
Abstract
In this article, I draw on my fieldwork creating protein models of hepatitis B at a biotech laboratory to think through how to approach the body and disease from ontological and phenomenological perspectives. I subsequently draw on Mariella Pandolfi’s work on how bodies can be made to suffer history and Paul Farmer’s work on global tuberculosis disparities to explore ways of analysing embodied activity as a means of identifying and clinically addressing enactments of social inequality and disease. I also introduce Merleau-Ponty’s phenomenological concept of ‘flesh’ as a conceptual heuristic that allows us to understand the meaningful structuring of ontological worlds beyond our own. As I argue, bringing these perspectives together not only allows us to re-envision what an effective disease treatment should be in diverse medical contexts, but also how to better understand health disparities and the nature of disease itself.
Paying attention to the practices through which disease is enacted in different contexts – and especially recognizing how humans suffer history and social inequality – holds significant potential for better understanding and ultimately treating persistent health disparities. Doing so, however, requires that we trace how disease is multiplied as it emerges in different practical contexts. In other words, it requires an ontological approach to investigate how various materialities, histories, and practices enact diseases and bring them into being. Yet this leaves us with the problem of reconciling how these different, localised disease ontologies can hang together as they emerge in divergent situations – a task that is particularly important when trying to develop effective treatments and interventions across different contexts.
To address this issue in both a conceptual and practical way, I will draw on my own work creating protein models of hepatitis B at a biotech laboratory, alongside Mariella Pandolfi’s insights on how bodies can be made to suffer history and Paul Farmer’s work on global tuberculosis disparities. Through exploring these different ethnographic contexts together, I will show how a focus on embodied activity can help to not only identify the emergence of different forms of a disease within different contexts, but also simultaneously create a technique of reconciling these particular instantiations towards a more fundamental understanding of disease.
Given that phenomenology and ontology are both distinct philosophical traditions with their own particular histories, however, it will ultimately be necessary for me to map out a terrain of affinity between the two. It is because these two traditions are harmonious on key issues about the relationship of bodies to the world that we can take insights gained from one method and make them speak to the other. To facilitate this synthesis, I will introduce Merleau-Ponty’s concept of flesh. As I shall argue, flesh is a powerful conceptual heuristic that reveals the always-already belonging of human bodies to material, social, and historical environments as our fundamental style of being. It is the condition of possibility for ontological enactment in all of its multiple forms, and is therefore a concept that allows us to bring together disease ontologies that have become multiplied in different contexts and find a principle that organises them together.
Importantly, in the kind of theoretical landscape that I am exploring here, the usual disease / illness distinction no longer seems to fit. This distinction, in use within medical anthropology since the late 1970s (Eisenberg, 1977; Kleinman, 1980) and still employed by many prominent social scientists and phenomenologists (cf. Leder, 2016), understands illness as the subjective and social experience of suffering that differs from the biological or pathological reality of a disease. As I will show, however, this distinction is no longer empirically tenable from ontological or phenomenological perspectives. The so-called ‘real’ biological and molecular materiality of diseases is always-already articulated and shaped by the convergence and coordination of research techniques, clinical interventions, medicines, history, sociocultural environments, and patient experiences.
Bringing ontological and phenomenological theories together to understand disease in specific medical settings will therefore necessitate that we redefine the very notion of what disease might be, expanding our understanding of disease towards a more holistic term that not only encompasses both halves of the previous distinction between illness and disease, but also reflects the always-already connectedness between bodies, pathogens, and the larger world. Perhaps most importantly, doing so will also require that we ultimately adjust our understanding of disease treatments and interventions to reflect the emergent – as opposed to pre-given – reality of disease in any given context.
Embodying Hepatitis B Proteins
Let me begin with the concrete. Over the course of several months, I worked as a computational protein modelling researcher at a biotech laboratory in the US, which I will call laboratory Q. While at laboratory Q, I had access to the maze of laboratory spaces and offices within the building, and I also had an office – a large, windowless room with spare computer monitors, cables, and hard drives stacked in huge disorderly piles on the floor and desks. On one of these desks was a space – cleared out of the tangled mess of computer fragments as if it had been carved out of a mound of sand – where a rather large Linux-powered computer was stationed. I spent my days at this computer completing literature research on the latest protein homology modelling techniques, and building my own computer models of hepatitis B polymerase proteins. In particular, our team at laboratory Q was focused on building an in silico (computer-based) computational model of the hepatitis B polymerase protein both for the sake of better understanding the structure of hepatitis B proteins, and as a tool for drug discovery. Our primary goal was to use our digital hepatitis B models to conduct high-throughput in silico screenings of the entire library of 85,000 drug candidate compounds at laboratory Q, and from these screenings we would produce a small list of compounds that might be the best candidates for new hepatitis B drugs based on their ability to form optimal chemical bonds with target molecules in the hepatitis B polymerase.
Making molecular models has been a constitutive practice of modern chemistry and biology since the 1860s (de Chadarevian and Hopwood, 2004), and has been given new importance and emphasis in the age of computational biology and proteomics, where researchers turn to the interactive elements of molecular models in order to get a ‘feeling’ for a molecule or protein in a way that research focused on genetic or amino acid codes simply cannot provide (Myers, 2008). In her fascinating work on these molecular embodiments, Natasha Myers (2006, 2008, 2009, 2015) describes how the process of in silico protein modelling deeply engages the tactile and physical world of the modeller. Through this process, the researcher comes to embody the protein or molecule under investigation, gaining a bodily intuition for the way it conforms (arranges itself in three-dimensional space) and behaves.
