
Abstract
Telemedicine is widely used for medical education but few studies directly investigate how telemedicine teaching compares to conventional in-person teaching. Here we determine whether telemedicine teaching is as effective as in-person teaching for the acquisition of an ultrasound skill important in trauma care. Nurses with no prior ultrasound experience (n = 10) received study material and a teaching session on how to locate and image the hepatorenal space (Morison’s pouch). One group of nurses was taught in-person (In-person Group) and the other group was taught via telemedicine (Telemedicine Group). Telemedicine allowed two-way audio and visual communication between the instructor and the nurses. A comparison of the teaching techniques showed that telemedicine teaching was equivalent to in-person teaching for the acquisition of practical and theoretical skills required to locate Morison’s pouch. The average time required to locate Morison’s pouch after teaching was similar between both groups. The results demonstrate that telemedicine teaching is as effective as in-person teaching for the acquisition of bedside ultrasound skills necessary to identify Morison’s pouch. Remote teaching of these bedside ultrasound skills may help in the diagnosis of intra-abdominal bleeding in rural healthcare centers.
Introduction
In abdominal trauma patients, the sonographic assessment of the hepatorenal space (Morison’s pouch) is used for the rapid diagnosis of intra-abdominal bleeding. Specifically, the sonographic identification of fluid in Morison’s pouch may indicate intra-abdominal bleeding.1–7
The rapid diagnosis of intra-abdominal bleeding is often hindered in rural and remote areas due to a lack of adequate equipment and trained clinicians.8–11 This problem has been addressed by in-person ultrasound training of medical personnel in remote settings. 12 It has also been addressed by telementoring and supervision of sonographic skills performed by remotely-stationed healthcare personnel. 12
Recent studies indicate that telemedicine can be used for teaching bedside ultrasound skills to healthcare providers with no prior ultrasound experience. Studies report teaching bedside ultrasound to ultrasound-naive physicians, 13 nurses,14,15 medical students, 16 non-healthcare workers, 17 and non-medical personnel in military and extra-terrestrial environments.18,19
While teaching ultrasound skills by telemedicine is widespread, a direct quantitative comparison of telemedicine teaching versus in-person teaching has not been previously addressed to our knowledge. The aim of this study was to compare the effectiveness of telemedicine teaching versus in-person teaching of an ultrasound skill important in the diagnosis of intra-abdominal bleeding. This prospective study is based on our previous experience over the past decade of in-person teaching of abdominal ultrasound to medical students and physicians with no prior experience in bedside ultrasound. 20 Here we set out to determine whether using telemedicine teaching is comparable to in-person teaching for imaging Morison’s pouch. Imaging Morison’s pouch is a straightforward and attainable ultrasound skill, chosen as a proof of principle for the teaching comparisons in this pilot study. Imaging Morison’s pouch is only one aspect of the Focused Assessment Sonography for Trauma (FAST) algorithm that is commonly used to diagnose abdominal bleeding. Remote teaching of this discrete skill and ultimately the FAST algorithm could benefit trauma care in rural areas of developed and developing countries.
Methods
Study participants
Nurses (n = 10) were recruited from St. Mary’s Hospital Center (a McGill University teaching hospital) and randomly divided equally into two groups (In-person Group and Telemedicine Group). All nurses had similar levels of clinical experience and no prior ultrasound experience.
Procedures received Full Institutional Approval (#14-27) by the Research Ethics Committee at St. Mary’s Hospital Center. All participants gave voluntary informed consent.
Assessment of teaching techniques
Both groups were given identical educational study material consisting of the fundamental basics of bedside ultrasound and an anatomical review of Morison's pouch (n = 19 pages). The study material contained selected chapters from an ultrasound beginner textbook. 21
One week later, the In-person Group and the Telemedicine Group received identical teaching sessions on how to image Morison’s pouch. Teaching sessions consisted of a short demonstration of the correct ultrasound technique for locating and imaging Morison’s pouch, followed by one-on-one coaching with each member of the group. Teaching sessions lasted approximately one hour and were performed on a healthy volunteer by an Emergency Department Targeted Ultrasound (EDTU) instructor for the Canadian Association of Emergency Physicians (CAEP). No distinguishable volunteer characteristics or images are reported in this manuscript.
