
Abstract
Objectives
Asthma is a prevalent chronic condition that affects approximately 300 million people worldwide, posing a significant health and economic burden. Effective management is often hindered by barriers to in-person care. Telehealth has emerged as a potential solution to enhance access to asthma care, yet its economic implications remain unclear. This review synthesizes evidence on the cost-effectiveness of synchronous telehealth compared to standard asthma care.
Methods
A systematic search of eight electronic databases (MEDLINE, EMBASE, Web of Science, CINAHL, Cochrane Library, Tufts Cost-Effectiveness Analysis Registry, NHS Economic Evaluations Database, and EconLit) was conducted from January 2000 to June 2024, with searches repeated in January 2026, for economic evaluations of telehealth interventions in asthma care. The reporting quality was assessed using the CHEERS checklist, and results were synthesized narratively.
Results
Four studies (published between 2005 and 2008) from high-income countries (UK and Australia) assessed telephone-based telehealth over periods ranging from 3 to 12 months compared to in-person care. Telehealth interventions resulted in higher asthma review rates, shorter visit durations, and lower costs per consultation but showed no consistent improvements in asthma control or quality of life.
Conclusions
Synchronous telehealth appears to be a cost-effective approach for increasing asthma review rates. However, evidence of its impact on quality of life and symptom control remains limited. Further recent studies with improved reporting are required to assess the long-term health economic value of telehealth in asthma care.
Introduction
Asthma is a heterogenous, non-communicable allergic disease characterized by chronic airway inflammation and identified by symptoms such as coughing, breathlessness, wheezing and sputum production.1,2 Asthma continues to be a significant global health issue, affecting an estimated 300 million individuals worldwide as per the Global Initiative for Asthma (GINA) 2024 report, with future increases expected. 1 Asthma imposes a significant economic burden on healthcare systems, individuals, and society. The economic burden of asthma is primarily driven by direct medical costs, such as hospitalizations, medications, and doctor visits, as well as indirect costs, including lost productivity and missed work or school.2,3 The costs associated with asthma vary across countries, whether at the individual patient level or on a broader societal scale. 4 For example, in Europe, the average cost per patient per year is estimated to be approximately USD $1,900, while in the United States, the estimated average cost is around USD $3100 per patient annually. 4
Asthma disproportionately impacts low-income and rural populations, contributing to health inequalities and posing a challenge for policymakers aiming to allocate resources effectively. 5 Poor adherence to medications and inadequate follow-up leads to symptoms exacerbations, hospitalizations, poor quality of life and increased healthcare costs in people with asthma.6,7 The sub-optimal control of asthma is also associated with limited access to healthcare. 8 Access to healthcare that involves in-office visits can be challenging for several reasons, including patient circumstances such as distance and travel expenses, provider availability and more recently, the experience of a pandemic, 9 thus highlighting the need for alternative care models. Telehealth has emerged as a potential solution to improve chronic disease management while reducing costs. 10
The effectiveness of telehealth modalities in asthma management remains inconclusive, particularly regarding healthcare resource utilization, asthma control, and quality of life (QoL). A Cochrane review of 17 studies found that telehealth interventions of various modalities significantly improved QoL compared to standard care. 11 Conversely, another systematic review of 14 randomized controlled trials (RCTs) reported mixed results on exacerbation rates, asthma control, and QoL. 12 McLean et al.'s meta-analysis found no significant improvements in emergency visits or QoL but noted reduced hospital admissions for severe asthmatics using interactive digital interventions. 13 Conversely, another meta-analysis focusing on adults indicated substantial improvements in asthma control and QoL with digital interactive interventions. 14 These inconsistent findings may stem from variations in the telehealth models evaluated, including synchronous, asynchronous, and hybrid approaches. Synchronous telehealth involves real-time interactions between patients and healthcare providers, typically via video conferencing or telephone calls, allowing for immediate communication. In contrast, asynchronous telehealth occurs at different points in time, such as in the store-and-forward model, where patients’ health data are transmitted to healthcare providers for review and response. Hybrid telehealth combines both models.