Throughout the course of daily conversations with my supervisor at laboratory Q, whom I have named Dr Klein for discussions in this article, I began to notice these kinds of molecular embodiments reflected in the ways that he would approach problems, talk about and perform molecular bonds with animated gestures, and interact with molecular models on our computer screens. In particular, I began to notice how Dr Klein would employ his embodied intuition for the shapes and behaviour of proteins in order to interpret the raw output from the screenings we were conducting with our models. At the point when we had finally completed building our model of the hepatitis B polymerase and had run all of our drug candidate molecules through several rounds of high-throughput screenings, Dr Klein sat down with me to sift through and choose the optimal poses (i.e., the specific angle and position of the drug compound while bonded to the target protein) produced by the software for each compound that showed a promising binding affinity. Using the computer mouse as an extension of his hand, Dr Klein would grasp the drug molecule bound to the hepatitis B protein (Figure 1), continuously rotating and examining it from all angles. Switching back and forth between different visual representations of the virus protein and drug compounds, Dr Klein would then spin the drug molecule around in front of him with his hand to see how it fitted within the open pockets of the virus protein.
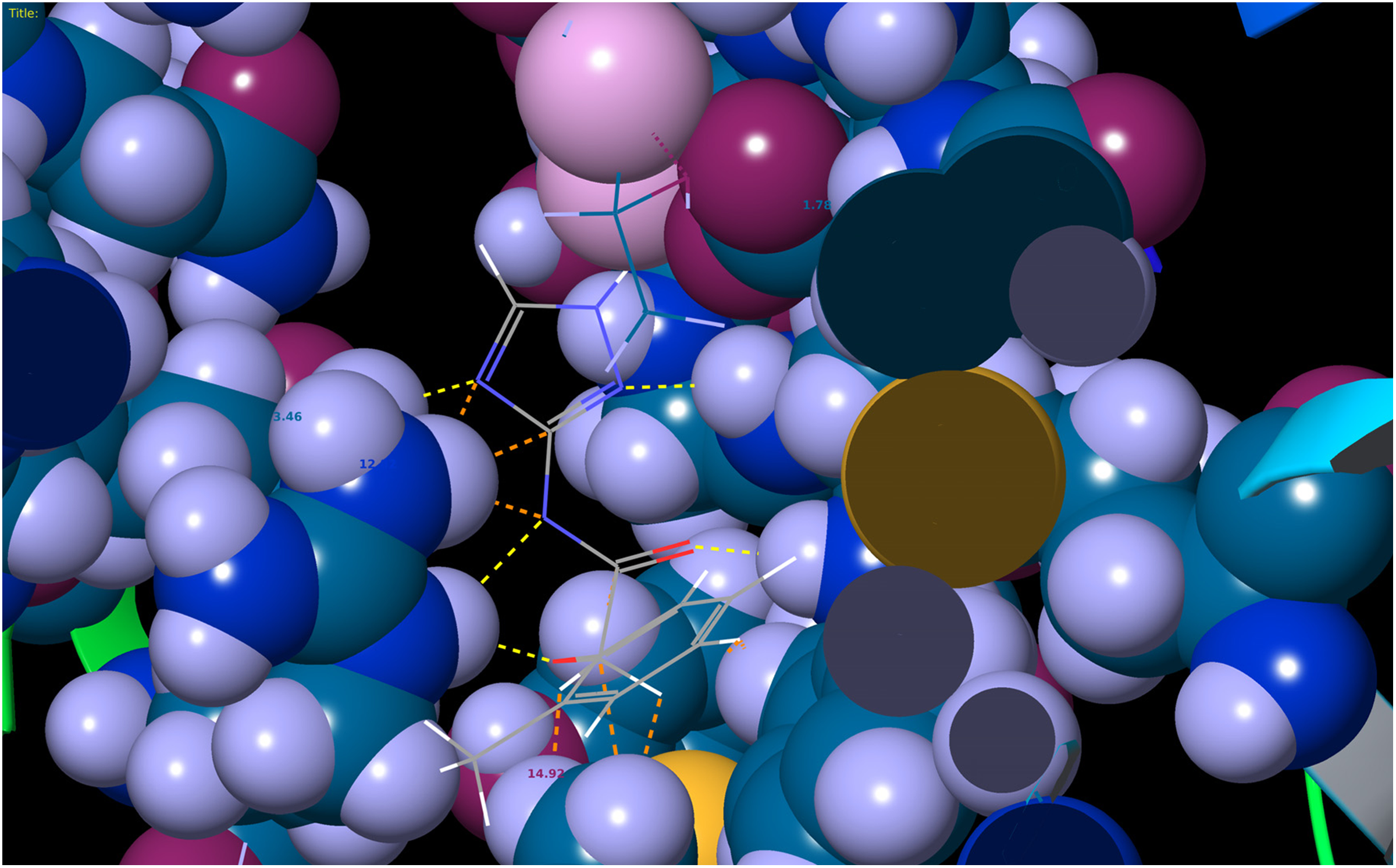
Screenshot of a drug candidate compound bound to an in silico model made at laboratory Q of the hepatitis B reverse transcriptase protein (a sub-domain of the polymerase). Coloured dotted lines indicate different types of chemical bonds.
In fact, even outside of interpreting these binding studies, every time Dr Klein saw a new molecule or protein on a computer screen, he would manipulate it and interact with it in this way, grasping it in his hand so that he could grasp it in his mind. He almost never had anything to say about a protein or a molecule until he had spent several minutes with it in this way. Simply seeing an image of a drug molecule bound to a protein wouldn’t give him the information he desired – he needed to take it up interactively with his body from many perspectives in order to draw upon his embodied intuition of chemical bonds and protein folds to make sense of what he was seeing. Through physical manipulation and interaction with our computer models in this way, the proteins and molecules began to take up the voluminosity of Dr Klein’s body itself. These kinds of molecular and protein embodiments, it turned out, would be key to the ontological enactment of a certain form of hepatitis B in our laboratory setting.