The same instructor taught both the In-person Group and the Telemedicine Group. The In-person Group was taught with the instructor in the same hospital room while the Telemedicine Group was taught using telemedicine, i.e. with the instructor in an adjoining suite of the same hospital. Telemedicine allowed two-way audio and visual communication between the instructor and the nurses (Figure 1).
Telemedicine equipment at St. Mary’s Hospital Center. Two Cisco Edge 95 MXP videoconferencing devices were connected point to point at a data transfer rate of 768 kbps over IP network using H.323 protocol. The ultrasound systems video outputs were transmitted using the presentation channel (duo video).
Description of criteria used to rate the acquisition of practical skills.
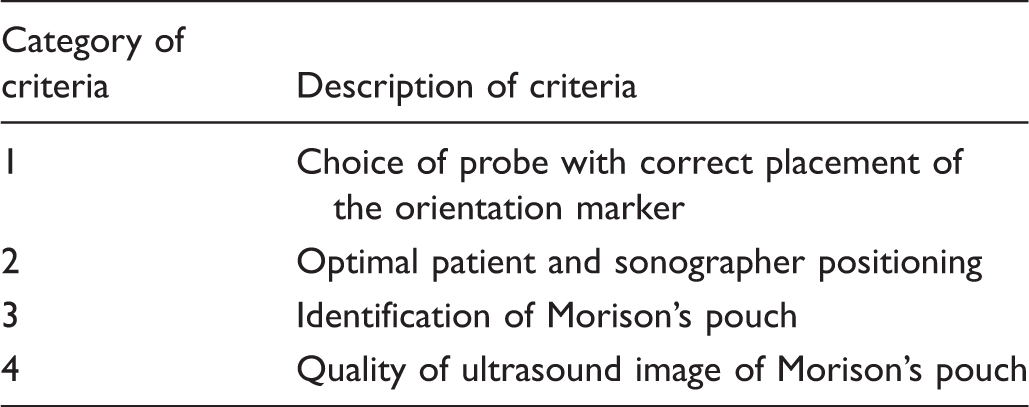
The theoretical test was composed of nine questions designed to test for knowledge of basic ultrasound physics, probe choice, image generation technique, and the importance of imaging Morison’s pouch.
Telecommunication technology
Two Cisco Edge 95 MXP videoconferencing devices were connected point to point with a data transfer rate of 768 kbps over IP network using H.323 protocol. The transfer rate was set below the maximum transfer rate of 1920 kbps as the equipment was configured for telemedicine connections to remote areas in northern Canada and subject to satellite-imposed restrictions on data transfer rates. Despite a sub-maximal data transfer rate, all participants confirmed an excellent clarity in the ultrasound images and no observed loss in frame rate. The ultrasound systems video outputs were transmitted using the presentation channel (duo video).
Statistical analysis
Statistics are quoted as mean ± standard deviation (SD). Significant differences were determined using a Fischer’s exact contingency test (for comparisons of practical test scores, Figure 2A–C), a Mann Whitney test (for comparisons of time to locate Morison’s pouch, Figure 3), and a Wilcoxon matched-pairs signed rank test for comparisons of theoretical test scores, Figure 4A–B). All statistical analyses were performed using GraphPad Prism 6.0f (GraphPad Software, Inc, La Jolla, CA, USA).
