
Abstract
Objectives
With high disease and disability burden in rural and remote regions, student-assisted clinics can be an effective workforce development tool to meet community health needs and workforce shortages. This research sought to identify the conditions under which student-assisted clinics can be successfully utilised as a workforce development strategy, with specific application to remote Queensland, Australia.
Methods
A rapid review of the international literature in English was conducted. This was the most appropriate type of review because the results of the review were time-sensitive, with the student-assisted clinic model being trialled in Queensland soon. A mixed methods design was applied, with the search strategy piloted with one database.
Results
Eleven studies met the inclusion criteria. Seven reported data on participant experiences, including consumers, students, services/clinics, and educators/supervisors/health professionals. Each of the studies operationalised student-assisted clinics through practice models (university-driven learning need), service delivery models (service driven need addressed through a student workforce), community need models (student delivered services primarily addressing a community health need), and blended models (practice need and community need). Some studies reported concerns about fragmentation of services, referral pathways and issues with follow-up, while others reported concerns about sustainable funding. All models reported successful outcomes when focused on service or consumer health outcomes, or student learning outcomes.
Conclusions
Student-assisted clinics make an important contribution to the development of the rural and remote health workforce. Student-assisted clinics can complement and extend existing services, supporting workforce development in an overstretched health system impacted by an ongoing pandemic.
Introduction
Local health service delivery brings challenges in rural and remote locations related to cost and distance, particularly with access to profession and scope specific expertise.1–3 These challenges can be very costly to hospital and health services in rural and remote locations, where the financial burden for accessing out-of-region services can often fall on the budget of the local public health services.1,4 Building expertise in the local health workforce can have significant benefits to the local health budget, and to the community, by reducing the need for travel and increasing local access to services.5,6
One country facing these challenges is Australia. Due to the lasting effects of colonisation, many of the Indigenous people of Australia – the Aboriginal and Torres Strait Islander peoples – live in the remotest and/or most disadvantaged parts of the country. Gulf Country, a very remote part of the state of Queensland, has a land mass of 186,000 square kilometres. 7 The population is 52,481, with the largest population centred in a large remote mining town, from where the primary health services are delivered. 8 Almost 40% of the population are the Aboriginal and Torres Strait Islander peoples (compared to an overall Queensland percentage of 4.6%). There is a high burden of chronic disease and disability for all Queenslanders (51.7%), with the rates 1.4 times higher in remote and very remote areas. This is because of lifestyle and medical conditions that could be reduced or avoided with earlier access to health services. 9 Additionally, the available local workforce (to address these health needs) is limited, with only 9.6% of individuals in the Gulf Country holding a university level qualification (compared to the state average of 21.9%), and only 24.7% holding a vocational qualification (compared to a state average of 28.3%). 8
The high disease and disability burden, and lower education rates, creates a challenging landscape in which to build a local response to critical health service needs. The COVID-19 pandemic has placed further strain on an already stressed health system.8,9 Further, access to psychologists and other health professionals who have expertise in complex health presentations is even more challenging, with professions and services often being metro-centric in education, training and career pathways. 10 For example, a key identified service gap in the local region was psychology paediatric assessment services, with the majority of assessment services only available in regional or metropolitan centres because of psychology workforce distribution problems. 10 The number of psychologists practicing in rural and remote Australia was estimated to be less than 8% of the psychology workforce. 10
A key strategy to addressing this type of service gap/workforce issue is student-assisted clinics, where health clinics or services are designed to be run or supported by students.11–14
Student-assisted clinics
The terms used for student-assisted clinics have included ‘student-led’, ‘student-assisted’ and ‘student-run’, with little consensus on how these terms are defined.
15
A concept analysis completed by Nagel et al.
15
investigated the use of terms across 222 articles, proposing common definitions for the different terms to help guide research and practice. Although Nagel et al. identified three main conceptual definitions that factored in the specific characteristics and intent of the clinics, the definitions were centred around academic institutions and not service needs.
