
Abstract
Introduction
This systematic review aimed to synthesize evidence on the key findings of evaluations of implementation of models of care in rehabilitation and describe facilitators and barriers to implementing new models of care.
Method
Six electronic databases were searched. Abstracts and full texts were screened and critically appraised. Facilitators and barriers were classified using the Consolidated Framework for Implementation Research version 2.0.
Results
Of the 64 studies identified, 52 (81%) were new care models implemented in a hospital and 12 (19%) were situated in a home or community-based setting. Common implementation evaluation metrics reported included fidelity (n = 15), adherence (n = 16), feasibility (n = 14), and acceptability (n = 12). Facilitator domains were innovation source (e.g., uncomplicated models), outer setting (e.g., positive attitude), inner setting (e.g., teamwork or motivation), individuals (e.g., skill) and implementation (e.g., planning according to need and context). Barrier domains were innovation source (e.g., model complexity), outer setting (e.g. .organisational culture), inner setting (e.g., staff turnover, training, or resources,), individuals (e.g., no champions) and implementation (e.g., lack of planning).
Conclusions
The review highlights the importance of planning before implementing new models of care in rehabilitation settings to address potential facilitators and barriers in a real-world environment.
Keywords
Introduction
According to the World Health Organization (2023), 2.4 billion people worldwide have a chronic health condition that could benefit from some form of rehabilitation. 1 Rehabilitation as a result of a chronic disease or injury involves an individual participating in a series of interventions (i.e., a care delivery model) that aim to reduce disability and optimise function. 1 Rehabilitation often enables an individual to be as independent as possible in their activities of daily living, and enables their participation in social, work, educational, and other activities. 1 In Australia, one in two people are estimated to have a chronic health condition, 2 accounting for two-thirds of the total burden of disease and injury. 3 Injury alone accounts for 7.6% of medical costs and 8.1% of the disease burden. 4 With the increasing demand for rehabilitation services and finite resources, new models of care that can both aid recovery and support access and ease of delivery are being implemented and trialled.5–7
Rehabilitation is a crucial component of the healthcare system that can assist people to regain their physical functioning after sustaining an injury or disease. 1 The provision of rehabilitation services can be influenced by many factors, such as the available healthcare infrastructure, funding mechanisms, prioritisation, accessibility of rehabilitation services, availability of health professionals, and resources. 8 Determining what factors are critical for the successful implementation and delivery of rehabilitation services, including the implementation of new rehabilitation care models, will support successful implementation of new care models across different rehabilitation settings.
Rehabilitation practices are constantly evolving, with new care models being introduced and evaluated.9–11 Rehabilitation can be provided in locations such as inpatient, outpatient, in the home or community-based settings.12,13 Care models may be applicable across several settings, yet what factors contribute to the successful implementation of new care models across rehabilitation settings are not widely reported. It is important to identify factors that can aid implementation of rehabilitation care models in real-world settings.
Evaluating the implementation of a new care model has the ability to shed light on how closely the delivered care aligns with the intended model (adoption), how closely the implementation resembled what was planned (fidelity), how many individuals received care under the new model (reach), how appropriate the care model is for patients and health professionals (acceptability), the cost-effectiveness of implementing the new model, and the feasibility and sustainability of the care model long-term. 14 Evaluating care model implementation can assist in drawing attention to areas that require improvement. Identifying facilitators and barriers to the implementation process can also aid in the identification of what works, or does not work well, and why. However, an awareness of factors that can aid or hinder implementation of new care models in rehabilitation settings is lacking.
Previous studies have examined the implementation of care models for individuals undergoing rehabilitation.14–17 However, little has been reported on the evaluation of the implementation of new care models in a rehabilitation setting across health conditions. There may be opportunities to learn from different approaches in implementing care models across rehabilitation settings and to identify common barriers and facilitators to implementation that would aid the planning for the implementation of new care models for rehabilitation. The aim of this systematic literature review was to synthesise evidence on the evaluation of the implementation of new models of care in rehabilitation and describe facilitators and barriers to implementing new models of care for patients in a rehabilitation care setting.
Methods
This systematic review adhered to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement. 18 The review protocol was not pre-registered.
Definitions and conceptual model
For this review, rehabilitation was considered to be a set of interventions used to reduce and optimise the limitations or disability of an individual with a physical health condition (excluding drug and alcohol rehabilitation and interventions related to mental disorders), and could take place in hospital, in the community or in the home. 1 A model of care describes a best practise approach for the delivery of care, often using a care guideline or protocol. 19 For this review, a new model of care was considered as the introduction of a model of care that includes either one or more new interventions into a rehabilitation setting, or the introduction of one or more existing interventions that had not previously been implemented in a rehabilitation setting, excluding virtual care models.
