Sales Representative (SPSR) method and qualitative interviews with GPs. SPSRs were field researchers representing mock pharmaceutical companies who recorded their observations of 267 GPs’ responses to pharmaceutical incentivisation offers. We triangulated SPSR data using qualitative interviews with a subset of the same GPs to gather information about how they interpreted different interaction outcomes.
Results
We found four major outcomes for GPs being offered incentives by pharmaceutical companies for prescribing medications. GPs might agree to make incentivisation deals, reject incentivisation offers, disallow PSRs to access them, or remain indeterminate with no clear indication of acceptance or rejection of incentivisation offers. GPs rejecting SPSRs’ incentivisation offers indicated having active commitments to other pharmaceutical companies, not being able to work with unheard-of companies, and asking SPSRs to return later.
Conclusions
The GP-pharmaceutical sales representative interaction that centres on profit-maximisation is complex as offers to engage in prescribing for mutual financial benefit are not taken up immediately. The SPSR method helps understand the extent of distortion of practices impacted by incentivisation. Such an understanding can support the development of strategies to control unethical behaviours.
Introduction
Pharmaceutical companies tend to allocate significant budgets to promote their products through advertisements and direct contact with physicians. 1 Pharmaceutical sales representatives (PSR) play a crucial role in orienting physicians’ attention to their products and company incentives offers for prescribing these.2,3 In 2020 alone, marketing costs exceeded research and development costs by USD 36 billion for the seven highest revenue-generating pharmaceutical companies; a major component was spent on incentives for physicians. 4 Incentives include direct monetary benefits and sponsorships of medical education activities,5–7 and there is a concern that this could distort physicians’ prescribing behaviour, as they might prioritise prescribing products from sponsoring companies. 8 PSRs typically act as mediators,9–11 with evidence of altered prescribing behaviour following physicians’ interaction with PSRs 12 and that benefits linked to prescriptions may outweigh considerations of patients’ health and wellbeing. 13 Our research in Pakistan identified a range of other incentive types, including items for physicians’ personal use, for their clinic/home renovation, and coverage of the cost of family events (i.e., birthdays, marriage ceremonies, and children’s schooling). 14 Thus incentivised physicians are likely to prescribe unnecessary or expensive medications, and this practice may negatively affect patients’ health and/or financial situation. 15
The strategies that PSRs adopt to build strong and persuasive relationships with physicians are not well understood. Existing studies have tended to focus on physicians’ medical skills, prescribing behaviours (particularly, unnecessary prescribing of medications), and medical errors,16–18 rather than examining in depth the interactions between physicians and PSRs. This study seeks to contribute to closing this gap by examining incentive-related interactions between general practitioners (GPs) and PSRs in Pakistan. Pakistan has a strong pharmaceutical industry, valued at USD 3.2 billion in 2021, gradually increasing by 15% per annum and accounting for almost 1% of the country’s national income.19,20 There are almost 650 pharmaceutical companies registered with the Drug Regulatory Authority of Pakistan (DRAP), including 30 multinationals. 20 In addition, there is a significant number of unregistered pharmaceutical companies that also operate in Pakistan and which contribute to the use of substandard medications driven by profit-led prescribing. 21
Our study sought to understand GPs’ reactions to incentivising offers from PSRs representing new and unpopular local pharmaceutical companies, the types of jargon or terms GPs and PSRs use to negotiate incentivisation deals, and the measures that could be adopted to reduce pharmaceutical incentivisation to GPs.
Methods
We collected data using (i) the Standardised Pharmaceutical Sales Representative (SPSR) method and (ii) qualitative interviews with GPs. In 2021, we conducted a baseline survey in Karachi to collect basic demographic information about GPs and assess their knowledge of and attitudes towards incentive-linked prescribing. A total of 422 GPs were systematically sampled from an official list of 1695 GPs, of which 419 (99.2%) consented to participate in the survey. Trained data collectors met with all the sampled GPs in person, and upon completion of the survey, invited them to participate in a follow-up study observing their interactions with PSRs. In the follow-up study, 267 GPs participated.
The SPSR method is an innovative extension of the ‘standardised patient’ (SP), which is considered a gold standard for assessing the quality of care in health care settings. 22 In brief, the method involves members of local communities who are extensively trained to present with predefined health conditions to health care providers as a means to assess how providers address these health conditions. Similarly, our research used trained field researchers who acted as PSRs representing fictitious pharmaceutical companies, offered incentives to GPs and observed GPs’ reactions.
