
Abstract
We investigated the care of patients with age-related macular degeneration (AMD) managed via a physician-to-physician teleconsultation network for ophthalmology. Eleven groups of ophthalmologists took part in the study. The groups were located in 10 cities across Italy. Each group was based on a Retina Centre located at a university or hospital, with one or two expert ophthalmologists (20 expert ophthalmologists in total). In each region containing a Retina Centre, 6-10 general ophthalmologists (94 ophthalmologists in total) referred patients via the network for a period of three months between June 2011 and December 2012. An automatic grading system quantified the risk of disease progression, and a remote booking system allowed the referring ophthalmologist to make appointments directly with the appropriate Retina Centre. There were 360 network patients and 318 control patients (consecutive patients undergoing usual care during the previous three months). The time delay before therapy was significantly shorter in the network patients (mean 5.5 days) compared with the usual care patients (mean 28.7 days; P < 0.0001). There was a significant improvement in visual acuity in the network patients after treatment (first visit = 0.29 logMAR; after treatment = 0.22 logMAR; P < 0.05). In contrast, there was no improvement in the usual care patients (first visit = 0.29 logMAR; after treatment = 0.27 logMAR; P > 0.05). The telemedicine network allows regional ophthalmologists to quantify the risk of disease progression, and to send patients to a Retina Centre quickly and easily, when required.
Introduction
Age-related macular degeneration (AMD) is the main cause of legal blindness in people over 50 years old in the industrialised world.
1
The exudative form of the disease is characterized by the growth of abnormal neovessels beneath the macula, at the centre of the retina. Prompt intravitreal injection of antibody fragments of vascular endothelial growth factor (anti-VEGF) reduces new vessel growth,
2
and has become the main therapy for this disease (Figure 1). Anti-VEGF therapy is also used in the treatment of Retinopathy of Prematurity.
3
1a Fluorescein angiography of exudative AMD. Abnormal new vessels on the macula are clearly visible (arrow) and 1b After prompt anti-VEGF treatment, the disappearance of the new vessels is associated with improved visual acuity.
Teleophthalmology has been used for patients in rural areas 4 and circumstances such as war 5 to speed up care delivery. Many programmes have been developed for eye care, disease screening, monitoring, diagnosis and management. 6 To our knowledge, there are no specific programmes using anti-VEGF therapy for AMD.
Teleconsultation network
In 2010, we created a physician-to-physician teleconsultation network for ophthalmology. The network’s main components are a central server, a web accessible database, storage and forwarding functions, dedicated Electronic Medical Records (EMR), short message service (SMS) and email notification between physicians, guaranteed privacy and confidentiality, and a central help desk. 7
The new version of the teleconsultation network is called Reading Centre 2.0. The main developments in the software are: (1) application software for both computers and iPads/iPhones (iRetina, see Figure 2a); (2) a grading system accounting for five variables providing key information about the risk of exudative AMD:
8
–
11
age, visual acuity, Amsler test (a simple test to evaluate the presence of distortion in the central visual field), macular haemorrhage and the status of the second eye. This grading system gives a total score quantifying the risk of disease progression (Figure 2b). The grading system was validated and showed a sensitivity of 90% (unpublished data). Other important developments in the software are (3) an interactive booking system, to make an appointment directly with the Retina Centre from outside, with SMS notifications for patients (Figure 2c,d); (4) successive multiple masks for comparing images of the same EMR during follow-up, and (5) pop-up windows to assist physicians and ensure correct data entry. The network permits follow-up of AMD patients treated by groups of ophthalmologists all over Italy. The database and software were stored in a data warehouse in Milan (Datasys Network IBM Business Partner) to ensure uninterrupted availability and data security.