The term ‘implementation’ in healthcare describes the process of putting evidence-based interventions into best practice.20,21 Implementation for this review was defined as specific strategies, measures, or methods of a rehabilitation program that were intended to be delivered using a model of care. Implementation evaluation measures considered included adoption, acceptability, appropriateness, feasibility, fidelity, implementation cost, reach, penetration, and sustainability (Supplemental file 1). Barriers to implementation were considered to be challenges that had a negative impact on the introduction of a new model of care, whereas facilitators to implementation were considered to be factors that supported the introduction of a new model of care. 21 In this review, the same components could be coded as barriers or facilitators depending on their observed effect on implementation.
The revised Consolidated Framework for Implementation Research (CFIR) was utilised to categorise the facilitators and barriers identified. 22 The CFIR is a meta-theoretical framework that can be used to identify contextual determinants of an implementation process. It includes five major domains 1 : innovation (e.g., innovation source, evidence based, relative advantage, adaptability, trialability, complexity, design and cost); 2 outer settings (e.g., critical incidence, local attitudes, local conditions, partnerships and connections, policies and laws, financing, external, social and market pressure, performance measurement pressure); 3 inner settings (e.g., structural characteristics, relational connections, communications, culture, tension for change, compatibility, relative priority, incentive system, mission alignment, available resources, access to knowledge and information); 4 individuals (e.g. high level, mid-level and opinion leaders, implementation facilitators, leads and team members, other implementation support, innovation delivers and recipients); 5 and implementation process (e.g. teaming, assessing needs, assessing context, planning, tailoring strategies, engaging, doing, reflecting and evaluating and adapting). For this review, any subdomains of CFIR were classified under the related domains and constructs.
Data sources
Six electronic databases were searched from 1 January 2000 to 14 March 2025: CINAHL (EBSCOhost), MEDLINE (Ovid), AMED (Ovid), Embase (Ovid), Scopus, and Web of Science. The search strategy was developed with a university research librarian, and keywords related to the following key concepts: (a) rehabilitation; (b) model of care; (c) implementation; and (d) evaluation. Search terms for the key concepts were combined using the Boolean operators (Supplemental files 2-7). Additional relevant articles were identified by backwards citation tracking of the reference lists of included studies.
Eligibility criteria
Studies were selected based on the following eligibility criteria. Inclusion criteria were studies that: (a) evaluated or described the implementation of a new model of care in rehabilitation settings (e.g., hospital-, community-, and home-based); (b) identified any barriers or facilitators during the implementation of the new model of care; (c) were original research articles, clinical trials, qualitative or quantitative or mixed methods studies; and (d) included an adult population aged ≥18 years. Exclusion criteria were studies that: (a) were published in languages other than English; (b) were published before 2000; (c) described the development or validation of a measure (e.g., clinical tool, guideline) and its impact on patient outcomes, but did not describe any implementation measures and strategies; (d) included a paediatric population aged <18 years; (e) that evaluated drug and alcohol rehabilitation, vocational rehabilitation, and care delivery models or interventions related to mental disorders; (f) evaluated the introduction of virtual care models or telerehabilitation models; (g) evaluated an intervention or care model that included pre-operative interventions where the rehabilitation setting could not be specifically examined; (h) evaluated adherence to existing clinical guidelines; and (i) were review articles, study protocols, conference abstracts and papers, books, book chapters, theses, case reports, and case series.
Study selection process
The full citation information including title and abstract of each article identified from the search strategy was imported into Endnote X20 (Clarivate, London, United Kingdom) and duplicates removed. Unique records were imported into Covidence (Veritas Health Innovation, Melbourne, Australia). Covidence is a web-based software program that allows multiple reviewers to screen records against inclusion and exclusion criteria. Covidence was used both for title and abstract, and full text screening. Three reviewers independently conducted the initial screening of the titles and abstracts in pairs (NBH and RJM, NBH and RPL). If any abstract did not meet the inclusion criteria, it was excluded. If reviewers could not determine whether the study should be included or excluded, the study was discussed, and a decision was made with 100% consensus among the three authors (NBH, RJM and RPL).
For full text screening, each of the potentially eligible studies was assessed and appraised by three reviewers in pairs (NBH and RJM, NBH and RPL). Any studies that did not meet the inclusion criteria were excluded. Disagreements were discussed and consensus reached.
Data extraction
For studies that met the inclusion criteria, the following data were extracted: (a) study characteristics (i.e. author and publication year, study objectives, study design, location, sample size, type of rehabilitation settings); (b) description of the intervention or new model of care; (c) implementation evaluation outcomes; and (d) facilitators or barriers to implementation. Data extraction was initially performed by one reviewer (NBH) and verified for accuracy by two reviewers (RJM, RPL). Any disagreement was discussed among the three review authors (NBH, RJM, RPL) and resolved by mutual consensus.