The economic impact of telehealth remains largely overlooked, despite its role in assessing care model value. A systematic review explored the economic value of telehealth across chronic conditions found significant cost savings, mainly from reduced travel and hospital visits, while improving access in remote areas. 15 Telehealth was identified as cost-effective for specialist care and home services but lacked asthma-specific studies. 15 Economic evaluations of internet-based and mobile interventions employing mixed communication strategies, self-monitoring, and treatment have yielded conflicting cost-effectiveness results compared to standard care.16,17 However, the review did not assess synchronous telehealth and its economic implications for adults with asthma.
Rationale for conducting this review
Currently, no systematic review has been conducted to synthesize the cost-effectiveness of telehealth for the adult asthma population. Understanding the economic and health impacts of synchronous telehealth interventions that replicate traditional face-to-face care is crucial for determining their potential to enhance clinical outcomes, improve access to care, and reduce healthcare costs.
Aim of review
The review aims to synthesize the cost-effectiveness evidence of synchronous telehealth (real-time interaction between practitioners and patients) compared to usual care (in-person visits) for asthma management. Asthma care includes routine review, follow-ups, education and/or consultations.
Methods
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines 18 (See PRISMA checklist, Online Supplement 1).
Protocol registration
This review was registered with PROSPERO (CRD42024555338) on 18 July 2024.
Eligibility criteria
Population
Adult participants (≥18 years old) diagnosed with asthma, regardless of severity or clinical characteristics, were included. Studies focusing on individuals under 18 years old were excluded.
Intervention
A real-time synchronous patient-practitioner interaction, using video calls, telephone consultations or both. Studies were excluded if they focused solely on the effectiveness of asynchronous communication, such as web-based platforms, mobile apps, or store-and-forward models, or if they lacked real-time interaction. Additionally, telehealth interventions designed exclusively to assess patient or workforce satisfaction were excluded.
Comparator
Usual care was delivered face-to-face. Studies comparing two telehealth modalities (synchronous or asynchronous) without a face-to-face comparator were excluded.
Outcomes
Primary outcomes such as Incremental Cost-Effectiveness Ratios (ICERs) and Net Monetary Benefit (NMB) were planned for assessment. A wide range of asthma-specific measures, in addition to intervention costs, were considered, including asthma control, asthma-related quality of life and health service use.
Study types
Any experimental and observational studies with both cost and effectiveness outcomes, including cost-effectiveness analysis (CEA), cost-utility analysis (CUA), cost-benefit analysis (CBA), cost-consequences analysis (CCA) and cost-minimization analysis (CMA) were included.
Information sources and search strategy
The search strategy employed medical subject headings (MeSH) and their equivalents to target (i) asthma, (ii) telehealth/telemedicine, and (iii) economic evaluations. The search strategy was developed collaboratively with a medical librarian and was applied to MEDLINE (Ovid), EMBASE, Web of Science, CINAHL, Cochrane Library, Tufts Cost-Effectiveness Analysis Registry, NHS Economic Evaluations Database, and EconLit from January 2000 to June 2024. Searches were repeated in January 2026, when no new results were found. Additionally, the reference lists of review studies on the economic evaluation of telehealth interventions were hand-searched. Only English-language articles were included. Detailed search strategy and results for each database are provided in Online Supplement 1.
Selection process
Records from database searches were managed using EndNote 20.6, where duplicates were identified and removed. Screening was conducted manually via Covidence online software (no automated or machine-assisted functions were used), with two independent reviewers (A.T. and E.J.) assessed titles, abstracts, and full texts against inclusion criteria. Disagreements were resolved through consultation with a third reviewer (C.P.).
Data extraction
Data extraction was performed by A.T. using a standardized form in Microsoft Excel 2407, with F.H. verifying accuracy. Discrepancies were resolved through discussion with a third reviewer (V.M.). Extracted data included study details (lead author, year, design, sample size, aim), economic evaluation methods (perspective, currency/year, time horizon), intervention type, comparator, healthcare resource utilization, effectiveness outcomes, incremental costs, and conclusions. Outcomes were categorized into clinical effectiveness, service utilization, and cost measures for synthesis.