2a The app was designed for an iPad, 2b EMR grading system. The ophthalmologist gives a three-point score for five variables. The system then provides the total score (arrow). If the total score is ≥8, the ophthalmologist is advised to send the patient to the appropriate Retina Centre, 2c The general ophthalmologist's view of the calendar for making an appointment and 2d The Retinal Centre ophthalmologist's view of the calendar, which allows availability to be stated.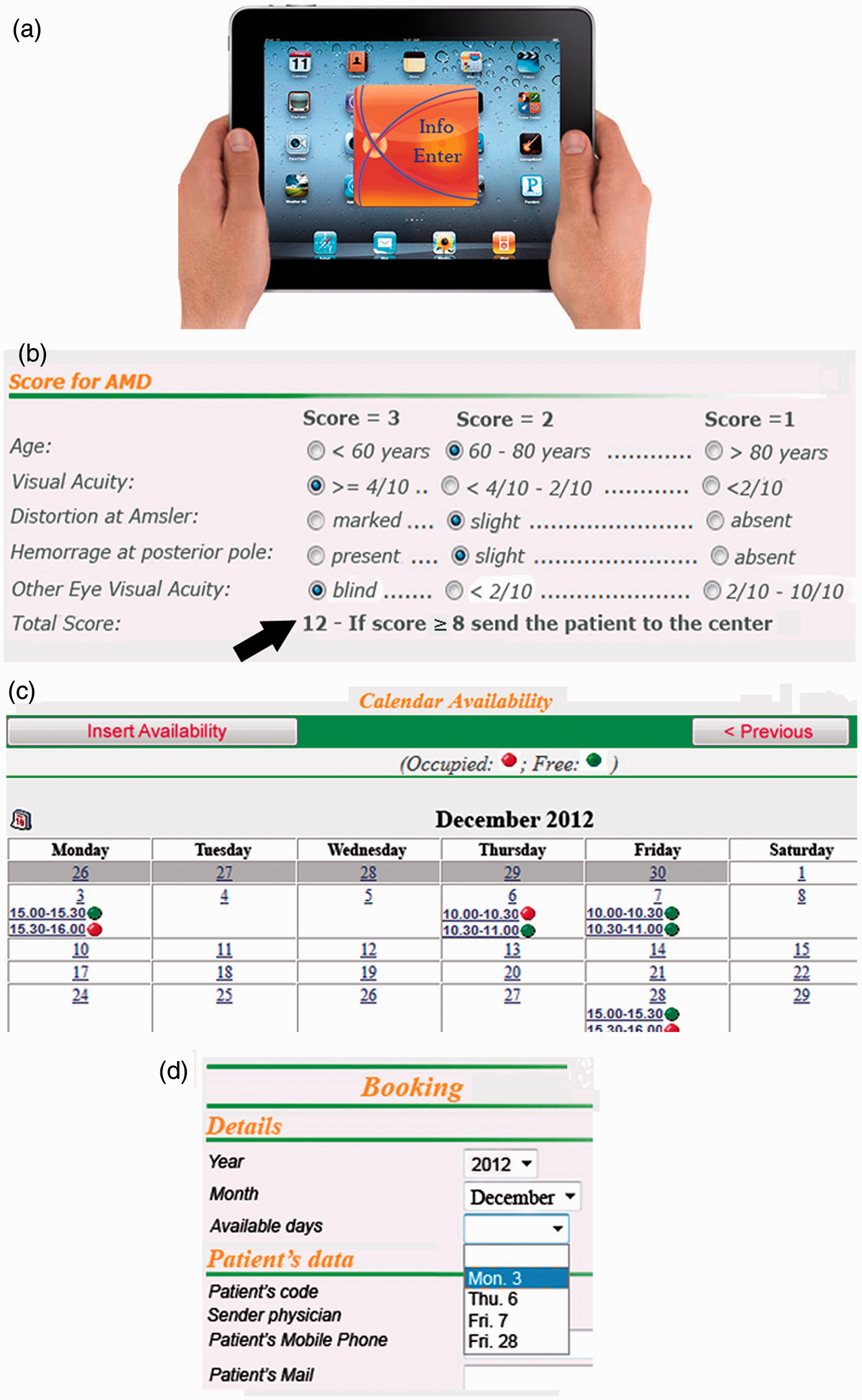
The aim of the present study was to investigate the care of AMD patients managed by the new network.