Quality assessment
The methodological quality of the included studies was independently assessed by one reviewer (NBH) and verified for accuracy by two reviewers (RJM, RPL) using the Mixed Methods Appraisal Tool (MMAT), version 2018 (Supplemental file 8). 23
The MMAT comprises two screening questions and five domains. Each domain pertains to a type of study design (i.e., qualitative studies, quantitative randomized controlled trials, quantitative non-randomized studies, quantitative descriptive studies, and mixed methods studies) and contains methodological quality criteria that are scored either yes, no, or cannot tell. An overall quality score ranging from zero to five stars can be derived based the proportion of criteria in a domain that are rated yes: 100% (5 stars), 80% (4 stars), 60% (3 stars), 40% (2 stars), 20% (1 stars), and 0% (0 stars).23,24 For mixed methods studies, which are rated on three domains, the overall quality score is set as the lowest domain score.23,24 Any disagreement was discussed among the reviewers and resolved by mutual consensus.
Data synthesis
The information extracted from the included studies was tabulated and narratively synthesised. The narrative synthesis involved reviewing the facilitators and barriers reported in the results and discussion sections of each study and categorising the factors using the CFIR. The classification was conducted by one reviewer (NBH) using an inductive, iterative process, where each characteristic was classified, and appraised by two reviewers (RJM, RPL). Each barrier or facilitator identified was then categorised to one domain in CFIR, 22 and multiple factors could be identified for each study (Supplemental files 10 and 11).
Results
A total of 9044 records were identified during database searches. Of these, 885 records were duplicates and removed. After screening the titles and abstracts of the remaining 8159 records, 7961 records were excluded, and 198 potentially eligible studies were selected for full text screening. After full-text screening, 62 studies were included. Eleven articles were identified during backward citation searching and only two of those articles were included, resulting in 64 included studies (Figure 1).5–7,9–13,25–80 PRISMA flow chart.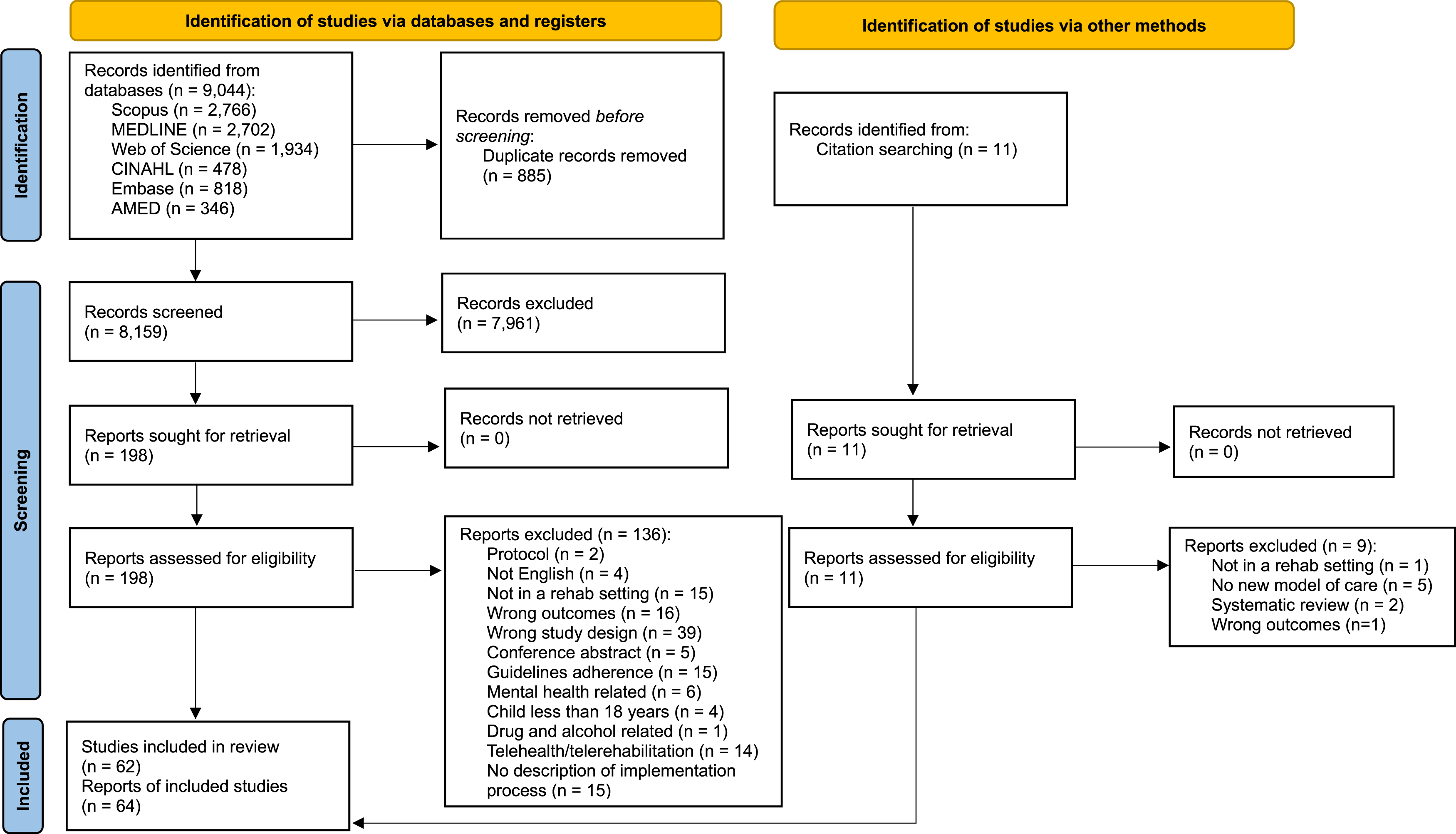
Characteristics of included studies.