Reporting quality assessment
The quality of reporting in the economic evaluation of health interventions was assessed using the Consolidated Health Economic Evaluation Reporting Standards (CHEERS 2022) guidelines. 19 The 28-item CHEERS checklist ensures that findings from all types of health economic evaluations are interpretable and useful for decision-making but does not assign a score. The checklist was completed by one reviewer (A.T) and verified by a second reviewer (F.H). Any disagreements were resolved through discussion with a third reviewer (V.M). No studies were excluded based on quality assessment.
Data synthesis
Due to the limited number of economic evaluation studies and heterogeneity in reported economic outcomes, effectiveness measurement tools and summary statistics across the four selected studies, a meta-analysis was not feasible. Therefore, a narrative synthesis was conducted. To ensure comparability and accuracy, costs were adjusted to 2024 USD using a web-based tool incorporating Gross Domestic Product (GDP) price deflators index and Purchasing Power Parity (PPP) conversion rates. 20
Results
Search summary
A flowchart illustrating the selection process and excluding reasons is presented in Figure 1. The database search yielded 5271 articles, with 500 identified as duplicates. The remaining 4771 articles were screened based on their title and abstract against the predefined inclusion and exclusion criteria. Following this, 29 articles were selected for full-text review, of which 25 articles were excluded for not meeting one or more of the inclusion criteria. A subsequent review of the reference lists from studies on the economic evaluation of telehealth did not identify any additional eligible articles. As a result, four studies were included for full text review. PRISMA flow chart.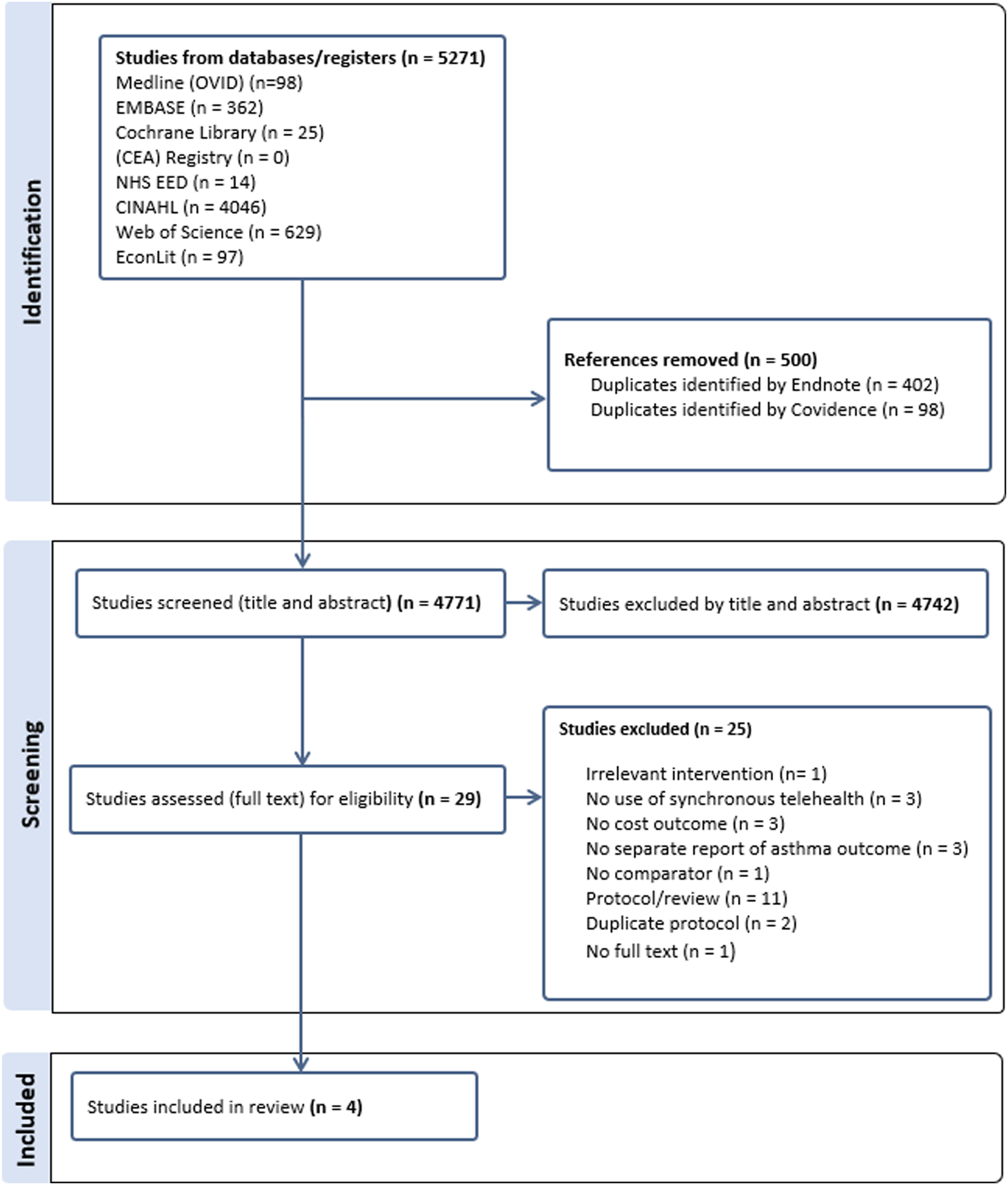
Data extraction and synthesis were conducted for four articles.21–24 One additional related paper 25 was used to supplement data extraction for completeness, as the authors referred to the trial paper for certain aspects of their economic analysis. 21
Study characteristics
Study characteristics.

Abbreviations: RCT randomized controlled trial, QoL quality of life.
Each study was an economic evaluation conducted alongside a randomized controlled trial (RCT), with two studies assessing different stages of the same trial.21,23 Of the 4 studies, two focused on an active asthma population related to the same trial. 21 One study targeted asthmatic patients with a history of hospital admission in the previous year,22,23 while the remaining study did not report any specific asthma-related clinical characteristics. 24
The four included studies involved either telephone-only interventions or optional appointments for asthma reviews, with face-to-face as a comparator. None of the studies incorporated video consultations or hybrid telehealth models combining telephone and video.