Methods
The study design was a longitudinal comparison of patient care in sites using the new telemedicine network. As a control group, we used consecutive patients undergoing usual care 12 – 14 (i.e. conventional in-person care procedures for diagnosis and treatment for AMD patients) during the three months before the use of the network began. Patient consent was obtained, and the study was approved by the appropriate ethics committee.
Eleven groups of ophthalmologists took part in the study. The groups were located in 10 cities across Italy (Figure 3). Each group was based on a Retina Centre located at a university or hospital, with one or two expert ophthalmologists (20 expert ophthalmologists in total). In each region containing a Retina Centre, 6-10 general ophthalmologists (94 ophthalmologists in total) referred patients via the network for a period of three months between June 2011 and December 2012.
Sites of the eleven groups of ophthalmologists (stars) and the related Retina Centres. SC denotes the Supervisory Centre in Milan, with the data warehouse, help desk and general coordination role.
A four-hour meeting was held in each city. Two authors explained how the system worked, and the procedures for its use (network login, database search, insertion of new data and answers, reading of message notification, correct entering of the grading system once the disease was suspected).
A tablet computer (iPad) was given to each participant. Web consultation tests were carried out on site. After the initial meeting, the general ophthalmologists used the teleconsultation network for a trial period of 7-10 days to exchange clinical data with retina specialists from Retina Centres. After the trial period, the ophthalmologists began to exchange real data over the following three-month period.
At the end of the three-month period, the ophthalmologists at each site discussed the following results at a final audit meeting: degree of access to the network, acceptability of technology and medical efficacy in terms of whether better therapy had been delivered as a result of the use of the network. The supervision and coordination of all activities, together with the final report, were carried out by the Supervisory Centre in Milan (Figure 3). Each ophthalmologist completed a short questionnaire (Appendix 1) about the use of the app.
To compare network care to usual care, we evaluated the following variables: time between the first visit and the onset of treatment, and visual acuity at the first visit and after treatment. Statistical analysis was carried out using a spreadsheet (Excel 2007, Microsoft Corp., Redmond, WA).
Results
Demographic and clinical data at the time of the first visit in patients suspected of suffering from exudative AMD.

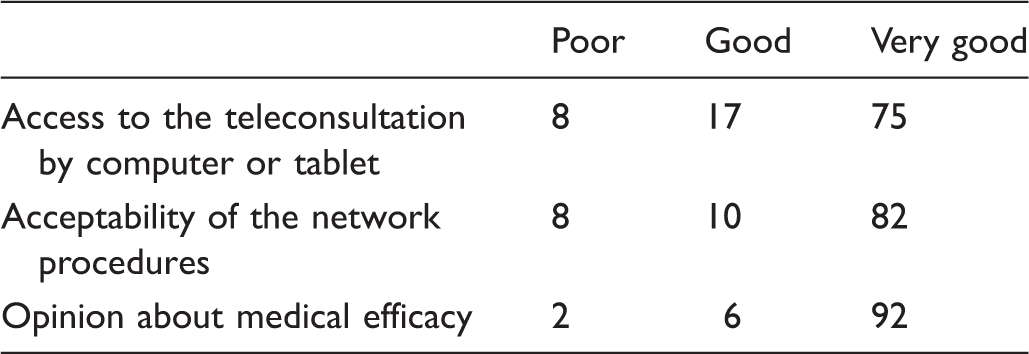
Responses (%) by the ophthalmologists (n = 114) during final audit meetings.
Out of the 310 cases sent to a Retina Centre, 189 cases (61%) were updated with additional clinical data acquired at the Retina Centre for the benefit of the general ophthalmologists. The consulting ophthalmologists also inserted 115 images relating to 89 patients to keep the general ophthalmologists informed.
