
Abstract
We evaluated the quality of telephone triage and the appropriateness of the decisions resulting from it at a primary care out-of-hours service. Four simulated clinical cases were used in the Incognito Standardized Patient method: an adult with nosebleed, an adult with fever, a child with fever and a child with vomiting. There was a set of obligatory questions for each case, translated from those used in a previous study. Quality was assessed by the proportion of questions asked by the call-handlers during telephone triage versus those that should have been asked. A total of 22 out-of-hours doctors were involved in the study, working in two different locations in the Verona city area. Over a 4-month period each of the four simulated clinical cases was used five times in calls to the two centres involved. The proportion of obligatory questions asked compared to those expected to be asked was 27–36%. On three occasions out of the 40 simulations, all of which were considered to be manageable by telephone, the patient was advised to go to an outpatient clinic for a face-to-face evaluation. The average duration of the calls was 3 min 47 s. The quality of telephone triage in the regions studied was low and provided considerable room for improvement. This is relevant to patient safety and risk management of the service.
Introduction
Telephone triage is the central part of a primary care out-of-hours service as it is the phase in which patient information is collected to determine the urgency of a medical problem and to decide on the care needed by the patient. There have been various studies of telephone triage in terms of security,1–3 differences in performance between different health care personnel, 4 effectiveness in reducing visits to general practitioners (GPs) and hospital referrals,5–8 patient satisfaction9,10 and the propensity of patients to follow the advice given to them.11,12
Telephone triage should meet one of the criteria of quality which is to minimize the clinical risks that it entails. Thus it is important for the health care personnel involved in a primary care out-of-hours service to receive appropriate training and to have access to modern support tools. The quality of telephone triage and the appropriateness of the decisions made are complex, and depend on the communication skills, medical knowledge and experience of call-handlers in assessing the clinical information collected through telephone triage.1,12,13 Recent studies have investigated the quality of telephone triage in primary care out-of-hours services in the Netherlands1,14,15 and the UK, 16 but there have not been any studies in Italy.
The aim of the present paper was to evaluate the validity of telephone triage by comparing the questions asked by call-handlers during telephone triage with those that should have been asked, and examining their decisions about therapy. 1
Methods