Assessment of reporting quality
The quality of reporting in health economic evaluation studies was assessed using the CHEERS 2022 checklist. 19 This tool was initially published in 2013 26 ; however, all included studies were published between 2005 and 2008, predating the checklist’s existence.
Quantitative scoring of the studies is beyond the scope of the CHEERS guidance and is strongly discouraged by the CHEERS panel. 19 Therefore, we narratively assessed the reporting of key economic items. Only one study was identified as an economic evaluation in its title, 21 and none of the included studies indicated whether a pre-developed health economic analysis plan was used.
Most studies reported objectives and methods, including descriptions of comparators, selection, measurement, and valuation of outcomes and costs, as well as uncertainty analysis. However, price dates22–24 and discount rates21–23 were not consistently reported. Additionally, three studies lacked clarity regarding their economic evaluation methods, complicating the interpretation of their findings.22–24 Furthermore, only two studies specified the perspective of their analysis, and neither justified their chosen perspective.23,24 There was also poor reporting in all studies regarding the adjustment and estimation of results for different subgroups. Lastly, none of the studies addressed ethical implications or equity considerations, which could impact patients, policy, or practice.
Clinical effectiveness and asthma-related outcomes
In half of the included studies, asthma review rates were the primary effectiveness measure for telehealth interventions, with significant improvements observed in two studies (12.6% to 26%, p < .001) compared to in-person care.21,23 Asthma-related quality of life was the most common secondary measure, assessed using the Mini-AQLQ in three studies,21,23,24 while the MAQLQ-M was used in Donald et al. (2008). 22 One study evaluated asthma control as a primary outcome, and another as a secondary outcome, both using the ACQ over 12 months23,24 Hospital readmission was assessed in one study over the same period. 22
Results indicated a trend toward improved asthma-related quality of life in the telehealth group across three studies, reaching statistical significance in one (p = .015). 24 Donald et al. reported a clinically significant quality-of-life improvement with the MAQLQ-M, absent in the control group. 22 Although ACQ scores showed health status improvements in two studies, these improvements were not statistically significant at 12 months (p = .349 vs p = .19).23,24 A reduction in hospital readmissions was reported in the telehealth group but did not reach statistical significance (P = .07). 22 Clinical effectiveness measures are summarised in Table S1.