Thinking Ontologically
Although ontology has historically been used in the field of philosophy to designate a concern with the existence of things and the essence of being, recourse to ontology specifically in anthropology and science and technology studies (STS) has instead often led to a focus on objects and materiality. Ontological investigations in anthropology and STS have thus tended to fall much more in line with the so-called ‘object-oriented ontology’ expounded by Graham Harman (2002) or the actor-network theory of Bruno Latour (2005), in that they are usually heralded as a return to objects, things, and materiality. Importantly, ontological investigations in anthropology and STS also tend to return human experience itself to the level of an object within an emergent landscape of other bodies, diseases, technologies, processes, and mundane objects. Whether from the perspective of ‘enactment’ (Mol, 2002), ‘ontological choreography’ (Cussins, 1996; Thompson, 2005), ‘deployment’ (Latour, 2005), or a variety of other terms used in anthropology and STS, the salient insight of ontological theory has been that objects and bodies are brought into being through practice, and that this process is no less than world-making: ‘“materiality”…needs to be understood as the contingent upshot of practices, rather than a bedrock reality to be illuminated by an ontological investigation’ (Woolgar and Lezaun, 2013: 326).
In The Body Multiple (2002), Annemarie Mol speaks of atherosclerosis as enacted by different practices, and describes how these interactions and practices are what bring the disease into being. She gives the example of Mrs Tilstra, who has pain in her calf after walking her dog. Although this phenomenon goes by the medical name ‘intermittent claudication’, the disease isn’t enacted until she visits the doctor. It requires both a patient who worries about something and a doctor who attends to it. But this enactment extends beyond pure human interaction as well, as the desk, the chairs, the [referring] general practitioner, the letter [of referral]: they all participate in the events that together ‘do’ intermittent claudication. As does Mrs. Tilstra’s dog, without whom she might not even have tried to walk more than the fifty meters after which her leg started to hurt. (Mol, 2002: 23)
Mol (2002) also speaks of how atherosclerosis can be enacted and multiplied in mutually exclusive ways – a process that John Law (2004) has called ‘ontological interference’. In the pathology lab, cross-sections of vessels are made from amputated legs, but obviously no pulse can be taken or questions asked of the patient. On the contrary, in the outpatient clinic a patient can be asked questions and have a pulse taken, but cross-sections of blood vessels cannot be made from the intact legs of patients. These practices of enacting atherosclerosis in the clinic and atherosclerosis in the pathology lab exclude one another. They cannot be realised simultaneously, and this incommensurability is a practical matter.
A distinctive quality of this sort of ontological account – indeed one of its greatest strengths – is its ability to ‘multiply the range of entities that can be shown to exert an active, mediating force in the transformation of a certain state of affairs’ (Lezaun, 2017: 309). Actor-network theory (ANT) is exemplary in this regard. In ANT, as in all of the approaches outlined in this section, the investigation begins from following action and practical activity. It is an approach, furthermore, committed to refusing an ontological privilege of human over non-human actors. An actor, in this case, ‘is not the source of an action but the moving target of a vast array of entities swarming toward it’ (Latour, 2005: 46). Any object, in fact, might be an actor so long as it has an effect on another object. In this regard, ANT produces a so-called ‘flat ontology’, to use Manuel DeLanda’s (2002) term, where objects and actors in the world cannot be reduced to certain immutable ontological categories such as human, nature, society, or species. Instead, such designations only come after the fact, as characteristics of the emergent associations between different objects.
As Latour further notes, ‘when we speak of actor we should always add the large network of attachments making it act’ (2005: 217–18). Thus, the hybrid term ‘actor-network’ that ANT deploys. An actor-network itself, however, ‘is an ontological definition and not a piece of inert matter in the hands of others’ (Latour, 1996: 374). As Latour emphasises, the task of ANT is to deploy these actor-networks. Such deployment is not mere description. Rather, deployment is a conceptual heuristic through which ‘the number of actors might be increased; the range of agencies making the actors act might be expanded…and the controversies about matters of concern might be mapped’ (Latour, 2005: 138). To use Martin Holbraad and Morten Axel Pedersen’s (2017) terms, thinking ontologically in anthropology is a ‘technique’ of ethnographic description. It is a method of empirically looking at the convergence of bodies, objects, the world, and history, and then mapping the ways in which they associate together as actors in a given situation to enact new, emergent forms. Thus, to return to our above examples with refined terminology, we might say that Annemarie Mol deploys dyes, microscopes, technicians, and Mrs Tilstra’s dog in The Body Multiple to demonstrate how emergent forms of atherosclerosis are brought into being.
Enacting Hepatitis B
In deploying my own ethnographic encounters at laboratory Q, I would like to offer that the molecular objects to which the researchers at laboratory Q were becoming habituated were not merely representations of hepatitis B proteins, but in a certain way enacted qualities of the virus proteins themselves. This is because comparing molecular models to the ‘real’ thing is a distinction that doesn’t actually hold up in practice. It is often only through the material work of making a virus protein coherently visible and gaining an embodied understanding of its forms and shapes through models that what we might call the ‘real’ or ‘actual’ viral protein can become a ‘molecular object’ to be studied or understood (Lynch, 1991). In the case of our hepatitis B research, one of the primary ways that researchers come to know what hepatitis B is and how to treat it is through their models, and the disease medium that they then use to conduct preliminary drug research is not the ‘real’ biological virus, but rather these in silico models. For this reason, Eric Francoeur sees the realm of ‘real’ molecular structures as ‘essentially cultural’, in that it is ‘coextensive with the means chemists have given themselves to show, talk about, and work with these structures’ (2000: 66).