We evaluated the quality of telephone triage and the appropriateness of the decisions resulting from it, at two call centres in Verona serving Verona Province. In this service, the call-handlers were doctors. A total of 22 out-of-hours doctors were involved in the study, working in two different locations. Before the study began, the doctors were given an information letter about the study. All the doctors gave their consent to participate. The study was approved by the appropriate ethics committee and by the local public company providing out-of-hours care services (ULSS 20).
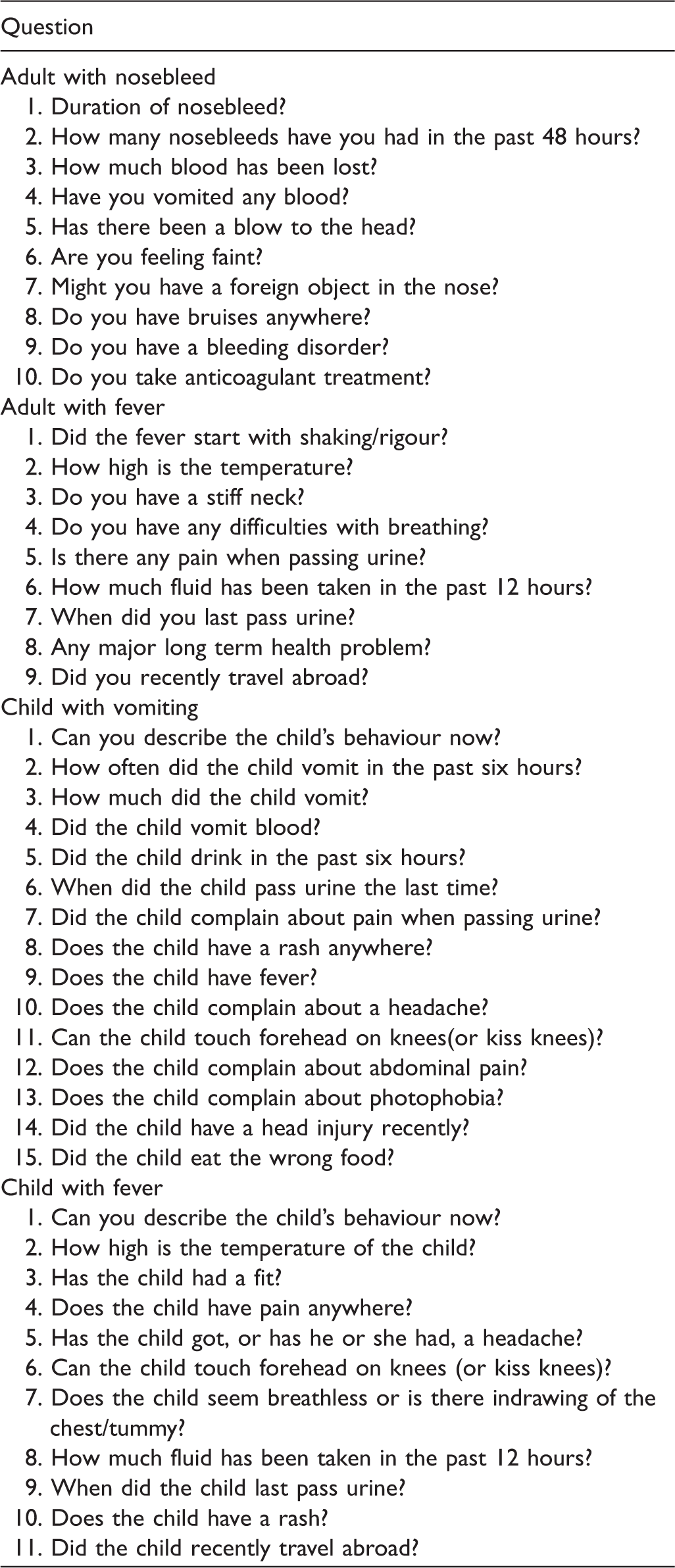
Clinical cases
Obligatory questions to be asked in each case.
Handling of clinical cases
The four cases were handled by primary care out-of-hours telephone triage staff in a four month study period beginning in June 2011. The cases were randomly proposed using the Incognito Standardized Patient (ISP) method.14,17–20 One of the researchers would telephone incognito one of the out-of-hours services in the Verona city area and give information concerning an illness without revealing that the case was simulated for the purposes of study and was not real. 1
The clinical cases did not require the call-handler to advise a home visit or to call the emergency ambulance service. If the person answering the calls had given such advice, callers would have revealed their true identity immediately and the nature of the study. Over the 4-month period each of the four simulated clinical cases was used five times in calls to the two centres involved, i.e. there was a total of 40 calls. No sample size calculation was conducted before the study began.
Because of their monthly shifts, each telephone triage call-handler received about 1 call per month. The calls were made from 21:30 to 23:30 for night shifts and from 11:00 to 19:00 for day shifts, thus avoiding calling at times particularly inconvenient for the telephone triage staff (for example, late at night and at the times of shift change).
The researchers involved in the role of the Incognito Standardized Patient were three men and three women, aged 24–42 years. They received structured instructions, and were supervised during their performance in order to reduce heterogeneity in the presentation of the cases.
To reduce the chance of repeating a clinical case to the same doctor, we took into account the shifts of the telephone triage participants. When making the calls we switched between simulated patients of both sexes, changing the patient names given to the doctor for every telephone call. We also used as many different telephones as possible, because the number was visible to the doctor and was stored in an archive of previous calls.
The standardized clinical cases were administered with the support of a written framework where the ISP could take notes and flag the questions asked. All the calls were recorded and listened to again if necessary.
Outcome measures
For each call made we noted: (1) the proportion of compulsory questions the call-handler asked compared to the questions on the standard reference list; (2) the proportion of correct decisions made by the call-handler; and (3) the length of the call itself. The duration of the simulated call was measured from the moment the conversation began until the parties hung up.