Economic analysis
Other than Pinnock et al. (2005), the included studies did not explicitly report their methods of economic evaluation,21–24 and none of the four studies employed model-based analyses, such as decision-analytic or Markov models, relying instead on trial-based data with relatively short time horizons. Pinnock et al. (2005) and a related 2007 study categorized their analysis as CEA.21,23 The Gruffydd-Jones study was classified as a CMA, assuming similar asthma symptom control across groups, with National Health Service (NHS) costs independently reported. 24 Donald et al. (2008) presented intervention and hospital readmission costs separately, classifying the study as CCA. 22 Two studies identified the NHS (UK) as their economic perspective.21,24 None of the studies considered productivity losses, direct non-medical costs, or non-health sector costs. As a result, both patient and societal perspectives were excluded, as outlined by Sittimart’s framework. 27
Details of economic analysis of included studies.
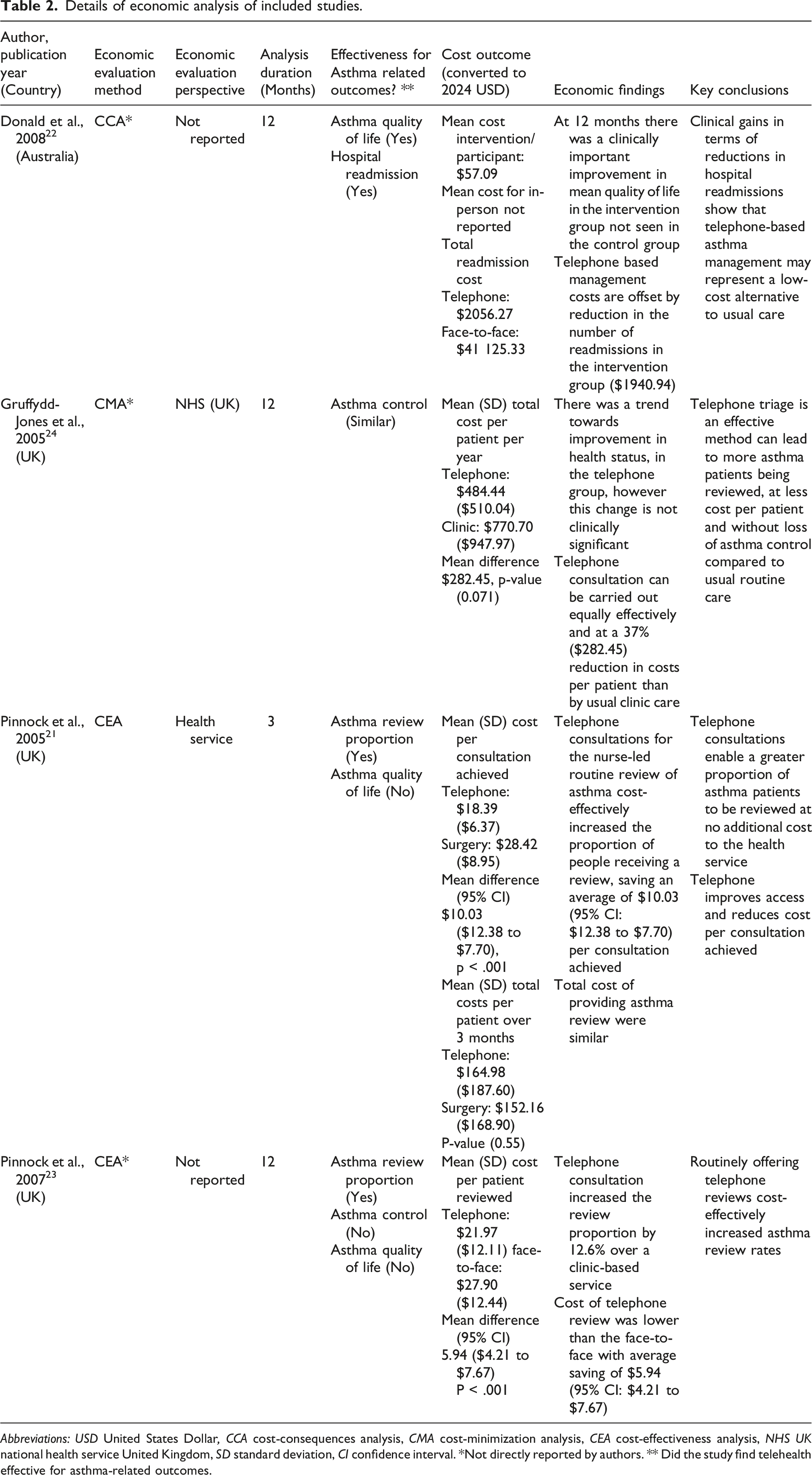
Abbreviations: USD United States Dollar, CCA cost-consequences analysis, CMA cost-minimization analysis, CEA cost-effectiveness analysis, NHS UK national health service United Kingdom, SD standard deviation, CI confidence interval. *Not directly reported by authors. ** Did the study find telehealth effective for asthma-related outcomes.
Discussion
The present study, as far as we are aware, is the first systematic review of economic evaluation studies focused on synchronous real-time telehealth intervention for adults with asthma. Although telehealth interventions began several decades ago and have experienced substantial growth, economic evaluations of synchronous telehealth for asthma care with adult population are still rare. The absence of recent evidence is notable given the rapid technological, regulatory and reimbursement changes that have occurred in telehealth delivery over the past decade, particularly following the COVID-19 pandemic.28,29 Restricting inclusion to synchronous telehealth interventions among adult was intended to maximise conceptual comparability with traditional face-to-face asthma management. Synchronous consultations mirror traditional care in structure, duration and resource utilization, facilitating more accurate estimation of costs and outcomes. Asynchronous models, such as store-and-forward or app-based interventions that are increasingly employed in both adult and paediatric population,30,31 were excluded as these modalities differ substantially in delivery, frequency of clinician inputs and cost components.
Many studies lacked clarity in reporting economic evaluation items, 19 and were not explicitly identified as economic evaluation, which posed challenges in understanding their analytic approaches and interpretation. The poor reporting quality of the included studies, as assessed using the CHEERS checklist, 19 further limit confidence in the findings. Key methodological details, such as economic perspective, costing methods, and uncertainty analysis were largely omitted. Additionally, none adopted a societal perspective. Potential benefits of telehealth, such as reduced travel time, out-of-pocket savings and productivity gains for patients are central to policy arguments for telehealth expansion. Excluding these cost components is therefore likely to underestimate the full economic value of telehealth interventions.15,32