This underscores why we cannot take disease proteins or molecules as entities that exist abstractly as things in themselves somewhere out in the world. Rather, the ontological modes through which viruses are brought into being are the various embodied practices that allow us to experience them, give shape to them, research them, and understand them. Molecular models don’t signify an absolute and abstract molecular referent – they don’t speak to some ‘truth’ about molecules and viruses behind their representation. Instead, molecular models enact viruses themselves as phenomena through interactive production and use. Similar to Annemarie Mol’s (2002) discussion of atherosclerosis, however, the enactment of the hepatitis B virus through this kind of in silico modelling entails its own particularities and exclusions. Specifically, it reinforces the discrete, stand-alone quality of proteins and viruses and works to enact them in a way that excludes human host environments and larger socioeconomic environments as integral to the functioning and treatment of these viruses.
The specific aim in using our models at laboratory Q was to develop a new nucleos(t)ide analogue drug for hepatitis B, which is a class of drugs that works through binding to known molecular targets within the viral polymerase and inhibiting viral replication. Most of the major drugs on the market for hepatitis B are nucleos(t)ide analogues, including tenofovir, adefovir, and entecavir. Yet this strategy towards drug discovery (termed ‘rational drug design’) reveals the gravity and pervasiveness of the disease-as-virus hepatitis B ontology that I’ve just mentioned. It is a pursuit that rests upon a certain ontological condition of possibility – namely that virus proteins and molecules can be targeted and interacted with at a discrete, molecular level. It requires that hepatitis B itself exists fundamentally at the level of the virus protein as a discrete entity that can be separated from the world.
Through the work of building these protein models with Dr Klein, I began to realise that this ontology of discrete proteins and viruses is built into the very embodied intuition for the shapes and forms of proteins that researchers acquire through using models. Looking at and interacting with these models of the hepatitis B polymerase protein day in and day out – a brightly coloured assemblage of atoms sitting alone against the deep black background of the computer display – one is interacting with a protein or a molecule that is discrete, self-contained, and alone (Figure 2). This particular ontology of proteins and viruses is the primary foundation upon which rational drug design of the kind that we carried out at laboratory Q is made possible. But, importantly, this ontology is acquired, enacted, and perpetuated through the embodied intuition for the discrete and individual forms of proteins that researchers acquire through modelling. This will be our starting point for discussing embodied activity.

Screenshot of an in silico model made at laboratory Q of the hepatitis B reverse transcriptase protein bound to DNA.
Thinking with Phenomenology and Embodiment
Before delving further, however, I would like to take the space to refine some of the ideas about phenomenology and embodiment that I’ve introduced above. First and foremost, it is paramount to emphasise that phenomenology refuses the dual ontological categories proposed by Immanuel Kant in his Critique of Pure Reason (1998 [1781]) of the thing in itself, which is something that exists without the use of the senses, and the phenomenon, which is something that only appears and exists through our sensory perception. Instead, phenomenological theory posits the always-already relation of perceiving bodies to objects and the world. Maurice Merleau-Ponty characterises this in several ways in the Phenomenology of Perception (2012 [1945]). As he writes, ‘the subject that I am, understood concretely, is inseparable from this particular body and from this particular world. The ontological world and the body that we uncover at the core of the subject are not the world and the body as ideas [i.e., things in themselves]’ (2012 [1945]: 431). In another passage, he notes, ‘my body is the pivot of the world…and in this sense I am conscious of the world by means of my body’ (2012 [1945]: 84).
Merleau-Ponty further notes that: insofar as I inhabit a ‘physical world’, where consistent ‘stimuli’ and typical situations are discovered…my life is made up of rhythms that do not have their reason in what I have chosen to be, but rather have their condition in the banal milieu that surrounds me. (2012 [1945]: 86) it is not the case that man ‘is’ and then has, by way of an extra, a relationship-of-Being towards the ‘world’ – a world with which he provides himself occasionally. Dasein is never ‘proximally’ an entity which is, so to speak, free from Being-in, but which sometimes has the inclination to take up a ‘relationship’ towards the world. (2010 [1927]: 84)
Hence the term that Heidegger uses for being – Dasein, translated as ‘there-being’ – which posits an inherent positionality, valence, and worldly involvement to being and to bodies.
Here we can already see parallels emerging between the ontological ideas discussed above and phenomenology. But the unique insight that phenomenological theory contributes is that understanding the enactment of bodies, objects, and worlds must begin with ‘the experience of perceiving in all its richness and indeterminacy, because in fact we do not have any objects prior to perception’ (Csordas, 1990: 9). Objects only arise as a secondary result of reflective thinking, but on the pre-objective level of perception ‘we have no objects, we are simply in the world’ (Csordas, 1990: 9). This perception, importantly, ‘is always embedded in a cultural world, such that the pre-objective in no way implies a pre-cultural’ (Csordas, 1993: 137). Only by looking to embodied experience can we thus begin to unravel how bodies, objects, and worlds are entangled.