AERO: an exercise adherence intervention; CR: cardiac rehabilitation; COPD: chronic obstructive pulmonary diseases; CAP-CR: care assessment platform on cardiac rehabilitation; GLAD: the good life with osteoarthritis: Denmark; ICU: intensive care unit; MAT: multimodal agility-based exercise training; N/A: not applicable; KF-NAP: Kessler Foundation neglect assessment process; KF-PAT: Kessler Foundation prism adaptation treatment; NR: not reported; PR: pulmonary rehabilitation; PRADO: programme d’accompagnement de retour a' domicile; REACH-HF: rehabilitation enablement in chronic heart failure; SD: standard deviation; SCI: spinal cord injury; SAT: strength and endurance training; TCR: traditional, centre-based rehabilitation.
aReporting on the implementation of the same intervention or model of care (i.e. REACH-HF).
bReporting on the implementation of the same intervention or model of care (i.e. KF-NAP and KF-PAT).
Twenty-seven (43%) studies employed mixed methods, 20 (32%) used qualitative methods, and the remaining 16 (25%) studies used quantitative methods. Most studies were hospital-based (81%, n = 52) and the remaining studies (19%, n = 12) were home, community-based, or involved mixed rehabilitation settings.
The mean age of participants across the sample ranged from 28.0 to 83.4 years. More than three-quarters of included studies (78%, n = 50) focused on new rehabilitation care models for chronic diseases and conditions including stroke, aphasia, atrial fibrillation, cancer, chronic obstructive pulmonary disease, chronic pain, frailty, musculoskeletal pain, Parkinson’s disease, and pulmonary hypertension. Eleven contributions (19%) assessed new models of care for injuries including spinal cord injury, hip fracture, or brain injury. Two studies (3%) examined rehabilitation models specifically for rural populations, and one examined the implementation of early rehabilitation in an intensive care unit.
Implementation evaluation outcomes in included studies by evaluation domain.

CAP-CR: care assessment platform on cardiac rehabilitation; MAT: multimodal agility-based exercise training; PR: pulmonary rehabilitation; SAT: strength and endurance training; SD: standard deviation.
Facilitators and barriers
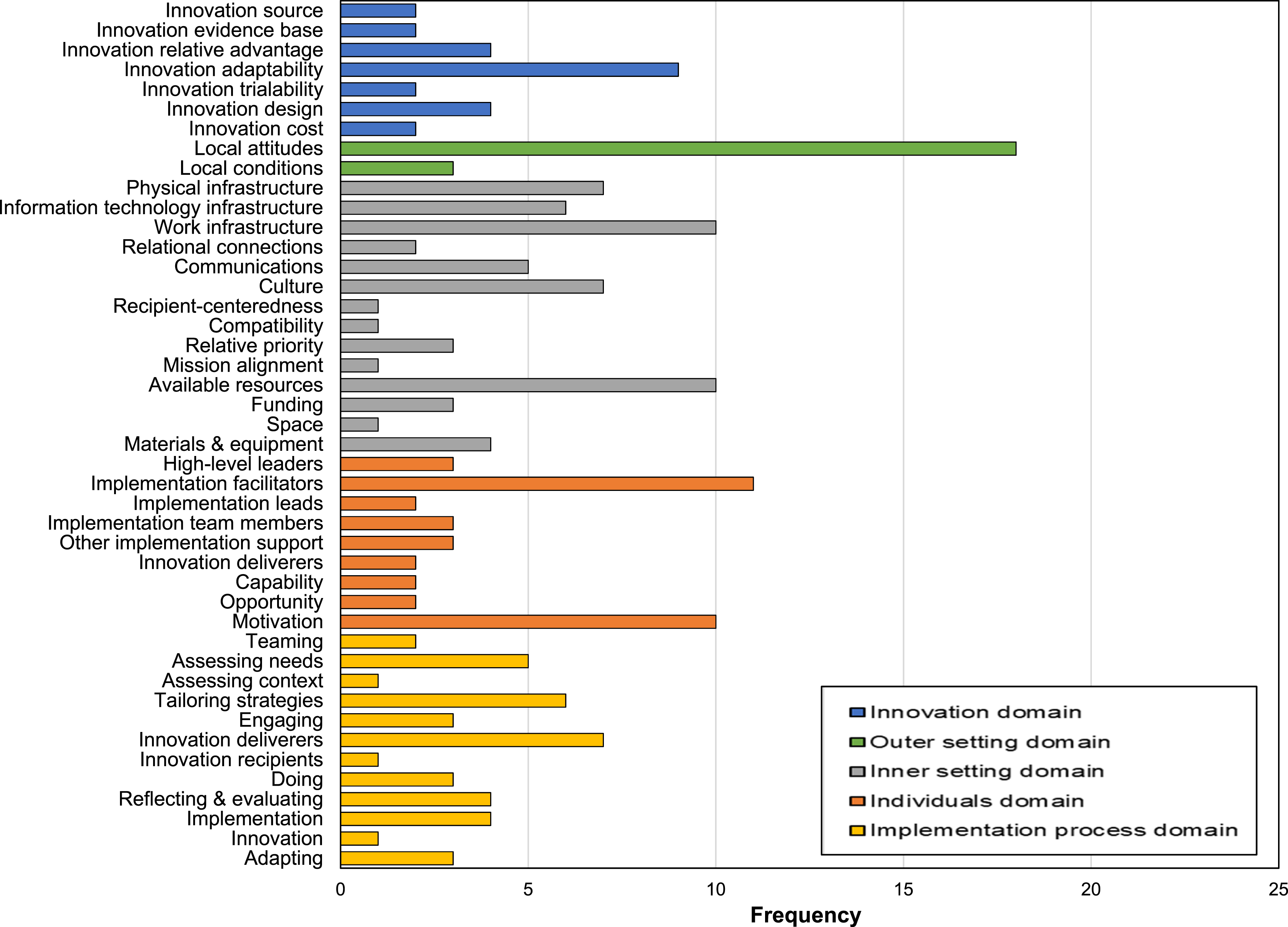
A total of 501 facilitators and barriers to the implementation of new models of care in rehabilitation were reported in five domains across 56 constructs of the CFIR (Figures 2 and 3; and Supplemental files, 10, 11 and 12).

Innovation source domain