Findings suggest telephone-based interventions are cost-effective for increasing asthma review rates, primarily due to reduced nurse time and shorter consultations duration. 33 While one study reported a non-significant reduction in hospital readmissions, the associated cost savings were substantial. 22 These findings indicate the potential for synchronous telehealth interventions to effectively manage asthma while reducing overall healthcare costs. However, none of the studies examined videoconferencing-based care. Evidence from other chronic disease contexts suggests that videoconferencing may be associated with improved clinical outcomes and patient engagement compared to telephone-based models, particularly where visual assessment and interaction are clinically relevant. 34
Hospital admission rates are often used as key indicators for tracking progress in asthma care, 2 yet studies evaluating telehealth interventions employ multiple outcome measures to assess effectiveness and cost-effectiveness. Most evidence does not demonstrate significant differences between telephone and face-to-face care in improving health outcomes, particularly asthma control and QoL. These findings align with a Cochrane meta-analysis that evaluated the benefits of various remote care models from six RCTs, two of which were also included in our review. 35 Similarly, another meta-analysis, which pooled the effects of asthma control and QoL using the same measurement tools, revealed no clinically significant differences when using interactive digital interventions. 14 Importantly, none of the included studies assessed medication adherence in relation to telehealth interventions, despite its critical role in preventing disease exacerbation.6,7,36 Nevertheless, reductions in hospital readmissions and healthcare utilization resulting from the interventions22,24 could indirectly suggest improvements in medication adherence. 36
Cost differences favouring telehealth were mainly attributed to shorter consultation times and increased patient review rates.21,23,24 The variation in cost items and timeframes across studies does not contradict the overall findings that telehealth interventions for asthma review yield cost savings compared to face-to-face care; a similar pattern has been observed in broader chronic disease telehealth research where home telehealth and remote monitoring were associated with lower average costs per patient. 37 Longer interventions duration and broader inclusion of cost items (e.g., patient and societal perspectives) may yield different results, potentially unmasking additional economic benefits. Evidence from a systematic review of telehealth for chronic conditions suggests that reductions in travel time, clinician time, and other utilization factors are common drivers of cost savings and improved efficiency in telehealth models compared with traditional care. 29 While telephone consultations did not demonstrate superiority over in-person care in reducing healthcare utilization or improving asthma control, they effectively encouraged access to asthma care and cost-effectively improved review rates.