15
For this reason, the current research has adopted the term student-assisted, with a similar definition to student infused initiatives: Student-infused health initiatives – projects or programs that are initiated by academic institutions as part of the formal curriculum and mainly operated or delivered by students to provide a health-related service(s) to community members. In this model, development and implementation of the project or program is designed with intention to promote acquisition of entry-to-practice competencies through experiential learning, service learning, or other planned activities as either a required or optional for-credit pre-licensure education strategy.
15
(p14)
In the context of the current research, it is proposed that the term student-assisted refers to clinics, projects and/or programs that are developed to address a community health, service or student learning need, and contribute to workforce development.
Student-assisted clinics have been identified as improving outcomes for patients11,12 and improving student skills and confidence.13–15 However, the popularity of student-assisted clinics, and the workforce advantages associated with increased clinical expertise through supervision of students, needs to be tempered with a considered approach. The disadvantages associated with student-assisted clinics has included issues such as time and planning (to ensure client outcomes and student experiences are safe-guarded), who has professional oversight, and who is responsible for continuity of care after the clinic has ended.14,15 These disadvantages highlight the need to purpose build a student-assisted clinic that can meet the needs of the community longer-term and not just for the time the clinic runs.
Research aims
The aim of this scoping review was to understand the conditions under which student-assisted clinics can be successfully utilised as a workforce strategy in the context of health services, with a focus on assessment and intervention. This review aimed to answer the following research questions: 1. What are the outcomes of student-assisted health assessment and/or brief intervention clinics in rural areas? 2. What are the experiences of student-assisted health assessment and/or brief intervention clinics in rural areas? 3. What operational models have been used to develop student-assisted health assessment and/or brief intervention clinics in rural areas?
A rapid review was the most appropriate type of review for this research question, as the results of the review were time-sensitive because planning was underway for a student-assisted clinic in a remote town in Gulf County, Queensland, Australia. A rapid review is most appropriate when the review is being used to inform practice, enabling the examination of the extent, range and nature of research activity in this topic area. 16 The final question will help narrow down the models that would be able to be utilised within the Queensland remote health service context.
Methods
To answer the review questions, a mixed methods rapid evidence review methodology was applied. A rapid search of the literature was conducted between 4 April 2021 and 30 June 2021 by three authors (DC, MH and GW), with a final search of the scientific literature completed in July 2022 by one author (DC) to ensure completeness. Data was extracted using a convergent integrated approach, adhering to the Joanna Briggs Institute (JBI) methodology for mixed methods systematic reviews (MMSR).17,18 A convergent integrative approach simultaneously synthesises quantitative and qualitative data to answer the research questions. 18 The protocol for this review was registered with the international prospective register of systematic reviews (PROSPERO). 19
Inclusion and exclusion criteria
Studies were included if they included human patients, a geographically rural and remote population, student-assisted health clinics and were addressing a gap in current services. Studies were excluded if they were not published in English, if they were focused only on student learning rather than meeting the health needs of a community and if they were a large regional or metropolitan sample.
Search strategy
The systematic review search strategy was piloted in April 2021 on CINAHL, with minor adjustments made to key word order and parameters to ensure all relevant articles were found (see S1 of the online supplement). The full search included the following databases: MEDLINE, Scopus, ProQuest Health and Medicine, Informit Health Database Collection, CINAHL, PsycINFO, Cochrane Library and Web of Science. The search strategy included key search terms related to the intervention (i.e. student-assisted clinics) and the exposure (assessment and intervention).