We could not link the out-of-hours doctors' demographic data to performance data because ISPs were blind with regard to doctors' identity. Also, out-of-hours doctors do not usually introduce themselves at the beginning of telephone consultations and asking for the doctor's identity could suggest to the call-handler that the caller was not a real patient.
Results
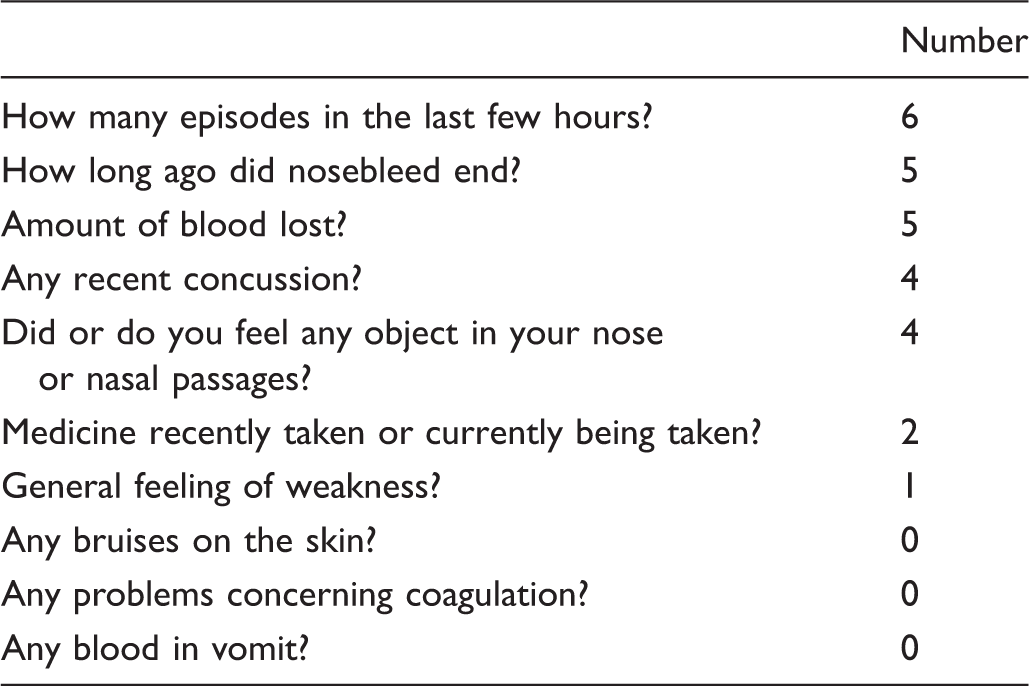
Adult with nosebleed. Number of doctors (of 10) who asked the obligatory questions.
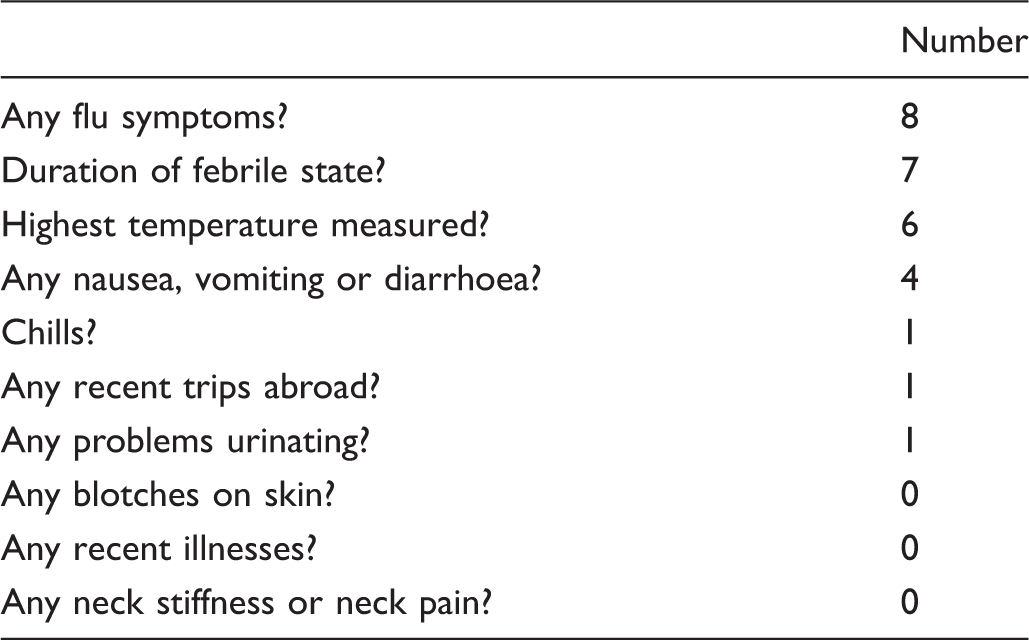
Adult with fever. Number of doctors (of 10) who asked the obligatory questions.