Suffering History
One strong example of applying this kind of phenomenological perspective towards understanding disease can be found in Mariella Pandolfi’s (2007) ethnographic work on illness and memory among women in southern Italy. In Pandolfi’s ethnography, if women: want to talk about the village, or about family events, past and present, they begin by narrating the troubles in their own bodies…and delineate new narrative grammar that transposes the historical extraordinary event into the body’s extraordinary event. (2007: 454)
Although Pandolfi is interested in narratives about the body, she investigates these from a phenomenological perspective instead of a semantic one. That is, instead of starting with the body as an object whose reflective capacity for thinking about its biological symptoms is symbolically mediated by culture, Pandolfi discusses how environments and history have sedimented themselves within the body on the pre-objective level over time, and therefore how history manifests itself upon the body in a way that confounds the usual boundary between feeling well and ill. As she notes: narrative seems full of symptoms and pathology, but it should rather be understood as the narrative of a body permeated by age-old suffering. Examples of symptomatologic discourse: ‘My legs feel heavy, my heart is bursting, I never sleep, my liver has gone to my brain.’ ‘My hands are shriveling up, my eyes hurt, my heart has seen things that made it shrink so small it never beats.’ ‘My blood has dried up, my blood has withdrawn and I no longer breathe as my blood has turned to water and I’ve lost the strength of my arms.’ (2007: 456)
In this particular case, the bodily experience of these women is not so much a matter of suffering disease, but it is ‘the story of how each woman suffers history’ (2007: 457). The body can be made to suffer from the way it is positioned towards behavioural, social, technological, and historical milieus, and these can all act together with a specific pathology towards enacting a disease. This brings us far beyond a purely biologically deterministic way of understanding disease, while still allowing us to understand how physiological states themselves are crucial to the embodied experience of disease. It speaks directly to the thickness and ambiguity of our own embodied experience, which is a result of our body’s relation to a cultural and historical world. This relation in turn influences how we ‘attend to and with’ the body in specific circumstances (Csordas, 1993). As Mariella Pandolfi notes, ‘a subject’s relationship with a symptom or illness always has a precise valence’ (2007: 457).
Flesh as Our Fundamental Style of Being
In drawing upon insights from my work at laboratory Q and Mariella Pandolfi’s ethnography, there are several concepts specific to Merleau-Ponty’s phenomenology that we can explore to deepen our understanding of embodiment and ontological enactment. The first concept to draw out has to do with the body and history. Merleau-Ponty writes in the Phenomenology of Perception (2012 [1945]) that there is an essential ambiguity in the way that the body is experienced, and this is largely due to the role of history in creating a habitual body in tension with our actual body. Through their relation to the world, our bodies acquire certain techniques of being and habits, but as these techniques are acquired and mastered they recede into the horizon of our awareness and are sedimented into our body schema as a habitual body. As Emmanuel de Saint Aubert explains, this body schema is the ‘intersensory and intercorporeal organization of our life, the axis of the unity of our being and of our relation to other beings’ (2009: 32). To habituate ourselves to objects through this body schema is ‘to make them participate within the voluminosity of one’s own body’ (Merleau-Ponty, 2012 [1945]: 145) in such a way that it enlarges our very perception and experience of bodily space and possibility. Acquiring habits in this way becomes a continuous ‘reworking and renewal of the body schema’ (Merleau-Ponty, 2012 [1945]: 143) where ‘the body knows and is known little by little, by annexing new territories’ (de Saint Aubert, 2009: 38).
Yet our embodied activity is both informed by this body schema and perpetually escapes it. In this way, embodied activity ‘takes up habitual schemas and deploys them, in situ, with competence and skill’ (Crossley, 1996: 101). The ambiguity that Merleau-Ponty speaks of then is of a body that is shaped by history (and therefore, by extension, its cultural and historical milieu), yet also one that must continuously ‘adjust to the “sense” of the situation’ and ‘express our orientation toward a “behavioral milieu”’ (2012 [1945]: 81). History, in Merleau-Ponty’s account, is therefore ‘neither a perpetual novelty nor a perpetual repetition, but rather the unique movement that both creates stable forms and shatters them’ (2012 [1945]: 90). In the same way that Merleau-Ponty’s phenomenology collapses the distinction between subject and object, it also collapses the past into the present. As Françoise Dastur notes in her interpretation of Merleau-Ponty, ‘the past, then, is no longer a modification of the present of consciousness, as in memory. Rather, it is “simultaneous” with the present; the present is constantly prolonged in retention, and retention gives to the present its “thickness”’ (2000: 43).
This thickness becomes the focus of Merleau-Ponty’s investigation into what he calls flesh in his later works. To be clear, flesh does not reduce to actual matter. It is the thickness and openness between bodies and the world, a formative element of subjects and objects that, as an incarnate principle, gives them a certain style of being. It is a texture ‘between the seer and the thing’ (Merleau-Ponty, 1968 [1964]: 135) which, by virtue of the similitude it gives them, is their means of communication. We may therefore think of flesh as referring to a generality of being, to use Merleau-Ponty’s term. If indeed embodied activity is characterised by a continuous reworking of our body schema through the envelopment of the body into the world, then this points us to a more general notion of being, or flesh, which refers to the always-already enveloping of the world into our bodies and our bodies into the world as our most fundamental and common style of being. As Merleau-Ponty writes, ‘there is an indivision of my body, of my body and the world, of my body and other bodies, and of other bodies between them’ (2003 [1995] : 279). In short, flesh is a ‘fabric common to all beings and the principle of indivision, and, as such, it is the name of being as a whole’ (Dastur, 2000: 37).