We trained a total of 15 SPSRs who presented at GP clinics as PSRs from new domestic pharmaceutical franchise companies looking to expand the market share of their various pharmaceutical products including antibiotics, painkillers, and multivitamins. As noted above, in Pakistan franchises are typically small-scale drug promotion-based companies, which procure pharmaceutical products from manufacturers and sell them under their unique brand names; the franchise may or may not be registered with DRAP. Pharmaceutical businesses and medical practices tend to consider pharmaceutical franchises as less credible as they tend to market low-quality medicines and use incentives as a major marketing tool.
We divided the SPSRs into three subgroups, each comprising five SPSRs that represented different pharmaceutical companies. SPSRs assessed the behaviour of GPs by interacting with them in their clinics in the way that ‘regular’ PSRs would. SPSRs carried drug information briefs and a list of 10 medications (Online Supplement) including three antibiotics, two painkillers, four multivitamins, and one cough syrup. To initiate the interaction, the SPSR approached GP clinics and, when called in, recited a script, which the research team had developed in consultation with a pharmaceutical marketing expert (Box). Upon completion of each interaction, the SPSRs immediately completed a structured questionnaire that also contained a free-text box for SPSRs to record qualitative information. Hello doctor! My name is XYZ. I am visiting from a new pharmaceutical franchise company called Remedium Pharma/Genezing pharma/Gamot pharma. I have come here to tell you about the pharmaceutical products that my company offers. I would be happy to do something for you if you could prescribe our products. Our franchise has these products (show list or summarise list). Can you please see them and let me know, which products you would like to prescribe to your patients? We are doing an excellent job in Lahore, and now we want to increase our sales in Karachi. May I know what support can I get from you? Building this relationship will have some mutual benefits – if you prescribe our products, our franchise will be happy to give you benefits of your choice, and this can also enable us to penetrate Karachi’s market. This is also a new job for me, and it would be great if we can both support each other to be successful. Is there anything I could do for you to encourage you to prescribe my company’s products?Box: SPSR script used for interacting with GPs
Standardised Pharmaceutical Sales Representative visits to all 267 GPs who participated in the follow-up study were completed between July and August 2022. Three SPSR teams, each comprising five members, were assigned to visit GPs in six different major areas of the city: East, West, South, Central, Korangi, and Malir. Each SPSR was allowed to pay a maximum of three visits to each assigned GP, as a higher number of interactions might have led the GP to suspect that SPSRs were not regular PSRs. SPSRs visited all GP clinics at least once, including visits in which the interaction between GPs and PSRs might or might not have happened. A total of 63 GPs were visited twice, and three GPs three times. There was one case where the SPSR conducted a fourth visit because we considered the first visit to be invalid as the GP had been away for a few days.
From October to November 2022, we conducted a qualitative study with 30 GPs, who were part of the follow-up study and the SPSR assessment. By conducting a preliminary analysis of the SPSR assessment data, we first grouped GPs into different categories based on their acceptance, rejection, or vague responses to SPSRs’ incentivisation offers. Within each category, we purposively selected 10 GPs. A qualitative researcher then contacted all 30 GPs by telephone to schedule in-person meetings and conduct interviews. At this phase of the study, the GPs had good awareness of the research team and the study due to repeated interactions from the baseline survey as well as the follow-up study; all 30 GPs whom we contacted agreed to be interviewed. All interviews were conducted in Urdu language. The duration of the interviews ranged from 45 to 60 min. Interviews sought to explore GPs’ perspectives on pharmaceutical incentives and their attitude to engaging with specific companies and PSRs.
Data analysis included text notes in free text fields of the SPSR questionnaire and semi-structured interview transcripts. Using both NVivo (version 12) and manual coding, the research team developed codes that were organised into three major outcomes: agreeing, rejecting, and undetermined. In the latter category, we identified various other pieces of information about GPs’ engagement with other companies, refusing to work with specific companies, and ignoring PSRs. To maintain confidentiality, while quoting excerpts from the interviews, we masked the individual identities of participants by assigning them unique identity codes, generated through a combination of the initials of the participant category, name, and the number of the interview.