Study selection and critical appraisal
All identified citations were collated and uploaded into Covidence (a systematic review management system), and duplicates removed. Titles and abstracts were screened against the inclusion and exclusion criteria by two authors, with a third author resolving disagreements at each stage of the process. For thoroughness, manual checks were also completed using Google Scholar. Potentially relevant studies were retrieved in full and critically appraised for methodological quality. Reasons for exclusion of full text studies were recorded. The full text of selected citations was critically appraised using the Mixed Methods Appraisal Tool version 2018 (MMAT v2018).20,21
Data extraction and synthesis
The data from the included studies were extracted by two independent reviewers using the standardised Joanna Briggs Institute System for the Unified Management, Assessment and Review of Information (JBI SUMARI) data extraction tool. 22 The data extracted for each study included region, context, population, research methodology, results and outcomes. Following extraction, data from the included studies were synthesised using a convergent integrated approach by one author (SV), with two authors (LS and PS) separating the data into key themes, using the research questions as a guide. 18 Any disagreements were resolved through discussion.
Results
Search outcomes
The initial search identified 70 studies, with three additional studies found through a grey literature search. After duplicates were removed (n = 6), a title and abstract screening was completed against the inclusion and exclusion criteria. The full text of the remaining 31 studies was assessed by three reviewers (DC, MH and GW) for inclusion, with 10 papers meeting the inclusion criteria. Agreement was reached through discussion. A final paper was included after review, bringing the total to 11 papers. A summary of the search results is presented using the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram (Figure 1).
23
A final search was conducted in June 2022 with no new results generated. PRISMA flow diagram:
23
results for rapid review.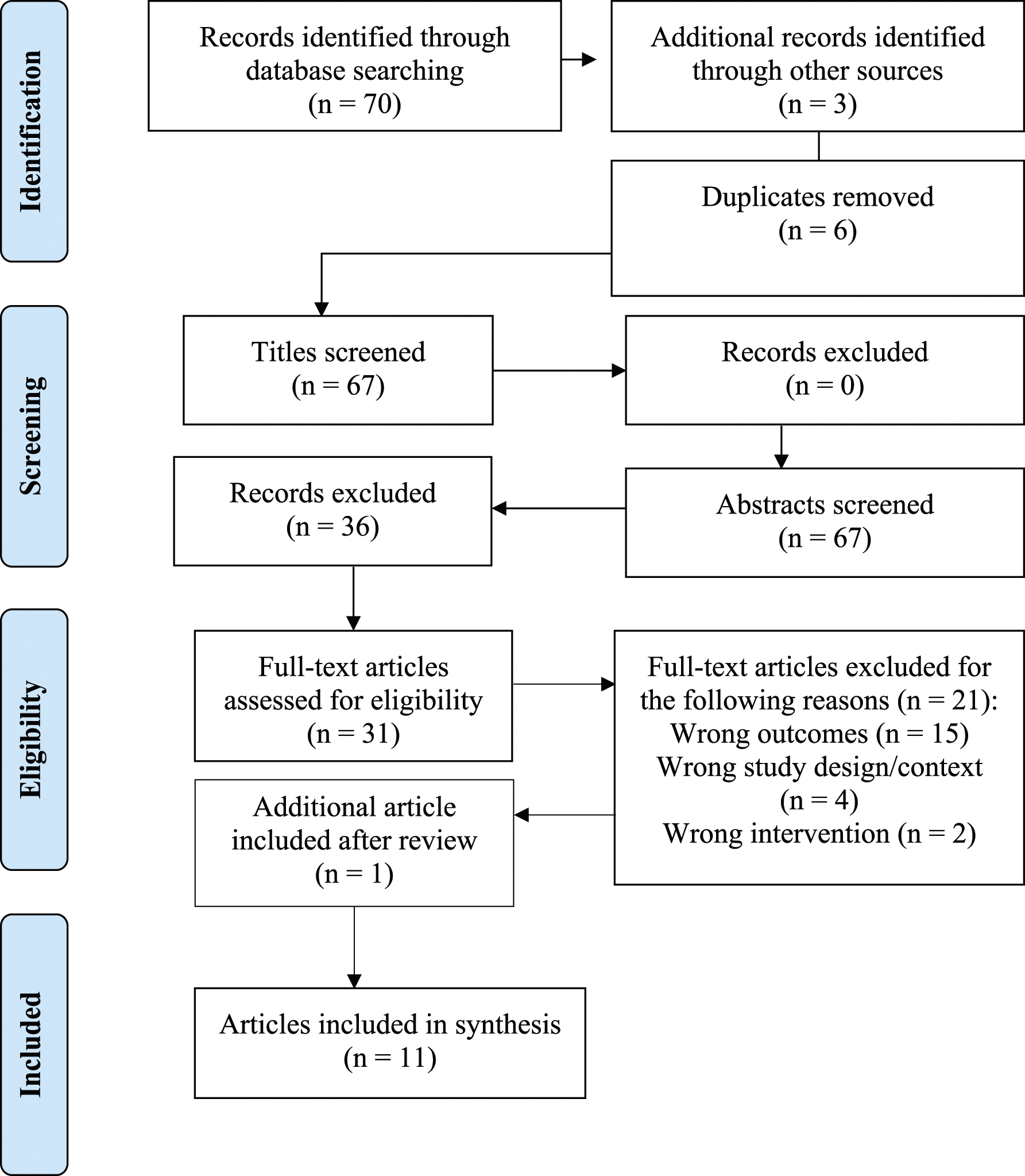
Critical appraisal
All studies passed the quality screening process. An overall confidence in results score has not been provided because current evidence indicates it is misleading to provide an overall score (for mixed methods reviews) rather than a detailed presentation of the criteria.21,22

Notes. Research designs of included studies are mixed methods (MM), qualitative (QUAL) and quantitative (QUAN).
Quality criteria is assessed as: Y: criteria met; N: criteria not met; ?: not reported in study; N/A: not applicable.
Characteristics of the studies