When observing how the world and historical experiences shape different bodies in different instantiations, however, the notion of flesh gives us a conceptual way to still understand how these relate to each other and are organised under a more fundamental style of being. This is why the notion of flesh will ultimately be so important for making sense of ontological enactment. It is also by virtue of this common texture of flesh between them that individual bodies can still feel into (Einfühlung) other bodies such that they might be considered ‘organs of one single intercorporeality’ (Merleau-Ponty, 1964 [1960]: 168). As Merleau-Ponty writes, ‘the body proper is a premonition of the other person, the Einfühlung an echo of incarnation’ (1964 [1960]: 175). Thus, understanding flesh reveals what de Saint Aubert has called an ‘intercorporeal schema’ (2009), which not only envelops our bodies into the bodies of others and the ‘flesh of the world’, to again use one of Merleau-Ponty’s phrases, but also more concretely envelops our bodies into the flesh of other objects, technologies, history, and sociocultural environments.
Whereas earlier in the Phenomenology of Perception, Merleau-Ponty posits the pre-objective unison of bodies and the world, he later uses flesh to explain that the belonging of one to the other is our fundamental style of being. It is an organising principle that might unify the diverse experiences of being that different individuals have, and as such is a vantage point through which we can begin to make sense of ontological enactment and ontologies of scale between different contexts.
New Directions in the Phenomenology of Disease
As Mariella Pandolfi’s ethnographic work shows, in addition to revealing how certain disease ontologies are enacted, one of the key conceptual strengths of a focus on embodiment is that it can help shatter norms about the ontological nature of the body and give us insight into the flesh of disease. Taking such an approach, however, will also require a new take on the phenomenology of disease that diverges from dominant theories in the field.
In Fredrik Svenaeus’ seminal work, The Hermeneutics of Medicine and the Phenomenology of Health (2000), we see Heidegger’s phenomenology used to characterise illness as an ‘unhomelike being-in-the-world’ where there is a lack of rhythm and balance in one’s body. Drew Leder, in his masterfully written The Absent Body (1990), develops a similar line of reasoning that I would like to explore more deeply here as a counterpoint to my own approach. In this work, Leder engages in a phenomenological exploration of how our bodily habits, techniques, and sensations disappear from our attention once they are mastered. ‘When functioning well’, he writes, the ‘body is a transparency through which we engage the world’ (1990: 82). During times of disease, however, he observes that the body is again brought to the fore of our attention as a dysfunctional and alien presence. This he labels dys-appearance, which refers to the ‘thematization of the body which accompanies dysfunction and problematic states’ (Leder, 1990: 86). Leder then uses this phenomenological understanding to characterise disease itself: ‘disease, even more than pain, is typified by complex patterns of dysfunction…. In disease, one is actively dis-abled’ (1990: 81).
Leder further notes that he does not think it would be appropriate to subsume ageing, puberty, menstruation, or pregnancy within the idea of dys-appearance. Although any of these experiences might entail intense physical and bodily change that would bring our bodies back to the foreground of our awareness, Leder notes that these experiences: are a normal and necessary part of the life cycle. They are not in themselves dysfunctional or alienating. As such, they should not be associated with the notions of ‘bad’ or ‘ill’ that comprise part of the Greek meaning of dys. (1990: 89)
My divergence from Leder’s view is that seeing disease as the case of a dysfunctioning body is too caught up in the normative, medicalised way of understanding disease in relation to certain biological norms about the body. A more appropriate phenomenological perspective on disease would move beyond seeing a dysfunctioning body in relation to certain ontological bodily norms, and instead remind us that disease is merely a case of our bodies persisting with a certain style of being, or flesh, precisely as they always have. Disease is not a divergence from or a dysfunctional state of our being-in-the-world, but rather an exemplification of this being-in-the-world. This is a move towards seeing bodies as processes that are defined by their openness and connectedness to the world around them, which inevitably includes a number of disease pathogens and other factors that contribute to disease. In taking this view, however, it is also important to remember the thickness of our bodily flesh, wherein bodies are not only made to suffer from their openness to disease pathogens and current material environments, but made to suffer from social and intercorporeal relationships, and suffer history.
Thickness // Phenomenology and Ontology
Hopefully we can now see how investigating embodied experience allows us to understand the deep connection between bodies and worlds, and thus gives us a route into observing the enactment of multiple bodies and diseases. The disjunctions between these multiple ontological worlds, furthermore, can only be reconciled and understood in relation to one another through an understanding of flesh and intercorporeality (Csordas, 2008). As I shall argue here, these two approaches overlap in five key ways that allow for the transfer of insights about the body or disease from one to the other.
The Relationship between Subjects and Objects / the World
Bruno Latour, in We Have Never Been Modern (1993), shows how a growing distance between subjects and objects is a myth of modernity that never plays out in practice. Indeed, any acknowledgement of enactment is an acceptance of the inseparability of subjects and objects, and the so-called ‘flat ontology’ of ANT reflects such a refusal to discriminate between human and non-human actors – or subjects and objects – in this way. Annemarie Mol also maintains that the practice-oriented focus of ontology reveals that ‘to be is to be related…a sentence that tells about what atherosclerosis is, is to be supplemented with another one that reveals where this is the case’ (2002: 54). For ontology, the relationship of objects to the world is never pre-given, but enacted through practice.
In phenomenology, I have noted that there is a collapse or enveloping of subjects and objects into one another, and furthermore that the relationship of embodied experience to the world is also never pre-given because of the constant enveloping-enveloped relationship between bodies and the world through flesh. In the phenomenology that I’ve been describing, the pre-objective unison of subjects and objects through embodied activity also demands a flat ontology precisely because all being is non-hierarchically characterised first and foremost by this openness between bodies, objects, and the world. This is why, from the perspective of both phenomenological and ontological theory, those who are sick should not have a special or dysfunctional ontological status – they are merely persisting as they always have in relation to the world.