Fifty-seven factors were reported across eight constructs in the innovative source domain. Of these, three constructs (innovation source, innovation evidence-base, innovation relative advantage) were reported as facilitators and one construct (i.e. innovation complexity) was reported as a barrier. Four constructs (innovation adaptability, innovation trialability, innovation design, innovation cost) were reported as both barriers and facilitators. Factors related to user-friendly online health applications (e.g., “the eHealth application was user-friendly … stimulated them to adhere to the treatment” [p8]), 11 easy to learn and individually adaptable care models, simple and easy referral processes (e.g., “having the navigator in the physical space … facilitate[d] near-real-time engagement with patients” [p4]), 68 flexible scheduling and prioritising the convenience of participants (e.g., “we restricted our timeframe … cut it short … for the patients” [p7]) 58 were cited as facilitators. Barriers included complex and inappropriate models (e.g., “model was not suitable for cognitive patients such as memory, concentration, problem-solving and initiation difficulties and neglect” [p9]), 50 time consuming rehabilitation sessions, and overlapping care models with existing rehabilitation interventions. 69
Outer setting domain
Seventy-four factors were reported across seven constructs for the outer setting domain. Of these, five constructs (critical incidents, policies and laws, financing, external pressure, performance measurement pressure) were reported as barriers. Two constructs (local attitudes, local conditions) were reported as both barriers and facilitators. Factors related to a positive attitude and enthusiasm of health professionals, the organisation of care delivery (e.g., “it’s very well laid out (therapist)” [p4], 41 “very helpful, very visual (patient)” [p7]), 32 healthcare provider job satisfaction, continuous staff training, feedback and monitoring regarding the implementation of the intervention were cited as facilitators. Barriers included negative attitudes and stigmatisation among staff and hospital management towards the intervention (e.g., “it has a large impact on our timetables (hospital management)”[p8], 69 “I actually found it had a negative impact on patients (staff)” [p6]), 50 negative responses from patients (e.g., perceptions that the intervention was not suitable for them), organisation policies and performance pressure (e.g., “therapists were under pressure to … make time to supervise the new intervention” [p5]), 50 and personal reasons for patient drop out from rehabilitation, such as sudden illness, lack of interest in continuing or being preoccupied with work.