Ethics approval
Ethics approval was obtained from the Pakistan National Bioethics Committee (# 4-87/NBC-582/21/1364), the Ethics Review Committees of the Aga Khan University (# 2020-4759-1129), and the London School of Hygiene and Tropical Medicine. After being provided with an information sheet, all GPs gave their written consent to be studied for their interactions with PSRs. Key ethical guidelines about voluntary participation and maintaining participants’ confidentiality were observed throughout the research process.
Results
Standardised Pharmaceutical Sales Representatives approached 267 GPs, of which 85% were male and 15% were female. Some 17% of the GPs reported providing health care in at least two primary care settings, a government-run hospital and a private independent clinic; GPs’ average age was 54.6 (SD:10.3) years.
Figure 1 shows four different outcomes of incentivisation offers with respect to the number of visits SPSRs paid to GPs. A total of 94 (35%) GPs did accept incentivisation offers from SPSRs; almost three-quarters (n = 69; 73%) did so on the first interaction. More than half (n = 157; 59%) rejected incentivisation offers by SPSR; again the majority (n = 121) did so at the first interaction. Some 5% (n = 13) were not accessible either because they were away for a long period or they did not meet PSRs. It was not possible to classify responses as accept or reject for n = 3 (1%) GPs. These GPs asked to see drug samples before talking about their potential engagement and were excluded from further visits as SPSRs did not carry drug samples and to minimise the risk that these GPs would recognise that the SPSRs were not regular PSRs. Distribution of GPs with respect to outcomes and the number of interactions with SPSRs.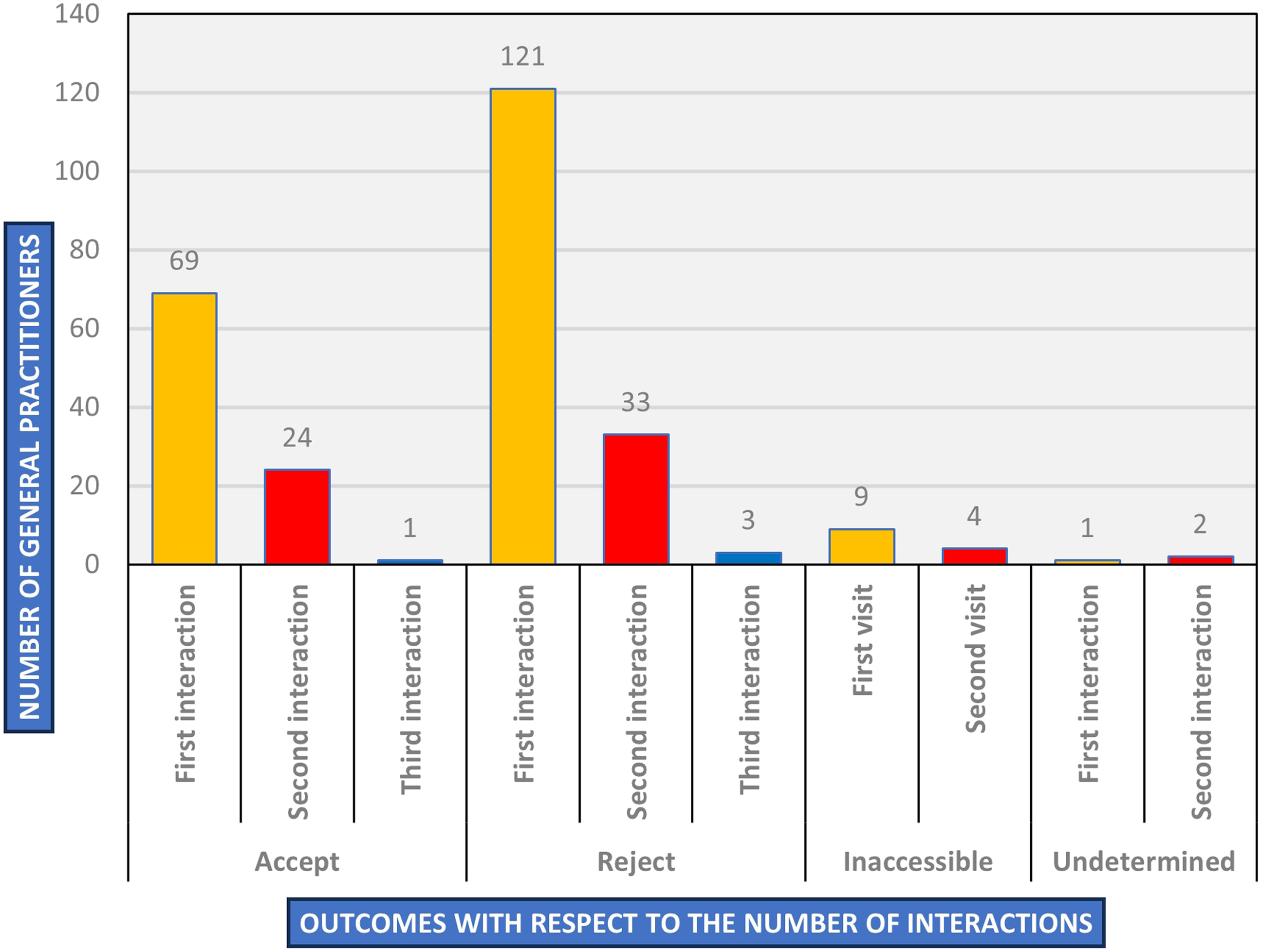
Of 30 GPs who participated in qualitative interviews, 24 were male and six were female. Based on SPSR assessment data, we categorised participating GPs into accepting or rejecting incentives, unable to work with new local pharmaceutical companies, committed to other pharmaceutical companies, not permitting SPSRs to enter clinics, and ignoring SPSRs. Figure 2 presents the main GP-SPSR outcomes, which we describe below. Flowchart of the outcomes of interactions between GPs and SPSRs.