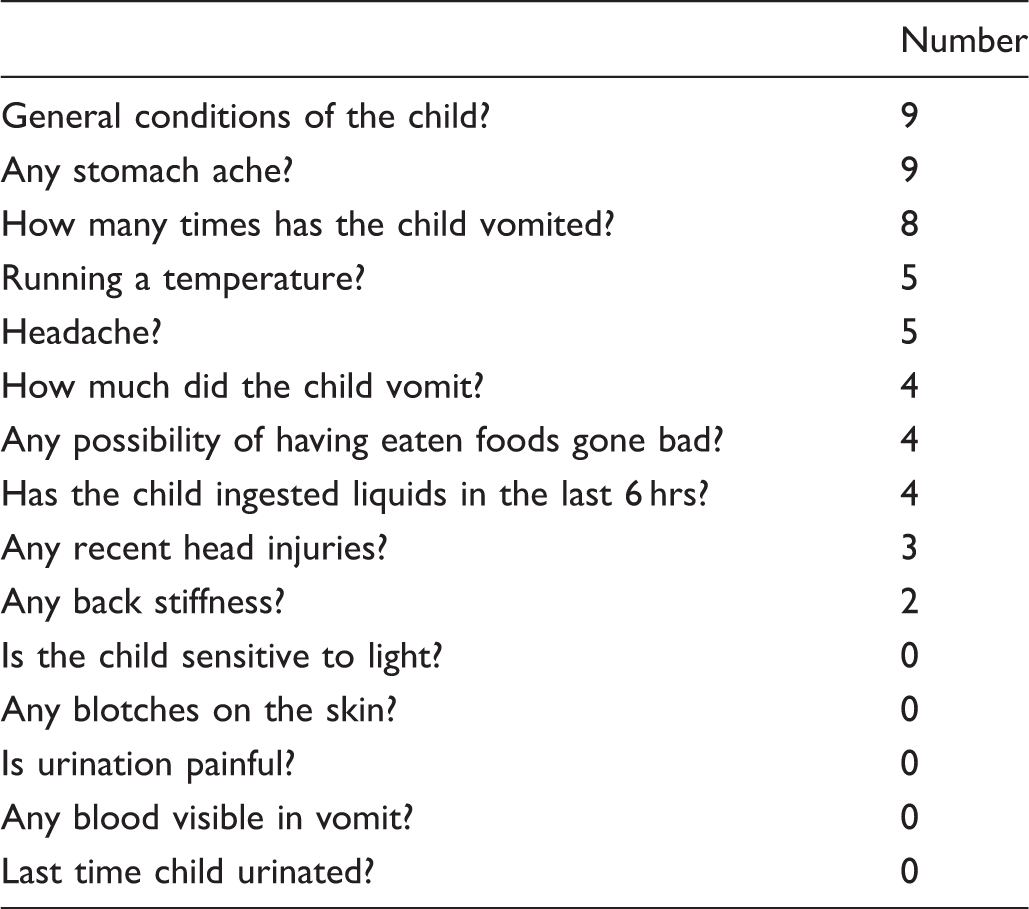
Child with vomiting. Number of doctors (of 10) who asked the obligatory questions.
Child with fever. Number of doctors (of 10) who asked the obligatory questions.