The included studies were mixed methods (three studies),24,25,29,30 qualitative (two studies)25,34 and quantitative (six studies).26–28,31–33 Six studies were conducted in rural Australia (New South Wales, Queensland, Western Australia),24–27,30,34 three in rural United States (Iowa, Colorado and Eastern Northern Carolina),31–33 one in rural United Kingdom (England) 29 and one in rural Ecuador. 28 Seven studies only included students from one health discipline (medicine, pharmacy and nursing),24,26,28,29,31,32,34 one study including two health disciplines 27 and three studies including more than three health disciplines.25,30,33 Nursing was represented in nine of the elected studies.24–28,30,31,33,34 Medicine was represented in five studies (only four included students),24,25,29,30,33 pharmacy in four studies24,25,32,33 and other allied health disciplines in four studies.24,27,30,33 Psychology was not represented in any of the included studies. A full summary of the characteristics of each study – including the aims, participants, methods, results, and limitations – is presented in S2 of the online supplement.
Synthesis of results
Results have been synthesised under the broader themes the review questions focused upon.
Reported outcomes of student-assisted clinics in rural areas
When applying a service-learning model to a student-assisted clinic, Stuhlmiller and Tolchard 26 measured outcomes using occasions of care/service and client numbers. Students in rural New South Wales, Australia, were reported to have delivered over 1000 occasions of care within the drop-in health clinic and had reached 1500 people through health promotion initiatives. 26 Student placement hours were reported as averaging between 80 and 120 h per student, with some students volunteering more time. 26 Frakes et al. 24 also measured outcomes using occasions of care/service as a success measure for their interprofessional student-assisted collaborative placement model. Staff were reported to have supported 78 students to deliver 4565 occasions of care/service to 460 new patients, which was estimated to be a 124% increase over the reporting period. 24 Increases in services provided were recorded over the two reporting periods included in the study, with an increase in new clients (11%) and an increase in student placements (52%) also reported. 24 The results from the Frakes et al. 24 study should be considered with caution because of the quality issues identified in Table 1 (see critical appraisal).
Grace and Coutts 30 reported outcomes by the type of health issues/conditions identified by the students during the pop-up interprofessional student-assisted clinic in rural New South Wales, Australia, although the number of presentations were not provided. Students completed discipline-specific assessments, with medical practitioners (GPs) reviewing each participants’ results and referring to local services as required. 30 The details of the referrals were not provided. Palma et al. 33 found that when delivering tailored student-assisted mobile clinics, gaps in health service access and availability could be met, with success measured through return visits (54% of patients who use the service more than once) and patient satisfaction (98% rated service as good-excellent). Bartlett et al., 29 in their study on rural immersion hubs for medical students in a rural district of England, reported patient attitudes as an outcome, with success being reported as patients’ willingness to see students (97%).