Acceptance
Of those accepting the incentive, most GPs negotiated the magnitude of the incentive and the types of medications from the list they could prescribe in return. The majority sought to accept a certain percentage of money (as an incentive) proportional to the volume of medications they agreed to prescribe each month. Before I offered the GP incentives, he asked for a 35% commission from the sales of the medicines he prescribes. He also offered to connect me with his colleagues who can also support my products in return for some benefits, and this way I could have more support to sell the medicines. (SPSR-05)
In addition to money, a few GPs also asked SPSRs to organise dinners for their families. The doctor asked me to come back at 11 p.m. I went again and waited for him. The doctor did not meet me until he finished seeing all his patients. So, once he was alone, he called me in and heard about my proposal again, and then asked if I could organise a dinner for his family or some local travel. (SPSR-10)
A small number of GPs also asked SPSRs to help them with clinic-related issues such as providing them with equipment or other items for use in clinics. The doctor asked for a 1.5-ton split air conditioner and committed to prescribing all the products from the list for PKR 50,000 every month. (SPSR-14)
Some GPs accepted incentives from SPSR on certain conditions. For instance, they negotiated the commission that the SPSR offered, and upon increasing its percentage, the GPs agreed to make the deal. In response to my offer of 30%, the GP negotiated the commission, asking for 50% of the profit from the sales. He advised me to go back to the office, confirm the company policy on commission to doctors, and bring medicine samples for him to start prescribing the products. (SPSR-10)
A few GPs asked SPSRs to also allocate some money to pharmacists who managed GPs’ pharmaceutical commissions to finalise the deal.