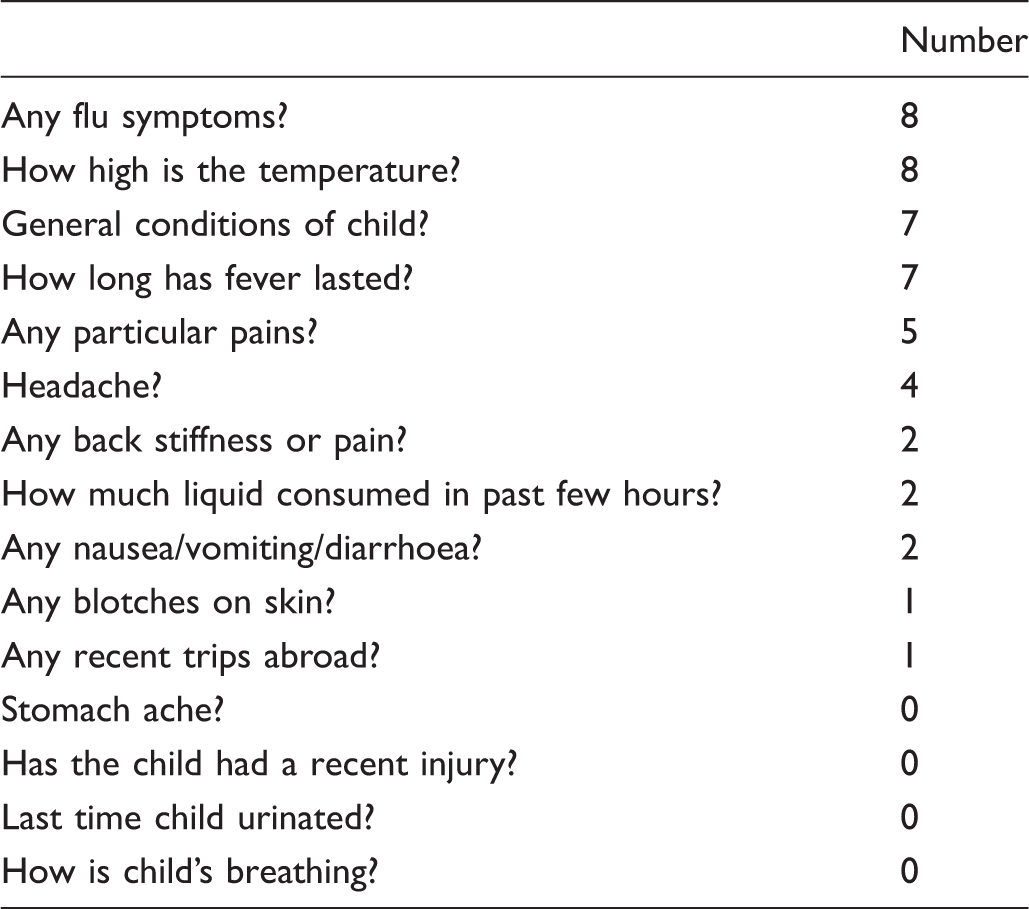
There were a few questions that were important in determining the clinical severity of the patients' symptoms, such as for the adult with fever, eight doctors asked about flu symptoms but none asked about neck pain. The doctors tended to ask a few questions, probably because the symptoms described in the simulated cases were very common and in most situations they were unlikely to mask serious diseases. Both in the adult (Tables 2 and 3) and the child patients (Tables 4 and 5), no attention was given to symptoms or conditions which might signal a more severe disease, such as asking about travel abroad to exclude any tropical disease.