Similarly, Larsen et al. 31 reported success by two measures, the number of health assessments completed and the number of appropriate and timely referrals made by nursing students to other services in the region. 31 Health assessments assisted in early identification of students who required psychosocial and biomedical support. A 20% increase was reported in the number of health assessments completed during the reporting period; however, the completion rate of referrals to other services differed significantly across school clinic sites because of timing and available services. 31
Stuhlmiller and Tolchard 27 reported on outcomes from a student-assisted free drop-in health service in rural New South Wales, Australia. The clinic was established using a community service consultation approach, addressing a community and student placement need. 27 The study reported improved outcomes using demographic, lifestyle and chronic condition data; however, the analysis was a population-level analysis rather than an individual change analysis. 27 The researchers also reported success through healthy lifestyle programs that were developed through this clinic, such as student-assisted soup kitchen and the healthy eating program for school-aged children. 27 Improvements in identified health conditions were reported by other researchers, indicating student-assisted clinics can lead to health improvements for clients. 32
Relatedly, advanced pharmacy students in rural Colorado delivered a student-assisted diabetes clinic program, focused on diabetes management and care over a 6-month period. 32 Nuffer et al. 32 reported successful outcomes based on measurable changes in diabetes point-of-care measurements, with all measurements reported as improving except for HDL-cholesterol values. 32 For a rural family nursing student-assisted home service in rural Ecuador, success was measured using quality of life outcome measures, with the student-assisted service resulting in significant improvements in aspects of physical health and function when compared to the control group. 28 However, sample loss bias needs to be considered when interpreting these outcomes. 28
Craig et al. 25 found that by using a project model and placing interdisciplinary teams on social capital projects that would benefit the community/health services they were targeting (seven rural towns in New South Wales), they could create solutions to clinical problems without directly having students work with clients. 25 The project was reported as a success, with nine of the 21 projects reported as being still in use at follow-up. 25 Thackrah et al. 34 used a project model to target culturally safe practices by students through cultural immersion in a student-assisted health promotion clinic in a remote Western Australian Aboriginal community. 25 Outcomes were reported through engagement with the student service and reflective learning outcomes reported by the students and Aboriginal Health Workers. 34 Client data was not reported. 34
Reported experiences of student-assisted clinics in rural areas
Seven studies reported data on participant experiences, including consumers,29,33 students,24,29,30,32,34 services/clinics25,29 and educators/supervisors/health professionals.25,29,30,34 Four studies only reported outcome data and did not report the experiences of the study participants.26–28,31 One study did report case study data, following the care outcomes of particular consumers; however, the consumers and the students did not provide direct feedback to the researchers about their experiences with the health clinic. 26 The following results are based on the studies that collected experience data from at least one source.24,25,29,30,32–34
Consumer experiences were reported in two studies using questionnaires that included Likert scale questions29,33 and free text questions. 29 In their free text responses, consumers reported that they valued the presence of students overall, believing they were provided with more time and learned more about their condition when a student was involved. 29 In two studies, consumers reported high satisfaction with the student service, with many reporting good outcomes based on either the student proving the medical care they needed or the extra attention they received from a qualified medical practitioner.29,33 A small number of consumers reported concerns about confidentiality and not having a choice about students’ involvement in their care. 29
Five studies reported student experiences,24,29,30,32,34 with one study identifying that approximately half of the students conveyed an increased willingness to pursue a rural career.
32
Positive experiences centred around professional and personal development, and teaching and learning.24,30,32,34 One study discussed students mixed experiences in rural and remote placements, with travel and isolation the common issues reported, and internet access security and lack of recreation opportunities also listed as deterrents.