Inner setting domain
One hundred and ninety-four factors were reported across 18 constructs for the inner setting domain. Of these, one construct (recipient-centeredness, for example, “a lot of patients have reported… they are doing it at the same time every day” (therapist))[p8] 50 was reported as facilitator and five constructs (information technology infrastructure, deliverer-centeredness, tension for change, compatibility, access to knowledge and information, e.g., “I worry that it (the intervention) won’t give you all the information (therapist)) [p7] 28 were reported as barriers. Eleven constructs (physical infrastructure, work infrastructure (e.g., “trying to contact the doctors and get them in position… is quite difficult……really busy unit”) [p6] 29 , relational connections, communications, culture, relative priority, incentive system, mission alignment, available resources (e.g., “we have lot of issues of lack of resources….there is nobody that can consistently be doing this except me” (clinician) [p5] 59 , funding, space, materials, and equipment (e.g. ,“ the availability of the equipment affects how much you can do with your patients” ))[p5] 40 were reported both as barriers and facilitators. Factors related to organisational support from higher management, using an interdisciplinary work approach to implementation, teamwork and effective communication (e.g., “I’ve had couple of patients… I don’t have the time to keep calling them”) [p4], 59 adequate funding for implementation, available resources, organisational measures (such as celebrating recruitment milestones by building a shared sense of community) were cited as facilitators. Barriers included inadequate equipment, high staff turnover and cutbacks, lack of staff access to information, problems with the internet or information technology (IT) system (e.g., slow and complex verification processes, inadequate IT systems to identify and track patients), lack of user ability and confidence among staff and patients with the technology, lack of onsite skilled professional support and training for staff, lack of a rehabilitation culture, lack of communication with general practitioners on site, and limited funding to support implementation.
Individual domain
Forty-eight factors were reported across 12 constructs in the individual domain. Of these, two constructs (implementation facilitators, implementation leads) were reported as facilitators and three constructs (opinion leaders, innovation recipients, need) were reported as barriers. Seven constructs (high-level leaders, implementation team members, other implementation support, innovation deliverers, capacity, opportunity, motivation) were reported both as barriers and facilitators. Factors related to prior expertise and knowledge of the implementation team, availability of local champions (e.g., “an implementation team of stakeholder champions … was a critical factor in facilitating implementation” [p5]), 68 and additional supports for patients (such as peer or family support) were cited as facilitators in the individual domain. Barriers included lack of expertise and knowledge about the delivery of the intervention by staff (e.g., “we’re just not always sure how to do it (therapist)”) [p3] 40 and lack of motivation towards the intervention from higher management, and staff.
Implementation process domain
Forty-one factors were reported across eleven constructs for the implementation process domain. Of these, three constructs (teaming, reflecting and evaluating, innovation) were considered as facilitators. Eight constructs (assessing context, assessing needs, tailoring strategies, engaging, innovation deliverers, doing, implementation, adapting) were reported both as barriers and facilitators for the implementation process domain. Factors related to tailored interventions according to patient’s health condition (e.g., “for patients prone to fatigue … teams planned their day, timetabling harder and lighter activities and rests across the day”), [p7] 58 implementation planning before delivery to engage more patients (e.g., “participants enjoyed, felt relaxed as the researcher made them feel comfortable and explained the treatments clearly”) [p9] 30 and staff buy-in were cited as facilitators in this domain. Barriers included variation in patient fitness level and illness, patients’ different preferences for practicing the rehabilitation sessions, and inconsistencies in physiotherapists expectations with patients’ abilities.
Quality assessment
Almost half of the included studies (n = 28; 48%) received an overall quality rating of 5 stars. Of the remaining studies, 18 studies (31%) were classified as 4 stars, six studies (11%) as 3 stars, four studies (7%) as 2 stars, and two studies (3%) as 1 star (Supplemental file 9).
Discussion
This review identified factors that were reported to have an impact on the implementation of new models of care for patients across rehabilitation settings and characterised these factors as barriers or facilitators using the CFIR. Common facilitators for successful implementation of new care models for rehabilitation were uncomplicated models, positive staff attitudes, support and motivation from peers and the organisation, teamwork, resources for implementation, staff prior knowledge and skill, and planning according to need and context before implementation of the model. Common barriers to the implementation of new care models for rehabilitation were complex models, negative staff attitudes, communication gaps, staff turnover, lack of a rehabilitation culture, lack of staff motivation, issues with IT, lack of staff training, limited funding, no implementation champions, and lack of implementation planning for model delivery.
Ideally, a care model should be simple to comprehend for both those implementing it and the people receiving the care. In the studies included in this review, simple, user-friendly, and individually adaptable care models worked as facilitators,28,44,56,58,68,70 while complex models worked as barriers.9,31,41,50,55,58,66,67,72,77 Models with flexible scheduling, that were affordable and had modifiable training sessions were commonly reported to be user-friendly and successful in terms of implementation acceptance, adherence, practicality, and fidelity.26,27,32,40,41,75,78–80 This demonstrates the importance of designing a care model with detailed and clear implementation steps for care providers that are also acceptable for participants.