The Unfinished Character of the World
Steve Woolgar and Javier Lezaun note that, ‘investigating the composition of ontological realities would thus be a way of challenging any presumption of order or completion in the world’ (2013: 323). Acknowledging the enactment of bodies and diseases presupposes a commitment to understanding how realities are multiple and how the world can always be reconfigured. Yet phenomenology stresses this same always-unfinished character of the world through the thickness of flesh and the tensions between our habit body and the actual body. Indeed, embodied activity is a perpetual re-negotiation and transfiguration of this relationship.
Out of Cultural Relativism and into ‘Disease Itself’
Both ontology and phenomenology share a common commitment to overcoming approaches that would construct a division between the social or cultural experiences of illness on the one hand, and the biological or physiological reality of disease on the other. Instead, both give us a perspective into ‘disease itself’ (Mol, 2002: 13), and share a commitment to understanding the co-production of the social and the biological (Lock, 1993; Lock and Nguyen, 2010). Understanding the ontology of disease takes us away from dealing with varying cultural representations of a stable, universal, and biologically determined disease. Instead, by foregrounding practicalities, materialities, and events, ‘disease becomes a part of what is done in practice’ (Mol, 2002: 13).
Yet one of the greatest strengths of a phenomenologically grounded perspective on health is that it also allows us to move beyond investigating mere subjective representations of biological disease through the model of illness, towards looking at how social, cultural, and historical processes are embodied within the very biological and physiological nature of disease itself. That is, both ontology and phenomenology avoid any sense of biological determinism, while simultaneously allowing for a serious treatment of the concrete, biological dimensions of the human body and disease.
An Open Notion of the Body / Materiality
When looking at how bodies and diseases are enacted, or how our bodies are connected with cultural and historical processes on the pre-objective level, it no longer makes sense to talk about bodies as entities that can be reduced down to physiological or biological processes. Instead, bodies become both organic and inorganic, living and non-living, material and immaterial. To use Lisa Blackman’s term, bodies become ‘im/material’ (2012). Both phenomenology and ontology allow us to move beyond biological determinism when understanding disease because at their heart they are systems of thought that conceptualise bodies not as closed physiological or biological systems, but rather as open processes ‘which extend into and are immersed in worlds’ (Blackman, 2012: 1). Bodies are defined by their very ability to be open to, connected with, and affected by the world around them, and this relationship occurs at ‘every level and scale of matter, from the subatomic to the cultural’ (Blackman, 2012: 5).
Once we make this move, however, the various mundane objects with which ontology occupies itself must also be seen as im/material since they are co-produced with human relations and social processes. This is perhaps more obvious in phenomenology, where the very insistence that material objects exist only as phenomena means that human, social, and im/material processes are fundamental to their being.
The Power to Observe Multiple Worlds
Importantly, thinking ontologically in the way that I’ve outlined here allows anthropologists to take the truth claims that their informants make about the material and biological world seriously, as it opens up the possibility of a plurality of worlds with varying, emergent relations within each. For phenomenology as well, if we begin with the constitutive power of the world, then an acknowledgement of ever-changing embodied activity is also an acknowledgement of ever-changing, multiple worlds. Indeed, from a phenomenological point of view, the world can never be the same from one moment to the next.
However, I should note Morten Axel Pedersen’s (2012) anthropological critique that ontology simply replaces the problem of synthesizing multiple worldviews with the problem of trying to understand relationships between different people inhabiting different worlds that might remain to us incomprehensible or incommensurable. To overcome this limitation, we should remember that if ontology perhaps multiplies worlds, then through paying attention to embodied activity we realise that these multiple worlds are still united by a common mode or style of being – namely flesh – that is the condition of possibility for enactment in all of these worlds. Practically, then, ontology needs phenomenology, as it is only through investigating embodied experience that we can begin to understand the meaningful structuring of ontological worlds beyond our own.
Beyond Culture Towards Embodiment and Ontology
One of the important consequences of the theoretical directions that I am pursuing here is that it requires that we revisit and ultimately reformulate the kinds of factors that play a role in health inequality. In public health research, it is common to fall back on a belief in the effectiveness of developed vaccines, screening technologies and protocols, and clinically tested drugs. In the case of hepatitis B, although there is still no cure, there are at least drugs that can reasonably manage hepatitis B with lifelong use. When disparities emerge in infection, screening, or vaccination rates, the factors that are then proposed to be lacking are patient-level beliefs, awareness, education, and compliance, although there is also an increasing focus on provider-level factors. Nonetheless, cultural commitments and social practices are all too often seen as barriers to the success of pharmaceutical and technological innovations.
Such culture-based approaches to health disparities ‘can lead to the mistaken idea that if we can only identify the cultural root of the problem, it can be resolved. The situation is usually much more complicated’ (Kleinman and Benson, 2006: 1675). In other words, there is a danger in ‘conflating structural violence with cultural difference’ (Farmer, 1999: 257), where focusing too heavily on cultural difference as the driver of health disparities and sickness tends to underplay the basic economic and structural factors that bring disease into being in any given context, and which are often more important drivers of health disparities than cultural beliefs or practices (Kleinman and Benson, 2006). As Laurence Kirmayer notes, ‘social inequality itself is a major determinant of health and is configured in ways that reflect local histories that are normalized, justified or rendered invisible through cultural frameworks of identity and commonsense’ (2012: 150).