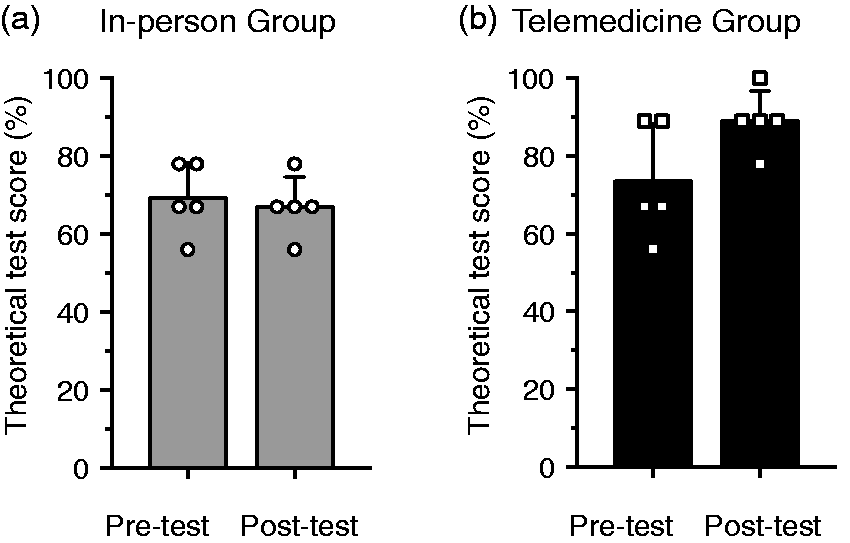
Telemedicine teaching is equivalent to in-person teaching for the acquisition of a practical ultrasound skill (locating Morison’s pouch). (a) The In-person Group significantly increased its practical test score after in-person teaching from 0/20 criteria (Pre-test) to 20/20 criteria (Post-test). *P < 0.001. (b) The Telemedicine Group significantly increased its practical test score after telemedicine teaching from 0/20 criteria (Pre-test) to 19/20 criteria (Post-test). *P < 0.001. (c) A comparison of the post-test scores for the In-person Group versus the Telemedicine Group showed no significant difference. P = 1. Telemedicine teaching is equivalent to in-person teaching for the time required to perform a practical ultrasound skill (locating Morison’s pouch). Telemedicine teaching was equivalent to in-person teaching for the acquisition of theoretical knowledge. (a) The In-person Group showed similar mean scores after in-person teaching for the theoretical pre- and post-tests. Error bars ± SD. (b) The Telemedicine Group showed similar mean scores after telemedicine teaching for the theoretical pre- and post-tests. Error bars ± SD.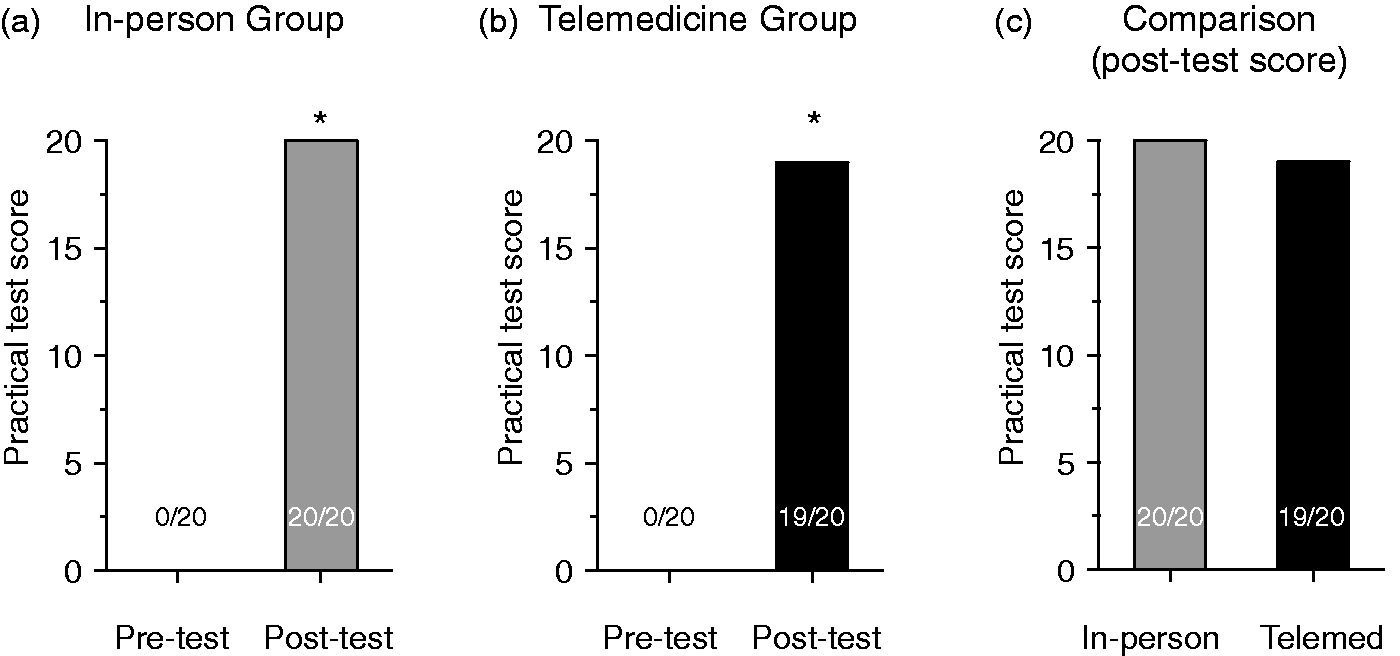
Results
All members of the two groups completed the practical and theoretical pre- and post-tests.