Because many pharmaceutical franchises may not necessarily be legal entities, the availability of their products is often very limited. Therefore, some GPs asked the SPSRs to come back after ensuring that the products were available at the nearby pharmacies to finalise the deal. While the GP initially refused, after hearing the offer of incentives, he asked if we could help him with the renovation of his clinic. Upon my approval of the possibility, he asked to first supply the medicines to the nearby pharmacy, and if they have good efficacy, he can make the deal. (SPSR-09)
Interviewed GPs mentioned a range of reasons for engaging in pharmaceutical incentivisation, including financial constraints, increasing family needs, a desire to maximise income and resources, and pressure to meet socially desired standards of living. Many believed that a lack of training in professional ethics might be the reason behind accepting incentives from pharmaceutical companies and that such training could improve their medical practice. Workshops that also include pre/post-tests may be useful, rather than asking doctors to take formal exams, as they would increase their stress. Also, competitions with rewards may help. (GP-19)
The majority of the GPs saw lower-than-expected income as an important factor leading them to rely on pharmaceutical incentivisation and that higher wages could potentially reduce engaging in profit-led prescribing. The pay should be increased for the doctors. I think this will change things even if malpractice decreases by a very small percentage; the doctors are already underpaid. The [outpatient departments] are not going too well, and even in private practice, the doctors work more and are paid less. This makes the doctors frustrated. Junior doctors are not even given incentives as their practices are not going too well. (GP-01)
Weak regulation of the pharmaceutical sector was also mentioned, and how this and competition between companies might drive the practice of incentivising doctors. When many local companies were set up, it was the job of the government authorities to only allow the companies that manufacture quality products and only the products with the highest quality should come to the market. It is not the responsibility of the doctors to allow those companies to manufacture products. Substandard companies have been allowed by the government to manufacture and market their products. When the companies are willing to give the incentives and the doctors are willing to take the incentives, then how can you fix it? (GP-03)
Finally, PSRs’ job security tends to be contingent on the volume of sales, placing considerable pressure on PSRs to use incentivisation as a major tool to get GPs’ support for their products. There shouldn’t be any targets given to the medical reps. They should be told to communicate information about their products to the doctors and then the doctors would prescribe the drugs as per the patient’s indications. Now, the rep says that his job is at stake, and he is helpless, the doctor is not willing to take incentives. (GP-06)
Rejection
Many GPs who rejected incentives also advised SPSRs to not attempt to make such offers again.
Indeed, of these, some shunned SPSRs and asked them to never come back to their clinics. The female doctor became very angry with me when she learned that I was representing a pharmaceutical franchise. She quite straightforwardly refused to prescribe my products and all the incentives and offers I made to her. (SPSR-15)
A small number of GPs agreed to prescribe SPSRs’ products to support them in their jobs, but they rejected taking incentives in return. The doctor asked me not to talk about incentives, but he could prescribe my products to support my job if I continue to visit in a professional way. (SPSR-12)
Interviewed GPs frequently mentioned ethical practice as the main reason for not engaging in pharmaceutical incentivisation in exchange for prescription. If the conscience is awake, and doctor is focused on earning lawfully, then there is no doubt that the doctor will draw a line between what is lawful and what is not. If the conscience is not there, then none of it will happen. (GP-23)
Some participants recommended that doctors should prioritise patients’ interests and prescribe quality medications, which they believed could usually be obtained from companies with a good reputation in the pharmaceutical market. Participants also said that doctors should not meet with PSRs from substandard companies: We should always consider the standard of the product. Sometimes even newer companies also have excellent products. These companies do try to tempt us, no doubt about that; they corrupt the doctors. Those with the strongest faiths are unaffected by these offers. (GP-19)
Undetermined
There were a number of cases where it was not possibly to clearly identify acceptance or rejection. For instance, while some GPs took interest in SPSRs’ incentivisation offers, they said they were ‘packed’ or ‘saturated’ and were unable to accept them. The doctor did not respond with clarity. He said I should talk to the nearby pharmacist and provide him with all the details. I then approached the pharmacist who said that the doctor was quite packed now and that I should keep visiting, so the pharmacist could let me know if the doctor could make any space in the future. (SPSR-09)
In interviews, GPs explained the meaning of being ‘packed’ or ‘saturated’ in response to pharmaceutical incentivisation offers as indicative of GPs’ commitments to other companies but that these GPs might be able to take offers in the future: This is because these doctors are so involved with four to five companies, they have made commitments with. So, the doctors say that they have targets to meet and can’t take commitments anymore. Therefore, they say no. (GP-18)
Many SPSRs indicated hearing from GPs that they were not interested in prescribing the products of pharmaceutical franchises and that they were therefore not interested in their incentives because of concerns about product quality. The doctor believes that franchise-based medicines are not of good quality because they are manufactured and packed in local streets. I assured him that our products have good efficacy but after looking at the product flyer, the doctor said it does not contain a stamp by a legal manufacturer, so he cannot trust the products. (SPSR-15)