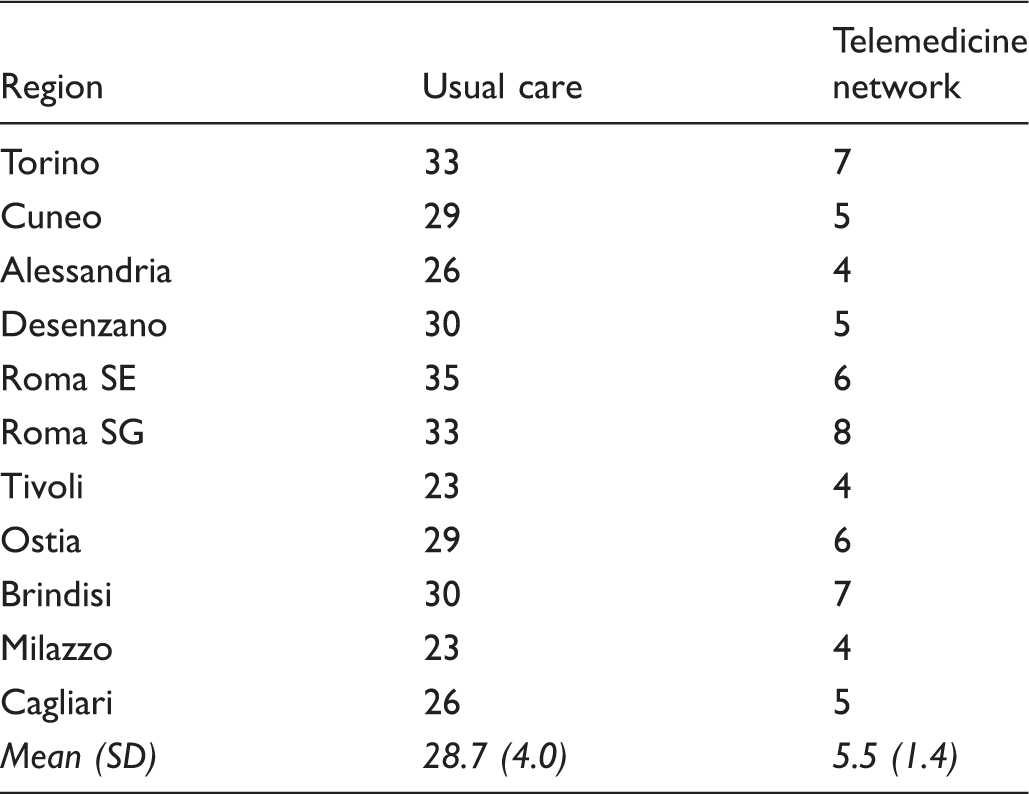
Interval (days) from the patient's first visit to the general ophthalmologist to therapy delivered at the Retina Centre.
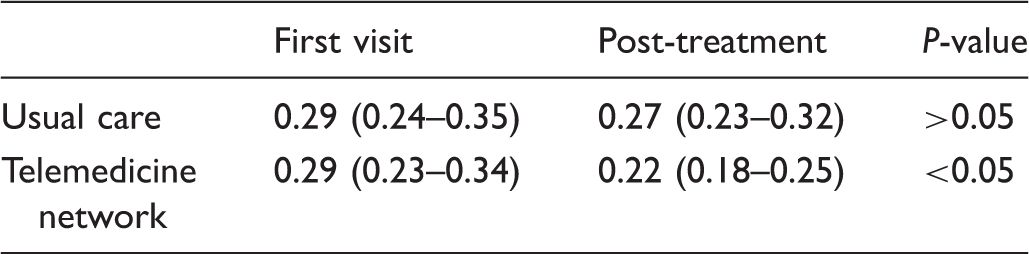
Mean visual acuity in the study patients. Values shown are mean LogMAR visual acuity (range). Lower scores represent better acuity.