Telemedicine teaching is equivalent to in-person teaching for the acquisition of practical ultrasound skills
Prior to receiving the teaching session, the In-person Group was unable to locate Morison’s pouch with ultrasound (mean practical pre-test score was 0/20 criteria for all five nurses; Figure 2A). After receiving the teaching session, the In-person Group was able to locate Morison’s pouch with ultrasound and significantly improved their mean practical test score to 20/20 criteria (P < 0.001; Figure 2A).
A similar improvement was observed in the practical test score for the Telemedicine Group after receiving the teaching session via telemedicine. The Telemedicine Group was unable to locate Morison’s pouch with ultrasound prior to the teaching session then significantly increased their score from 0/20 to 19/20 following the teaching session (P < 0.001; Figure 2B).
A direct comparison of the practical skills of the In-person Group and the Telemedicine Group after receiving the teaching session revealed no significant difference in the practical post-test scores for the two groups (20/20 versus 19/20; P = 1; Figure 2C). Thus teaching via telemedicine is equivalent to in-person teaching for the acquisition of practical ultrasound skills necessary to locate Morison’s pouch.
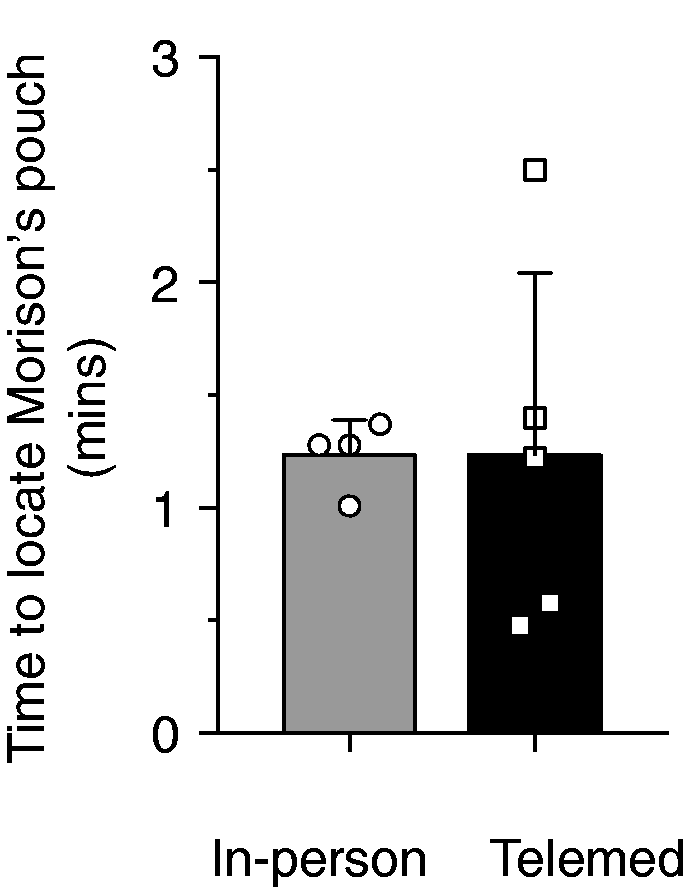
Telemedicine teaching is equivalent to in-person teaching for the time required to perform a practical ultrasound skill
The time required to perform the practical ultrasound skill of locating Morison’s pouch was assessed after receiving the teaching session. The In-person Group reported a mean time of 1.24 ± 0.16 min to locate Morison’s pouch. The Telemedicine Group displayed a mean time of 1.24 ± 0.81 min (P = 0.86; Figure 3). Thus teaching via telemedicine is equivalent to in-person teaching with regard to the speed of performing an acquired practical ultrasound skill.