29
Another study reported that trust, communication, and culturally appropriate health messages were reported by students as being important for the success of student-assisted clinics, allowing the service to draw on the knowledge and strengths of the culture and community.
34
These experiences highlighted the importance of student-assisted clinics being purpose built for the community/health needs. One student shared her own learning: I learned how presumptuous and abrupt I can be…it is easy is slip back into that and then people ignore you. I had to concentrate on being respectful.
34
(p329)
Three studies reported that interprofessional learning was highly valued by students,24,25,30 although in one study this was reported by informants (supervisors/staff/services) and not students. 25
Some students felt they first needed to be immersed in their own profession, so they had a better understanding of what their role is in an interprofessional team. 30 Stuhlmiller and Tolchard 26 also reported the benefits of students learning through the collaborative learning model; however, these benefits were reported by the researchers and not the students.
Four studies reported the experiences of educators/supervisors/health professionals,25,29,30,34 and two studies reported the experiences of services/clinics.25,29 In one study, clinical educators noted that student involvement added value to their practice and kept their knowledge and skills up to date: I have to polish my skills up definitely … because I know I’m having a student I feel motivated to read up a little bit more and brush up my skills … it definitely improves my consulting.
29
(p5)
While in another study health professionals reported the benefit of students and interprofessional care to consumer outcomes: To improve safety in [consumer] care, greater emphasis needs to be placed on the findings of the other professions and their concerns communicated better to each other (osteopathy supervisor 2).
30
(p117)
One study reported the importance of health professionals in encouraging consumer attendance and supporting students to disseminate health information within the community using culturally safe practices.
34
Other studies reported that services and health professionals found student involvement helpful, improving services, communication or awareness of health or service issues.25,29 One clinic reported: It’s added to our practice and it’s added to our enjoyment and its made us happy to come to work … and I think that’s definitely something the staff feel, you know, students literally breathe a breath of fresh air into the practice.
29
(p5)
Operational models utilised to deliver student-assisted clinics
Student-assisted clinics: operational models utilised in included studies.

The student-assisted programs that utilised service delivery models were argued to be successful because they were improving service provision, 25 or meeting the demands in service which the current workforce could not meet alone.24,31 Service delivery models24,25,31 seemed to be the more vulnerable to current resources and management support when compared to practice models28,29,32 that were led by university learning programs. However, students’ willingness to participate in rural and remote placement programs appeared to be dependent on perceived inclusion (in the main university program) and practical supports (accommodation and financial). 29
Sustainability of operational models
Many of the student-assisted operational models were utilising pre-existing health services or were embedded within university services or programs to safeguard their sustainability,24,26,27,29,31,33 while others did not address the sustainability of the model after the initial program was delivered.25,28,30,32,34 Frakes et al. 24 reported that although they received funding to develop and implement an interprofessional student-assisted clinic, access to ongoing funding would always place the sustainability of student-assisted clinics at risk. Palmer et al. 33 identified the need to support student-assisted clinics within university programs, including the provision of clinical education and administrative resources.
Challenges and constraints of student-assisted clinics
Frakes et al.
24
relied on stakeholder involvement to deliver the clinic, also making it vulnerable to stakeholder staffing changes that may not prioritise the initiative. Additionally, differences in curriculum, and placement timing and length, placed pressure on resources when initially setting up the student-assisted clinic.
24
Grace and Coutts
30
highlighted the high level of organisation required to make a clinic successful, with communication across professions and shared intake processes being a priority. In another study students reported that the way in which universities deliver their curriculum does not always support rural and remote placements, with some feeling a sense of injustice: I still feel like we’re getting the bad end of the deal being in Ludlow, I don’t think there are benefits to being put here as opposed to Shrewsbury. I think we miss out on a lot; like facilities and library and having more people around, there is a much bigger student population in Shrewsbury and lots more to do.
