
Abstract

The Rizzoli Orthopaedic Institute in Bologna is the oldest centre of excellence for orthopaedics in Italy. It specialises in musculoskeletal tumours and joint surgery. More than half of the Institute's patients come from outside the region where it is located (Emilia-Romagna), and a substantial number come from the far south of Italy. Because of the effort required to travel to Bologna from the South, an experimental telemedicine service was started in the late 1990s. After positive results1–3, a routine service began in 2002, providing teleconsultations to patients living in the five more distant regions of the country (Sicilia, Sardegna, Calabria, Puglia, Campania).
The technological infrastructure is based on a Virtual Private Network and video-over-IP, and it is operated by a private company (HIM.IT s.r.l.). The company is also responsible for establishing partnerships with the remote sites (health centres, hospitals and outpatient clinics) which host the teleconsulting service for the patients. Each of the five regions has one or more remote sites. 4
In the first three years, teleconsultations were provided by orthopaedic specialists for follow-up and for second opinions. Starting in 2005, teleconsultations were also provided by anaesthetists, who interviewed patients and collected their clinical data, thus avoiding travel before scheduled surgery at the Rizzoli Institute. Thus the three kinds of teleconsultations were:
anaesthetic: to interview patients before planned surgery at the Rizzoli Institute orthopaedic follow-up: post-surgery review of Rizzoli patients orthopaedic second opinion: for patients with no previous contact with the Rizzoli Institute.
In conventional practice, a face-to-face orthopaedic consultation may require some physical interaction between the specialist and the patient. Because of this, when a patient contacts the call centre of the telemedicine service, the operator completes a form with the clinical history and collects any diagnostic test results already available. An orthopaedic specialist then evaluates this material in order to decide whether the case is suitable for teleconsultation, and if additional diagnostic examinations will be required.
Teleconsultations for follow-up and second opinion are normally supported by radiological imaging, such as X-rays of the joints, CT and MRI scans, ultrasound, PET or SPECT scans. The anaesthetist usually requires blood tests, chest X-rays, doppler ultrasonography and ECG examinations. To avoid delays, the examination results are normally transmitted from the remote sites to the Rizzoli Institute before the teleconsultation takes place. In the first years of the service, much of the diagnostic imaging was still recorded on film or paper, and this required a digital conversion step before transmission. With the widespread adoption of digital imaging and PACS systems, this conversion was no longer required.
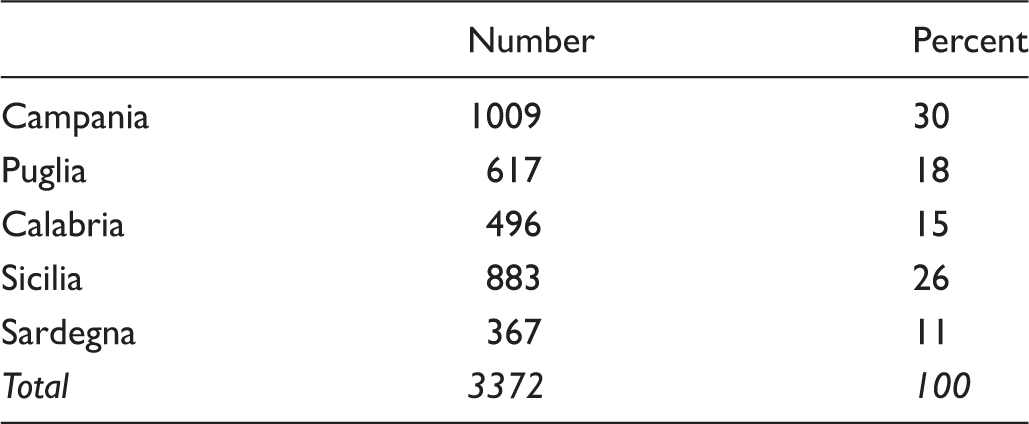
Regional distribution of the patients.
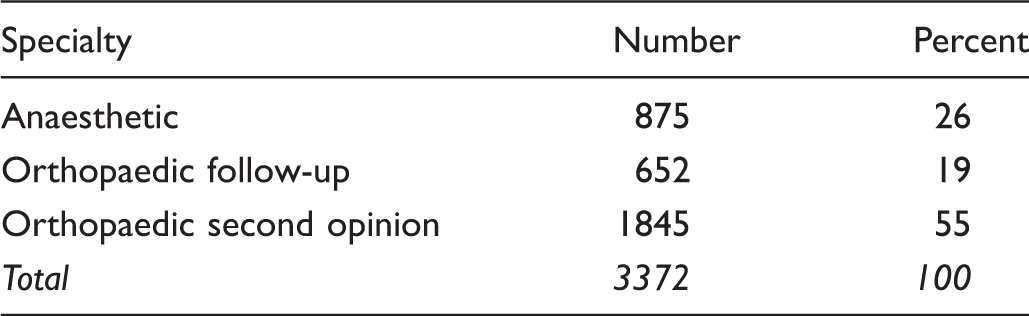
Types of teleconsultation provided.
Although the teleconsulting service represents the largest Italian experience for telemedicine applied to orthopaedics, its sustainability is still unknown. The main problem is the absence of any reimbursement policy in the National Healthcare System (NHS) for telemedicine services. The fact that the service is only available for private-paying patients is an ethical problem, but it is also an obstacle in reaching a larger potential market. Unless there is a substantial increase in the number of patients, the cost of the technology and the service management will remain high.
In the last few years there has been an important re-organization of the relationship between the national healthcare system in Italy and the regional authorities, in terms of responsibilities, healthcare funding and legislation on healthcare. There are now 21 different regional healthcare systems, rather than a single national healthcare service. The tension between the national and the regional level has been made worse by the reduction in national funding for public healthcare, due to the economic crisis affecting the country. This, of course, is the opposite of what is necessary for the development of a teleconsulting service between different regions. If this continues, then the outlook for telemedicine in Italy will be bleak.
Some hope comes from an attempt to share national telemedicine guidelines, as recently discussed by the ministry of health and by the 21 regions. In the draft guidelines, telemedicine services have been classified and minimum standards laid down for use within the NHS. Ethical and organizational aspects are defined, with attention to relevant European legislation and future trends. Furthermore, the proposed guidelines describe for the first time the different economic models for providing telemedicine services to private paying patients or those within the NHS.
Despite good results from telemedicine for more than a decade, the long-term sustainability of the teleconsulting service at the Rizzoli Orthopaedic Institute could be jeopardised unless a regulatory framework is rapidly approved. The definition and the application of national guidelines is crucial to the positive evolution of telemedicine in Italy.