Telemedicine teaching is equivalent to in-person teaching for the acquisition of theoretical ultrasound knowledge
The acquisition of theoretical ultrasound skills was assessed one week after receiving the study material and prior to receiving the teaching session. The In-person Group attained a mean theoretical pre-test score of 69 ± 9% (Figure 4A). This theoretical test score did not change significantly after receiving the teaching session (post-test score of 67 ± 3.5%; P = 0.99; Figure 4A).
The mean theoretical pre-test score for the Telemedicine Group was 73 ± 15% prior to the teaching session (Figure 4B). After the teaching session, the mean theoretical test score of the Telemedicine Group did not significantly change (post-test score of 89 ± 3.5%; P > 0.05; Figure 4B).
Discussion
This pilot study demonstrates that telemedicine teaching is equivalent to in-person teaching for the acquisition of bedside ultrasound skills necessary to identify Morison’s pouch. Specifically, telemedicine teaching was equivalent to in-person teaching for the acquisition of practical skills (Figure 2), the speed of execution of the acquired practical skills (Figure 3), and the acquisition of theoretical knowledge (Figure 4).
The demonstration that teaching an ultrasound skill by telemedicine is as effective as in-person teaching is in keeping with previous studies showing that medical students learn clinical knowledge via telemedicine as well as via traditional classroom lectures. 22 Another report demonstrates that medical students prefer telemedicine teaching over in-person teaching with regard to clarity of procedures, ability to ask questions, and quality of time spent learning surgical procedures. 23
The assessment of practical skills before and after the teaching session was performed in-person for both the In-person and Telemedicine Groups (Figure 2). The assessment of practical skills was identical to an assessment currently in use for student, resident, and physician level bedside ultrasound courses (personal communication). Future studies will implement a remote assessment of practical skills as necessitated by telemedicine teaching in rural areas.
The lack of significant change in the theoretical pre- and post-test scores (Figure 4) suggests the nurses were sufficiently self-taught such that no additional theoretical learning could be gained from the teaching session. This reinforces the usefulness of the pre-course reading material.
This pilot study is limited by its small sample size of ultrasound-naïve healthcare personnel. In addition, our study was limited to teaching one discrete ultrasound skill. The relative effectiveness of in-person versus telemedicine teaching of more complex ultrasound skills remains to be determined.
Our results may help to address the lack of healthcare personnel trained in the use of ultrasound in remote areas. Often rural clinicians have to travel to major centers to receive medical education and training in the use of ultrasound. Alternatively, trained physicians from major centers have to travel to teach in remote areas. 12 Both systems are time-consuming and costly. Teaching by telemedicine offers an economical alternative for teaching ultrasound skills in remote or limited-resource settings.
In conclusion, the results demonstrate that telemedicine can be used to successfully teach ultrasound-naïve clinicians the bedside ultrasound skills necessary to identify Morison’s pouch. Telemedicine teaching was equivalent to in-person teaching for the acquisition of practical skills and theoretical knowledge. Identification of Morison’s pouch is one aspect of the FAST algorithm. Future studies with a greater sample size and additional study material will compare the effectiveness of telemedicine teaching versus in-person teaching of the complete FAST algorithm for the treatment of traumatic injuries in remote healthcare centers.
Footnotes
Acknowledgements
We thank St. Mary’s Hospital Center for kindly providing the telemedicine equipment. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. An abstract of this work was presented at the Third Annual World Congress Ultrasound in Medical Education.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of contributorship
PS: conception and design, ultrasound instructor, data interpretation, manuscript writing and final approval of manuscript; A-MB: participant recruiting, collection and assembly of data, data analysis and interpretation, manuscript writing; SO: data analysis and interpretation, manuscript writing and final approval of manuscript: JL: final approval of manuscript; AR: final approval of manuscript, ultrasound examiner.