One GP also expressed concern about the increased cost of the franchise-based medications, in addition to the doubtful efficacy of the medications. They sell their products at a very high cost even when their efficacy is doubtful. I have heard that franchises generally get their products from Lalu Khet [a local market where illegal pharmaceutical products are manufactured/packed/sold], package them, and bring those products to the market. They get the flyers made. The medical reps they have are also juniors who don’t even know anything about medicine. Sometimes their hands are even shaking while they talk to us and seek support on sales. (GP-28)
However, while GPs might reject franchise-based medications, this does not necessarily mean that they rejected accepting incentives altogether; indeed, GPs might engage with certified companies that usually also offer incentives to ensure their and patients’ safety as well as to get incentives. There were also cases where GPs did not engage with incentivisation offers beyond asking a few general questions (He just asked one question about the background of the company and distribution network and then just ignored who I was and what I was talking about. I felt that the doctor did not interact with me with interest (SPSR-10)) and indicating general lack of interest in the product. I think it is undecided whether the doctor is interested in making a deal with us because there was no clarity in his response to my offers. He did not show interest in my products and incentives, but at the same time, he did not refuse to take them. During my detailing of the products, he just said “Okay stop, do not try to teach me about what medications work for what”. (SPSR-05)
In the interviews, many GPs were not able to make sense of why some GPs ignored PSRs. However, they believed that doing so was an inappropriate way to deal with PSRs because it is their professional responsibility to explain their products to physicians. This is not right. If someone is telling you about their product, then you should at least hear them out, maybe it is a good product. You can choose not to take benefits but maybe the product is good. I don’t know; maybe that is some policy of their own. Or maybe they are just trying to give the impression that they are important and want the reps to come 2 or 4 times then they would meet the reps. (GP-02)
Inaccessibility of GPs
As noted above, a small number of GPs did not meet PSRs, with clinic attendants who usually manage these meetings asked SPSRs to leave the clinics. The attendant said the doctor does not meet with pharmaceutical representatives, no matter how long you wait for him; be it 1 hour or 10 hours. (SPSR-11)
Interviews indicated that many GPs believed that physicians who experience a heavy load of patients could generate good income and for this reason, they might not be interested in meeting PSRs and discussing incentives. Sometimes I have observed that patient flow is high, and the reps keep coming one after the other. The doctor earns enough at the [clinic] that he/she doesn’t need medical reps. This is the actual thing. Patient flow and time do play a role because the reps don’t come for two minutes and place their product, they describe the literature instead. (GP-02)
Discussion
This study explored outcomes resulting from pharmaceutical incentivisation offers to GPs in Pakistan. Existing research typically analyses the profit-oriented mindset of the pharmaceutical industry, budgets allocated to pharmaceutical marketing, the role of PSRs in promoting pharmaceutical products, and the likelihood of the distortion of doctors’ prescribing behaviours resulting from pharmaceutical incentivisation.23–25 Our study took a micro-level approach, providing important new insights into the complex interactions between GPs and PSRs and enabling distinguishing between four possible outcomes from those interactions.
We found that the interactions between GPs and PSRs may not always be straightforward. For example, the rejection of incentivisation offers by GPs may be indicative of their ethical practice but we found that they tended to engage with pharmaceutical companies nonetheless, which puts their ethical behaviour into question. The SPSR method used in this study helped unravel these subtleties and explain the complexity underlying GP-PSR interactions, which can be seen to be driven by profit-maximisation motives. The SPSR method could thus provide a useful tool for regulatory bodies to monitor and regulate the primary care sector in Pakistan.
Consistent with other studies, we found that GPs were prepared to change their prescribing behaviour in response to pharmaceutical incentives and this might not be in patients’ best interests.26–28 GPs had the tendency to prescribe medications unnecessarily and for personal gains. Further, prescribing for profit might increase the financial burden on patients.
Our data also provides important insight into specific situations and jargon used by GPs and PSRs to in relation to pharmaceutical incentives. For instance, we observed instances where GPs said they were ‘saturated’ or ‘packed’, implying their refusal to engage with SPSRs at that particular point in time while indicating openness to accepting incentives once they had met the targets of other pharmaceutical companies. Further, GPs rejecting incentivisation offers from unknown local companies suggests that these GPs might have accepted incentives from well-established companies.
The pressure to maximise sales on which PSRs’ jobs are contingent drives the use of aggressive marketing techniques, 25 including overt discussion of incentives and asking physicians to justify prescribing from other pharmaceutical companies. Some GPs in our study agreed to prescribe their products but rejected accepting incentives. While this practice may be seen to be encouraging as such, it has implications for patients’ health, in particular where GPs were accepting products from unknown companies and lacked concern about the quality of related medications.