29
(p.8)
It was also reported that there were limitations in the number of professionals available to see clients (when a referral is made), impeding outcomes for clients.25,30 Two studies identified that there was a danger that student-assisted clinics can cause fragmented health care because of referral follow-up and barriers around access to other services (e.g. financial or distance).30,33
Evaluation was identified as a challenge, with some studies only using clinical records or routine feedback,24,26,31 while one study may have been affected by recall bias because of the extended time the study covered. 25 Some studies focused on occasions of service or service data outcomes as a measure of success rather than consumer and/or student experiences.26,28,31 Studies that did focus on participant experiences did not always include all viewpoints, biasing the outcomes to a narrower perspective than otherwise would have been received.24,25,30,33,34
None of the included studies included measures that reviewed the operational student-assisted clinic model, with only a few studies reporting on the likelihood that the student-assisted clinic would result in students choosing a rural health career.24,29,32 Record keeping and consistent point-of-care results being recorded were identified as limitations of drop-in student-assisted clinics, identifying the need to include training in processes and procedures in student-assisted clinics, and regularly checking client data for completeness.26,27,33 Some studies did not report response data for all participants and/or completeness of data.26,27,30,33,34 Studies that did include response data identified sample size as a concern, 28 as well as participation rates,28,29 lost to follow-up 28 and incomplete data.27–29,31,33 It is recognised that with many research projects of this nature there is limited funding available to conduct more robust research; however, these identified issues limit the generalisability of outcomes across nations and communities.
Discussion
This review aimed to answer three key questions to inform the development of a student-assisted clinic in a remote community in Queensland, Australia: what the outcomes of student-assisted clinics in rural areas are, what the participant experiences of student assisted clinics in rural areas are, and what operational models have been utilised to deliver student-assisted clinics in rural areas. Eleven papers met the inclusion criteria for this review, with clinics being delivered within rural and remote communities in the United Kingdom, Australia, the US and Ecuador. There were differences in the terminology and definitions used, with student-led, student-run, student-assisted and service-learning being the most common.24–34 Having a comprehensive definition of a student-assisted clinic was seen as important, with the current research adopting the term ‘student-assisted’, adapting a definition from Nagal et al., 15 (p14) student-assisted clinics were defined as programs/services/clinics that are developed from a community health, service or student learning need and contribute to workforce development.
Similar to previous research,11–15 all studies reported positive outcomes for consumers, services and/or students24–34; however, there were inconsistencies in how outcomes were reported across studies. Some studies focused primarily on student outcomes, while others focused on consumer or service outcomes.24–34 Only one of the studies addressed the longer-term implications for student-assisted clinics, identifying the unintended consequence of fractured service provision, 33 a concern that has been identified in other research.14,15 This concern also extended to clinics that were designed to meet a community health need but did not have links or access to local services, 30 highlighting concerns around referral pathways (limited) and continuity of care (including follow-up) that has been discussed in other research.14,15 There also seemed to be limited community involvement in the development of student-assisted clinics, with health needs being more commonly identified by community services or university programs.24,26–28,30–32 These concerns highlight the need for student-assisted clinics to have community input at a grass-roots level, and be led by a key community service, or to have clear referral linkages to key community services, so that when the student-assisted clinic is completed consumers know what services they can access and who their primary service is.14,15,24,25,30,33
Furthermore, although many studies identified workforce issues or community health needs as a driver for clinic development, outcomes were measured as occasions of service and consumer health improvements, rather than broader community improvements (such as decrease in unmet health needs or increased access to services) or workforce development.26–28,30,31,33 The inconsistency in how outcomes were measured has been found in other reviews, demonstrating the need for agreement on how to measure the success of student-assisted clinics. 15 Certainly, at a minimum, outcomes should focus on consumer, community and student learning outcomes, allowing researchers to identify if the student-assisted clinic is contributing in positive ways to workforce development or creating a fragmentation in health care.15,35
There were many challenges and constraints identified for student-assisted clinics, with funding, staffing and leadership commonly identified influencing the long-term sustainability of a student-assisted clinic.24,25 The quality of the evaluations across studies raised concerns about confidence in results, with occasions of service or health outcomes for consumers being a common measure of success,24,26,31,32 again demonstrating the need to broaden outcomes to include workforce and community benefits.14,15 Clinics were considered to be more sustainable if they were embedded within the funding or an existing service, or if they were led or supported by a university program.24,26,27,29,31,33
Studies that focused on participant experiences were able to highlight important qualities of a student-assisted clinic; however, most studies were limited in the experience data they collected,24,25,30,32–34 with only one study including data from all participant sources. 29 Student feedback commonly centred around their scope of practice and personal learning experiences (including isolation and financial constraints),24,29,30,32,34 while service/health professional feedback commonly focused on communication, mutual learning and consumer benefits.25,29,30,34 Consumer experience data was positive but it was also very limited,29,33 highlighting the need to include consumers in research focus groups and interviews to better understand their experiences.