Access to the teleconsultation network, acceptability of network procedures and medical efficacy were judged good or very good by all the general ophthalmologists (Table 2).
Discussion
Patients suffering a decrease in visual acuity usually make an appointment with their local general ophthalmologist. If the ophthalmologist suspects AMD, the patient has to make further appointments at a specialized public or private Retina Centre for additional testing and for anti-VEGF therapy when indicated. The majority of these patients are elderly people, who require organization and self-commitment, so the start of treatment is often delayed.
Our telemedicine network allows general referring ophthalmologists, who first identify AMD patients, to complete an EMR. The grading system then automatically indicates the risk of exudative AMD. If the score is high, the referring ophthalmologist can directly book an appointment for the patient at the appropriate Retina Centre. EMRs are visible to the Centre’s consulting ophthalmologist via the web, and SMS messages sent to both physicians and patients facilitate the booking process.
An important advantage of the network is the significant time reduction before treatment begins (Table 3). Any delay between initial diagnosis and treatment causes a significant decrease in final visual acuity recovery after treatment. Treatment procedures should be expedited, and delay should not exceed two weeks for the sake of vision preservation in individual patients. 15 The network, which reduces the time between visits and allows prompt therapy, has clear benefits for both patients and society as a whole.
Another advantage of the network is the interaction between general ophthalmologists and those working in ophthalmology centres to reduce the number of trips made (and money spent) by patients and their companions. This is particularly burdensome in anti-VEGF treatment, where therapy may need to be carried out for many years. We estimated that each of our 310 patients, sent directly to the relevant Retina Centre, avoided 1-2 visits, as well as the accompanying trips by their companions, during the three-month study.
The automatic grading system helped general ophthalmologists decide to send patients to the Retina Centre. The grading system has limitations, but takes into consideration the fact that general ophthalmologists do not have the facilities for carrying out detailed instrumental analyses.
Another important function allows a general ophthalmologist, who is the first doctor seen by the patient, to make a direct appointment with the Retina Centre. A calendar function allows the general ophthalmologists to make the appointment and also allows consulting ophthalmologists to indicate their availability (Figure 2c,d). Wasted appointments can be avoided, and SMS and email notifications are sent to both ophthalmologists and patients, indicating the time and place of the visit.
We believe that the success of the teleconsultation work was due to the involvement of interested groups of ophthalmologists, and to useful software functions, such as the grading system and the online appointments calendar. The use of portable devices, the high number of CME credits (20 credits) and the remote help-desk service for assistance, advice and news were also important.
The present study had certain limitations. The cohort of patients studied was not randomized, and simply represents a before and after trial. Ophthalmologists possess differing levels of skill regarding information technology, the ability to use the network and interact with the help-desk when necessary, which might introduce bias. The aim of the preliminary training phase was to limit this possible bias as much as possible.
In conclusion, delay plays a key role in the final outcome of exudative AMD, where abnormal new vessels grow rapidly at the centre of the retina. Treatment delay results in a permanent loss of final visual acuity. The telemedicine network allows regional ophthalmologists to quantify the risk of disease progression, and to send patients to the Retina Centre quickly and easily, when required. The treatment process using anti-VEGF therapy was accelerated, and final outcome improved. This is an example of how clinical telemedicine can benefit both patients and the healthcare system, and we believe that the same model might be applicable in many other medical specialties.
Footnotes
Acknowledgements
We thank the consulting ophthalmologists at the Retinal Centres and the 94 general ophthalmologists. We also thank Michael John for his assistance. The work was supported by Andrea Marazzi through an educational grant from Novartis Farma S.p.A. Italy.
Appendix 1. Questionnaire for app users
Access to the teleconsultation by computer or tablet was:
Poor Good Very good Acceptability of the network procedures was:
Poor Good Very good The medical efficacy of the teleconsultation was:
Poor Good Very good