Readiness to accept change can be influenced by organisational culture, whereas factors such as a supportive learning environment and positive staff attitudes have been associated with readiness to accept change.67,72,73,76,77 Demonstrated within the studies in this review, was the capacity for the local environment to influence implementation of new care models across rehabilitation settings. Implementation issues, such as the absence of an organisation-wide rehabilitation culture, as well as negative attitudes of staff and patients, were persistent in several studies.11,45,50,58 In some instances, negative attitudes of staff or patients, and their local beliefs was reported to hinder implementation, even if an organisation had a rehabilitation culture. 64 Engaging clinicians, management, and patients in care model development, with continuous monitoring and feedback, is likely to create a positive work culture. Bayley and colleagues particularly highlighted the importance of clinicians’ beliefs, attitudes, and strong organisational support to promote evidence-based care in rehabilitation. 31
Examining how organisational culture and attitudes interact may be useful for designing new care models. A number of studies identified communication gaps at the organisational level as barriers to implementation.7,39,45,53,58 This was particularly noticeable when a new care model overlapped with an existing model or was perceived as adding to staff workload. Effective communication among healthcare providers is a known facilitator in establishing a good interdisciplinary teamwork environment in healthcare.13,77,81
Prior knowledge, skills, and experiences of clinicians with a high degree of subject expertise were found to facilitate the implementation of a new model of care, along with support from patient families.44,54,58,59,62 New care models with support and motivation from peers and management were found to be effective in terms of patients’ adherence and were also identified as sustainable in the long-term.6,37,39,44,61,76,79,82 This review highlights the possibility of increasing a new care model’s acceptance and sustainability by leveraging positive views towards the new intervention or care delivery models. However, a lack of motivation can have the reverse effect, leading to implementation barriers. Manhas and colleagues demonstrated that a lack of motivation and unsupportive leadership were key challenges to the sustainability of their rehabilitation care model. 61
In this review, the implementation process was found to be influenced by the resources available. The most frequent cause of resource unavailability was staff turnover. Various strategies to reduce staff turnover, such as building a strong rapport among healthcare providers and explicit measures, such as celebrating achievements, or providing mentoring support were identified as useful strategies.38,72 A lack of access to information and a lack of knowledge and practical skill to deliver the care model elements were reported as barriers in several studies,35,45,58,62 demonstrating the need to design any care models with frequent training sessions and to provide professional support to staff during implementation. Similarly, Antypas and colleagues 83 also considered implementation resources and adequate staff as important factors in successful implementation of care models. 83
The review identified a lack of funds as an implementation barrier for new rehabilitation care models, particularly when the rehabilitation was carried out in a home-based setting.11,37,56,73 Two studies offered patients reimbursement or complimentary sessions to offset individual patient rehabilitation costs.36,38 However, cost barriers highlight the importance of ensuring necessary funding is available prior to starting implementation of a care model. Adequate long-term financial resources are crucial in terms of long-term sustainability.
The review also brought to the fore issues with IT infrastructure as a key barrier. Common IT issues reported were complex online applications or apps, participants’ lack of access to the internet and lack of capability to use apps. Problems with IT highlight the necessity of creating a care model that is easy and adaptable to the needs of the participants. The review findings are consistent with other studies that have recommended the customisability and personalisation of technology to make applications easy to operate independently for a wide range of potential users. 8
A lack of a local implementation champion was noted as a barrier.44,62 Engaging local champions has been found to facilitate implementation delivery.62,68 Having highly motivated and committed staff has been reported to facilitate care model delivery and encouraged patients to undertake rehabilitation sessions on a regular basis. 35 However, in other studies, staff reported that rehabilitation sessions were too time consuming and implementing new care elements might adversely affect their private practice. 11 These diverse examples illustrate the importance of engaging with staff and maintaining staff motivation during implementation of new care models.66,69,72
The review found that new care models that were customised to meet the requirements and circumstances of the local setting were shown to have more staff engagement and were noted to have flexible delivery options when implemented in practice.15,16,84 The importance of taking into account the local environment and the needs of all stakeholders is critical in designing the implementation of models of care in rehabilitation. Achieving integrity, feasibility, acceptability, and adherence requires a co-design approach to developing a care model that incorporates patients’ perspectives, staff expertise, and experience in healthcare settings. Evidence shows how co-designed or participatory designs with staff, patients, and stakeholders in different settings can translate evidence into acceptable and feasible solutions. 85 However, the review also found that tailoring interventions or care models to the specific needs of a local context had significant complexities, particularly when attempting to maintain fidelity to the original evidence base. Inconsistencies between the expectations of patients and healthcare professionals were evident regarding patients’ ability and acceptability of the model within the local environment. This highlights the need to be prepared to adapt an intervention or care model while ensuring its effectiveness.50,52,57,58 Furthermore, the participatory method fosters confidence and trust between patients and staff, ensuring the fidelity and sustainability of a care model. 85