Despite lack of recent available evidence, the findings remain relevant to current policy debates concerning telehealth funding decisions and equity of access. 28 Telehealth is frequently promoted as a mechanism to improve access to chronic disease care in rural and underserve population 38 ; however, the absence of recent economic evaluation limits policymakers’ ability to assess value for money. This review highlights the need for rigorous, policy-relevant economic evaluation within modern telehealth programs.
Limitations
This review has several limitations. The small sample size (four heterogeneous studies) and restriction to two high-income countries (Australia, UK) limit the generalizability of the findings to lower-income settings. The narrow scope of the inclusion criteria likely contributed to the limited number of eligible studies. The absence of videoconferencing studies also limits the applicability of the findings to current practice, given the increasing use of videoconferencing. Furthermore, as the reviewed studies confined the economic evaluation to a healthcare perspective, the review cannot account for costs related to patients and society. The lack of blinding in some studies may have introduced bias and the short study durations prevented long-term impact assessments. Selection bias is also possible, as only English-language studies were included. Moreover, the reviewed studies were published between 2005 and 2008. These deficiencies hinder comparability across studies and increase the risk of bias, suggesting that conclusion regarding cost-effectiveness should be interpreted cautiously.
This review provides insights into the outcome measures used to evaluate the costs and effectiveness of synchronous telehealth services for individuals with asthma, highlighting how the choice of these measures impacts the findings of economic evaluations, and summarises the relevant evidence base at this point in time. The insights gained could inform the design of future long-term economic evaluation studies aimed at assessing the sustainability of these initiatives in the context of adult asthma management.
Conclusions
Synchronous telehealth appears to be a cost-effective model for increasing asthma review rates and may contribute to reducing hospitalizations. However, there is a lack of economic evidence regarding quality of life and symptom control. Future studies should focus on these aspects while improving the quality of economic reporting in telehealth evaluations.
Supplemental material
Supplemental material - Cost-effectiveness of synchronous telehealth versus face-to-face care for asthma management: A systematic review
Supplemental material for Cost-effectiveness of synchronous telehealth versus face-to-face care for asthma management: A systematic review by Aisha Towhari, Victoria McCreanor, Xenia Dolja-Gore, Penny Reeves, Ebbah Jiriengwa, Finn Hamilton, Christine Paul in Journal of Health Services Research & Policy
Footnotes
Acknowledgments
The authors thank Research Librarian Jessica Birchall at the University of Newcastle for her assistance in updating the search strategies. AT was supported by a postgraduate scholarship from Saudi Electronic University and the Ministry of Education of Saudi Arabia.
Author contributions
AT led the design of the study together with VM, XD, PR and CP. AT conducted the literature search. AT led study screening and data extraction. EJ contributed to the study screening. FH independently verified the data extraction. AT completed the data analysis and drafted the manuscript. CP, VM, XD and PR contributed to interpretation of the results. All authors critically reviewed the manuscript and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Relevant data for this review, including the data extraction form, extracted data, CHEERS checklist for reporting quality assessment, and other supporting materials can be provided by the first author upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.