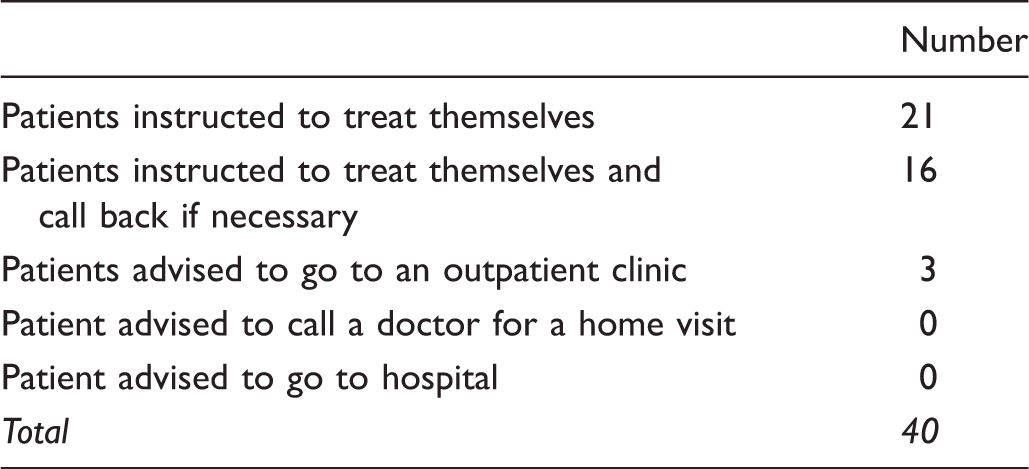
Management decisions concerning the 40 simulated cases.
At the end of the study we asked the doctors involved if they had suspected that the calls received were fake calls; no doctor gave a positive response.
Discussion
The results of the study showed that there were significant deficiencies in the telephone triage provided in the out-of-hours primary care service and, therefore, ample room for improvement. Indeed the study showed that the quality of telephone triage, in terms of mandatory questions asked during the call, was well below the desired standard, although the ability to assess the case, the clinical management decisions made and the treatment advised was almost always appropriate (it should be kept in mind, however, that the cases were not especially severe). The deficiencies found during triage might have been due to the call-handlers’ inexperience or lack of training, but were probably the result of fatigue resulting from night shifts, repetitiveness and the difficulty of dealing with the callers’ emotions and expectations together with the problem of making a remote evaluation of the seriousness and urgency of the case.
In comparing the results of the previous study conducted in the Netherlands and those of our study, involving the same simulated clinical cases, we found 70% versus 36% of mandatory questions asked in the case of a child with vomiting, 47% versus 32% in the case of the child with fever, 36% versus 28% in the case of the adult with fever, and 54% compared to 27% of the adult with nosebleed, respectively. A service in which only one-third of the questions necessary to make a correct decision is actually asked represents a high medical risk and could become a medicolegal burden on patients and doctors. Telephone triage is a delicate phase of a telephone consultation during which there is the risk that insufficient information is given by the caller resulting in an underestimation of the case, with potentially serious consequences for the patient, or an overestimation of the case with advice for inappropriate treatment that could also be economically disadvantageous. In other words, the quality of the telephone triage service and the risks that teleconsultations and telediagnoses entail are closely related.
The present study had several limitations: (1) the small size due to limited resources; (2) the use of clinical cases of mild severity, because the call-handler might have decided that a face-to-face consultation was required; (3) the complexity of the ISP method; (4) the lack of a comprehensive statistical analysis; (5) the limited generalizability; (6) the use of standardized clinical cases built by expert consensus, but not directly supported by evidence-based guidelines (because no evidence based clinical guideline provides questions to be administered in a telephone triage setting). Nonetheless, the study demonstrated that the model is feasible, and enabled us to assess to what extent and in what areas the quality of telephone triage concerning out-of-hours primary care requires improvement.
Several suggestions for future research emerged from the study. We chose not to call at times particularly inconvenient for the out-of-hours staff (e.g. late night and shift change). However, these times could be particularly important, as these are times when mistakes might be more likely to occur. Another question that emerges from the study regards the strategies that should be adopted in order to improve the quality of telephone triage. These include the effect of specific training, in particular training on management techniques and structuring telephone consultations, 15 and the effectiveness, efficiency and security that computerized support could offer the telephone triage doctors in decision making. Previous studies have shown that decision-making tools are safe and can reduce the clinical risks associated with unassisted telephone triage call handlers, as well as being cost-effective and possibly reducing the number of unnecessary visits to emergency room services.21,22
The results of the present study show that the quality of telephone triage in the regions studied was low and that there was room for improvement. The doctors answering the telephone asked a very low proportion of obligatory questions and this could affect patient safety and risk management for the service itself. Research is required to identify ways of improving the situation.
Footnotes
Acknowledgements
We are grateful to Hay Derkx (Maastricht University) for his collaboration.