Relationships between the facilitators and barriers
Some facilitators and barriers identified in the review had intersecting roles in the implementation of new care models across rehabilitation settings. For example, the implementation process was hindered in some studies due to staff turnover, resulting in staff with little to no experience implementing the care model or new staff trying to learn new implementation skills in a limited time.57,62,64 In other studies, due to staff shortages and extreme workload pressure, clinicians prioritised their regular work rather than implementing the new care model, which they perceived to take additional time.29,31,39,40,50,59,61,71,72 Other facilitators and barriers had dual roles within the studies, operating as both a facilitator and a barrier. For example, the implementation process in some studies were facilitated by prioritising the expertise, knowledge, and abilities of clinicians and staff regarding the care model.11,48,49,55 In other studies, the lack of prior experience and expertise is thought to be a barrier to implementation process.39,57 A similar intersecting pattern emerged between innovation complexity and IT system challenges. In several studies, complex care models were described as difficult to implement and closer examination revealed that the perceived complexity often stemmed from inadequate or malfunctioning IT systems that supported the model.9,31,41,50,55,58,66,67,72,77 Conversely, when IT systems were well-integrated and aligned with the new care model, the innovation was perceived as more intuitive and manageable.28,44,56,58,68,70
Implications of the review
This review identified that although the type of care model, health condition, and care setting may differ, similar factors can enable or hinder the implementation of new care models in rehabilitation. The review also highlighted the intersecting nature of factors and that some factors that might work as facilitators in one domain and barriers in another domain. The review has shown that planning for implementation and tailoring implementation strategies to suit the context are crucial for successful implementation. Studies that had complex care models, inadequate implementation planning, high staff turnover, poor communication, and that were not adequately resourced had limited success with implementation.86,87 Care models should be designed according to the local context and in a user-friendly manner. Access to knowledge and information about the care model should be available both to the implementation providers and recipients.
Any organisation considering implementing a new care model in rehabilitation should prioritise the development of a supportive organisational culture that promotes teamwork, collaboration, and ensure there is committed support from organisation leaders and staff. Arranging practical training sessions for staff to demonstrate model elements, and continuous monitoring with regular feedback can all facilitate a positive teamwork environment and improve staff confidence in care model delivery.11,35,45
Strengths and limitations
The review strengths include a comprehensive search strategy involving six databases with a medical librarian involved in the development of key search terms. The PRISMA guidelines were followed, and multiple reviewers were involved in study selection, data extraction and the narrative synthesis. Any disagreement was discussed among the reviewers and resolved by mutual consensus. As to limitations, the search strategy did not include grey literature or articles published in languages other than English. The review excluded studies reporting on the implementation of virtual care models or telerehabilitation, which may have resulted in additional information on facilitators and barriers being overlooked. The facilitators and barriers identified were those reported by study authors, yet the classification of factors using the CFIR was subjective. Potential links between the facilitators and barriers are unknown.
In conclusion, this review highlights the importance of planning when implementing new models of care in rehabilitation to harness facilitators and to address potential barriers prior to implementing new models of rehabilitation care in a real-world environment. The facilitators and barriers to implementation identified by the review can be used to aid the optimal design and implementation of new models of care in rehabilitation.
Supplemental material
Supplemental material - Facilitators and barriers to implementing new models of care for patients in a rehabilitation care setting: A systematic review
Supplemental material for Facilitators and barriers to implementing new models of care for patients in a rehabilitation care setting: A systematic review by Nabila Binte Haque, Reidar P Lystad, Jeffrey Braithwaite and Rebecca J Mitchell in Journal of Health Services Research & Policy
Footnotes
Acknowledgements
The authors thank Mr Jeremy Cullis, librarian at Macquarie University for his contribution to literature search terminology.
Ethical consideration
Not applicable, as this is a review of the literature.
Author contributions
Nabila Binte Haque: Methodology, Investigation, Visualization, Writing - Original Draft, Writing - Reviewing and Editing; Reidar P Lystad: Conceptualization, Methodology, Investigation, Writing - Reviewing and Editing, Visualization, Supervision; Jeffrey Braithwaite: Writing - Reviewing and Editing, Supervision; Rebecca J. Mitchell: Conceptualization, Methodology, Investigation, Writing - Reviewing and Editing, Supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a grant from the NSW Ministry of Health and a Macquarie University international research excellence scholarship (iMQRES).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analysed during this study are included in this published article [and its supplementary information files].
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.