Our study has several important implications for research in low- and middle-income countries. It enhances our understanding of how pharmaceutical companies and GPs (and physicians more broadly) bypass existing guidelines, laws, and policies restricting the provision of incentives from pharmaceutical companies to medical doctors. Replicating the SPSR method in countries such as India, Bangladesh, and others in East Asia and the Eastern Mediterranean will provide further insights into the magnitude of incentive-linked prescribing as well as strengthen the SPSR method. Further research is needed to help test the validity and reliability of the SPSR method, and so strengthen the case for its use in health care regulation. The method might also help determine the extent to which antibiotic prescribing is associated to pharmaceutical incentivisation and so inform antimicrobial stewardship programmes. It could further be used to better understand the relationship between pharmaceutical companies and pharmacists in countries where over-the-counter medication is common.
This study captured real-life scenarios of GP-PSRs interactions around incentivisation offers. The PSRS method helped demonstrate that there are GPs who adhere to ethical medical practice even in the context of weak health system regulation as is the case in Pakistan. We identified a small number of GPs who not only verbally rejected incentivisation offers but also expressed their dislike and anger against such offers. Regulators, health system advocates, and ethicists should build partnerships with these GPs in the promotion of ethical medical practice. In addition to continued education on ethical prescribing, government-based financial incentives for good medical practice could discourage GPs from accepting incentives from pharmaceutical companies. Elsewhere, pay-for-performance schemes have shown promise in terms of improving the quality of care,29,30 but for this to work will require better monitoring. As noted, the SPSR method could be a potential monitoring tool for regulatory institutions like the Pakistan Medical Commission and various provincial health care commissions. We suggest that the GP-PSR interaction outcomes presented in this study can be useful concepts to increase students’ awareness of ethical dilemmas arising from pharmaceutical incentivisation if incorporated into medical schools’ curricula.
Study limitations
Our SPSRs represented new local pharmaceutical companies and it is possible that GPs who refused to accept incentives and ignored SPSRs might not have been comfortable talking about incentives with unknown companies. Similarly, to safeguard SPSRs, we restricted GP visits to a maximum of 3–4; this restriction might have limited their ability to build informal ties with GPs and which might have brought additional insights. Moreover, our study was based in the Karachi region of Pakistan. Given the sociocultural diversity, a multisite study would have likely provided additional insights into how GPs react to pharmaceutical incentivisation offers. Finally, we only focused on GPs, and we believe that the use of the SPSR method would enrich our understanding of patterns in accepting pharmaceutical incentives among private consultants and other doctors working in private hospitals.
Conclusion
This study provides a detailed analysis of the incentive-driven interactions between GPs and PSRs in Pakistan. Pharmaceutical deals are typically made in confidence. In countries where health governance is weak and electronic prescribing is a challenge, the SPSR method can be of great value to monitor doctors’ engagement in unethical, profit-led prescribing. The doctor–PSR interaction is not straightforward as offers to engage in prescribing for mutual financial benefit are not taken up immediately, and doctors are cross-pressured by ethical training. Better understanding of this interaction using the SPSR method can provide valuable insights for policymaking.
Supplemental Material
Supplemental Material - What happens when private general practitioners receive incentivisation offers from pharmaceutical sales representatives? A qualitative study in Pakistan
Supplemental Material for What happens when private general practitioners receive incentivisation offers from pharmaceutical sales representatives? A qualitative study in Pakistan by Muhammad Naveed Noor, Afifah Rahman-Shepherd, Sabeen Sharif Khan, Rumina Hasan, Amna Rehana Siddiqui, Iqbal Azam, Faiza Bhutto, Afshan Khurshid Isani, Sameen Siddiqi, Robyna Irshad Khan, Sadia Shakoor and Mishal Khan in Journal of Health Services Research & Policy.
Footnotes
Acknowledgements
We acknowledge support from Dr Natasha Ali (Associate Dean at AKU), the PMC, the SHCC and the Centre for Biomedical Culture and Ethics (CBEC). The research project is executed by the Department of Pathology and Laboratory Medicine, at AKU. We are thankful to the administrative staff of the microscopy laboratory based in the Department of Pathology and Laboratory Medicine for their support of the project. We are also thankful to the GPs who participated in our study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the UK Research and Innovation (UKRI) under grant number MR/T02349X/1. This work was supported by REDACTED.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.