Instead of beginning from a decontextualised notion of culture and health beliefs to investigate health disparities and inequality, perhaps it might then be more useful to start with a sincere effort to understand those who are sick in their own environmental milieus, their own ‘local moral worlds’ (Kleinman, 1995). These local moral worlds, as Arthur Kleinman has glossed them, are ‘the commitments of social participants in a local world about what is at stake in everyday experience’ (1995: 45). Instead of looking towards cultural commitments, such an approach would be an inquiry into what Sarah Willen (2013) calls existential commitments. This type of phenomenological understanding might be much more useful in imparting a structural competency (Metzl and Hansen, 2014) that could be used to understand how social and structural networks come to bear upon a patient’s health and disease. Through this kind of person-centred, phenomenological inquiry lies a technique to more readily understand how disease might be enacted and multiplied from one context to the next. It is an approach that allows us to see the body and disease as dense points of contact between material, historical, social, and technological environments, all of which come together to give shape to specific bodies and pathologies.
Coordination // Treating Disparities
In laying out the above ethnographic and theoretical discussions, it should hopefully be apparent that treatments and interventions developed to treat a disease enacted in laboratory settings must be of a very different nature from those treatments devised to treat im/material bodies made to suffer from their positions towards physical, behavioural, social, technological, and historical milieus. To articulate this point, and to weave together my arguments into a succinct demonstration of how to use this orientation to better understand and treat health disparities, I’d like to briefly discuss Paul Farmer’s (1999) work on structural violence and tuberculosis (TB) in Haiti. Paul Farmer notes that TB has always disproportionately affected the poor. Between the contexts in which TB antibiotics are developed in the US and the embodied experience of those suffering from TB in Haiti, TB is multiplied. The embodied experience of TB in Haiti is also one of hunger and starvation, opportunistic infection brought on by unclean drinking water, rapid transmission due to close living quarters, and the inability to make frequent trips to the clinic to receive treatment. For years, healthcare workers in Haiti, convinced by the proven laboratory and clinical efficacy of TB antibiotics, would blame the behaviours or cultural commitments of those with TB in rural Haiti for their own sickness if they did not or could not follow treatment prescriptions. From their perspective, it wasn’t that the treatments weren’t working, but that patients weren’t compliant.
Coordinating treatment for TB in an effective way in this setting, however, entails taking what is effective in a clinical trial and augmenting it to address the embodied experience of the disease in a new context. In the case of Farmer’s treatments in Haiti, he was able to bring up compliance and cure rates from 50% to nearly 100% by adding nutritional support to his antibiotic treatments, and by either reimbursing patients for travel to the clinic or having a clinic worker travel to their homes to administer treatment (Farmer, 1999). Through paying attention to the existential commitments of those infected with TB in rural Haiti, Farmer observed that the disease is not only constituted by an infection of TB bacteria, but by experiences of poverty and malnutrition as well. Farmer then designed a treatment that would target the full set of embodied and material relations that constitute having TB in rural Haiti, as opposed to one that might only target the disease-as-bacterium enactment of TB that is tested in clinical settings in the US. When you are treating two different things, of course treatment must vary accordingly.
Conclusion – Redefining Disease
The theories presented here are meant to make us think critically about the nature of a body or disease. Through taking a new approach to using phenomenology in relation to medicine or disease, I have shown how it not only allows us to move away from biological, medicalised norms about the body, but is an expedient way through which we can gain access to seeing the enactment of ontological difference. This is done through recognizing the im/material flesh of the body – showing how culture, socioeconomic structures, and history are part of the very fabric of our biologies and of disease itself, without losing the ability to inquire into the concrete physicality and materiality of both biology and disease. This allows us to take seriously the truth claims made by anthropological others and to find a way to speak well about such alterity – a task that previous symbolic and interpretive schools in anthropology are unable to accomplish because they rely on the foundation of a universal, objective material world upon which cultural and symbolic interpretations are merely laid in a subjective fashion. As Mol puts it: however important feelings and interpretations may be, they are not alone in making up what life is about. Day-to-day reality, the life we live, is also a fleshy affair. A matter of chairs and tables, food and air, machines and blood. Of bodies. (2002: 27, my emphasis)
What I would like to highlight here is that these new understandings hold a productive potential for medical anthropologists and biomedical researchers alike to better understand health inequality and envision more effective medical treatments. The difference is in moving away from seeing a disease fundamentally as the local effects of an enclosed virus, pathogen, tumour, or biological abnormality within human bodies that are then put into relation with larger physical, historical, economic, and sociocultural environments, towards seeing disease as being this very set of relations, of which the virus, pathogen, or tumour itself is only a part. As a humanistic discipline, perhaps anthropology can employ new ways of looking that can reinstate this complexity. We have to recognise that thinking of disease as being transmitted within certain viruses or pathogens does not reflect an objective truth about what a disease is, but rather reflects a certain way of enacting and understanding disease pathogens as a result of so many cultural, technical, and embodied scientific and biopolitical practices. When we shift our focus to this new way of looking, then good care and good treatments, as a matter of methodological and ontological necessity, must involve tempering treatments with ways to address social and historical suffering.
Footnotes
Acknowledgements
A sincere thanks to Javier Lezaun for his insightful comments on several drafts of this article, and for the many thoughtful discussions that helped shape my understanding of and interest in ontological theory. Thanks also to Elisabeth Hsu for nurturing my interest in phenomenology, and for the initial encouragement to pursue these questions at the intersection of ontology and phenomenology. Lastly, thanks to Nicholas Spence for his helpful and encouraging comments on earlier versions of this article.
Funding
This work was supported by a Small Research Travel Grant from the Peter Lienhardt and Philip Bagby Memorial Fund, School of Anthropology and Museum Ethnography, University of Oxford.