The final review question attempted to identify the operational models that were being utilised to deliver student-assisted clinics. Three main operational modes were identified (practice model,28,29,32 service delivery model24,25,31 and community-need model33,34), with two studies utilising a blended model (combined practice model and community-need model).26,27,30 Practice models appeared to be more sustainable overall, because clinical education and student learning were funded within the university program, and rural clinics always needed the extra workforce that students provided.28,29,32 The blended model, utilising the benefits of the practice model and addressing a community health need, appeared to be the most benefit to the community, although ongoing funding for the community clinic would place this model at risk, even if existing services are redistributed to meet the needs of the clinic.26,27,30 Nonetheless, service delivery models appeared to hold the greatest risk because they were strongly dependent on leadership, funding and staffing.24,25,31 The risks of the blended model could be mitigated if there was a lead agency or champion of the clinic that enabled the clinic to adapt and grow/change depending on current service resources, workforce development needs and community needs.14,15,24,25
Proposed model for a student-assisted clinic in a remote Queensland community
Based on the findings of this review, a blended model was proposed for a local student-led clinic in remote Australia, using a practice and a community-need blended model. The student-assisted clinic would be supported within current funding and services, with the local university department of rural and remote health providing in-kind resources and support (students, training, assessments and supervision) and the local public health service leading the clinic through a collaboration between three key health teams (paediatrics, allied health and mental health). An action research framework was also proposed to allow the team to improve the model through continuous feedback from services, health professionals, consumers, students and the local community.
Limitations
There are two main limitations with this review. The first is time. The review was conducted to inform the student-assisted clinic model to be utilised later the same year. It is possible that a longer, more comprehensive review would have identified other research that may have met the inclusion criteria.
The second limitation is language. We only considered papers written in English. This has likely resulted in a cultural bias, losing the richness of data that may have been produced if articles in other languages had been included.
Conclusions
Student-assisted clinics are an important component of a rural and remote health workforce, particularly when there are service gaps that needed addressing.
We identified a working definition for student-assisted clinics that can inform future research, with an operationalisation of the models used to deliver these clinics. These definitions may be useful to measure outcomes for student-assisted clinics.
The results of this review may also provide guidance and recommendations for developing sustainable student-assisted clinics, providing opportunities to expand on the current models, especially in more disadvantaged and isolated communities across the globe.
There is also an opportunity to formalise student-assisted clinics within workforce development strategies, providing opportunities to meet local workforce needs even in the face of health challenges, such as a global pandemic.
Supplemental Material
Supplemental Material - Rapid evidence assessment of student-assisted assessment and brief intervention clinics: Addressing the gaps in rural and remote health care
Supplemental Material for Rapid evidence assessment of student-assisted assessment and brief intervention clinics: Addressing the gaps in rural and remote health care by Sharon M Varela, Georgia Wells, Mason Henderson, Danielle Collins, Lynette Stenhouse and Prema Subramaniam in Journal of Health Services Research & Policy.
Footnotes
Acknowledgements
The Murtupuni Centre for Rural and Remote Health and the North West Hospital and Health Service provided in-kind resources and support to conduct this review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.