
Abstract
Introduction
Tele-emergency provides audio/visual communication between a central emergency care centre (tele-emergency hub) and a distant emergency department (remote ED) for real-time emergency care consultation. The purpose of this mixed methods study is to examine how often tele-emergency is activated in usual practice and in what circumstances it is used.
Methods
Tele-emergency log data and merged electronic medical record data from Avera Health (Sioux Falls, SD) were analysed for 60,193 emergency department (ED) encounters presenting over a two-and-a-half year period at 21 critical access hospitals using the tele-emergency service. Of these, tele-emergency was activated for 1512 ED encounters.
Results
Analyses indicated that patients presenting at rural EDs with circulatory, injury, mental and symptoms diagnoses were significantly more likely to have tele-emergency department services activated as were patients who were transferred to another hospital. Interviews conducted with 85 clinicians and administrators at 26 rural hospitals that used this service indicated that this pattern of utilization facilitated rapid transfers and followed recommended clinical protocols for patients needing serious and/or urgent attention (e.g. stroke symptoms, chest pain).
Discussion
Although only used in 3.5% of ED encounters on average, our findings provide evidence that tele-emergency activation is well reasoned and related to those situations when extra expert assistance is particularly beneficial.
Introduction
Tele-emergency (tele-ED) is an electronic, two-way, audio/visual communication service between a central emergency care centre (tele-ED hub) and a distant hospital emergency department (remote ED) designed to provide real-time emergency care consultation.1,2 The hub ED clinical team often consists of a board certified emergency department (ED) physician and ED-trained nurses. In contrast, the remote ED provider is usually a primary care physician, nurse practitioner or physician assistant. Tele-ED can provide timely and high-quality emergency department services that improve rural patient care and support rural hospital staff during critical medical events.1,2
In emerging technologies, early publications often focus on the feasibility of a specific technology application or on user satisfaction with it. This is certainly the case in the telemedicine literature. 3 We recently conducted a systematic review of the tele-ED literature and found only a handful of published studies evaluating its use to connect a tele-ED hub with remote EDs for assistance with the broad spectrum of patients who present there. 1 Studies indicated that both remote ED and hub providers view consultations as improving patient care 4 and that this model of tele-ED care is comparable to traditional care in terms of patient outcomes.5,6 Compared to usual care, tele-ED has been found to reduce unnecessary transfers from remote EDs to hub EDs.4,7 Thus, the limited available research has demonstrated its feasibility and acceptance. However, we found no studies describing how often it is activated in usual practice and in what circumstances it is used. We became interested in the research question ‘under what conditions are remote ED personnel most likely to activate tele-ED?’ Data available for this study help to answer this question to further understand the value of tele-ED for rural hospitals.
Methods
Avera Health is an integrated health system, comprised of 31 owned, leased or managed hospitals, as well as clinics and other entities. The hospitals maintain separate medical staffs, bylaws and policies, but come together to develop evidence-based practices. These hospitals also share in an enterprise electronic medical record (EMR), Meditech, which links all Avera affiliated entities. Avera Health’s eEmergency programme is a tele-ED service with a hub staffed 24/7 by emergency medicine specialty physicians and registered nurses from Avera McKennan Hospital, a tertiary care hospital located in Sioux Falls, SD. This hub provides tele-ED services to remote EDs in South Dakota and seven surrounding states. The hub creates records in a tele-ED log every time the tele-ED system is activated and the log contains information specific to the tele-ED encounter (e.g. technical problems, patient disposition). The database for the current analyses was created by merging the tele-ED log data with the Meditech EMR system data. Meditech EMR data provided for these analyses involved all cases presenting with an ED encounter. These analyses focus on tele-ED cases from the period 1 November 2009 (the date of the earliest full month of tele-ED implementation) until 30 June 2012 (the date of the latest data provided for analysis). Five urban Avera Health hospitals have tele-ED implemented but use it in limited situations, often to facilitate transfers to Avera McKennan Hospital, and thus cases from these larger hospitals were excluded. Of the 51 critical access hospitals (CAHs) that had used the tele-ED service for at least six months, 21 CAHs also had the Meditech EMR system operational during this time. In these 21 CAHs, there were 60,193 total ED encounters. Of these, 1512 were ED encounters where tele-ED was activated, and 58,681 were ED encounters where tele-ED was not activated.
Nonparametric correlation analyses were used to compare hospital characteristics and rates of tele-ED activation. Logistic regression was used to model the likelihood of activation of tele-ED based on hospital characteristics, patient major diagnosis categories and patient age. Hospital characteristics examined included total ED encounters per year and total inpatient admissions per year. Patient major diagnosis categories were defined by ICD-9 CM codes. 8 Major diagnosis categories with fewer than 40 tele-ED activated cases were all aggregated into the ‘other’ category, which was used as the reference category in analyses. Major diagnosis categories with more than 40 tele-ED activated cases were circulatory, injury, mental, respiratory, symptoms and other. Chi-square test of proportions was used to assess if there was a difference in discharge destination between patients where tele-ED was activated and those where it was not activated. Logistic regression was used to model the likelihood of transfer based on activation of tele-ED and patient major diagnosis category.
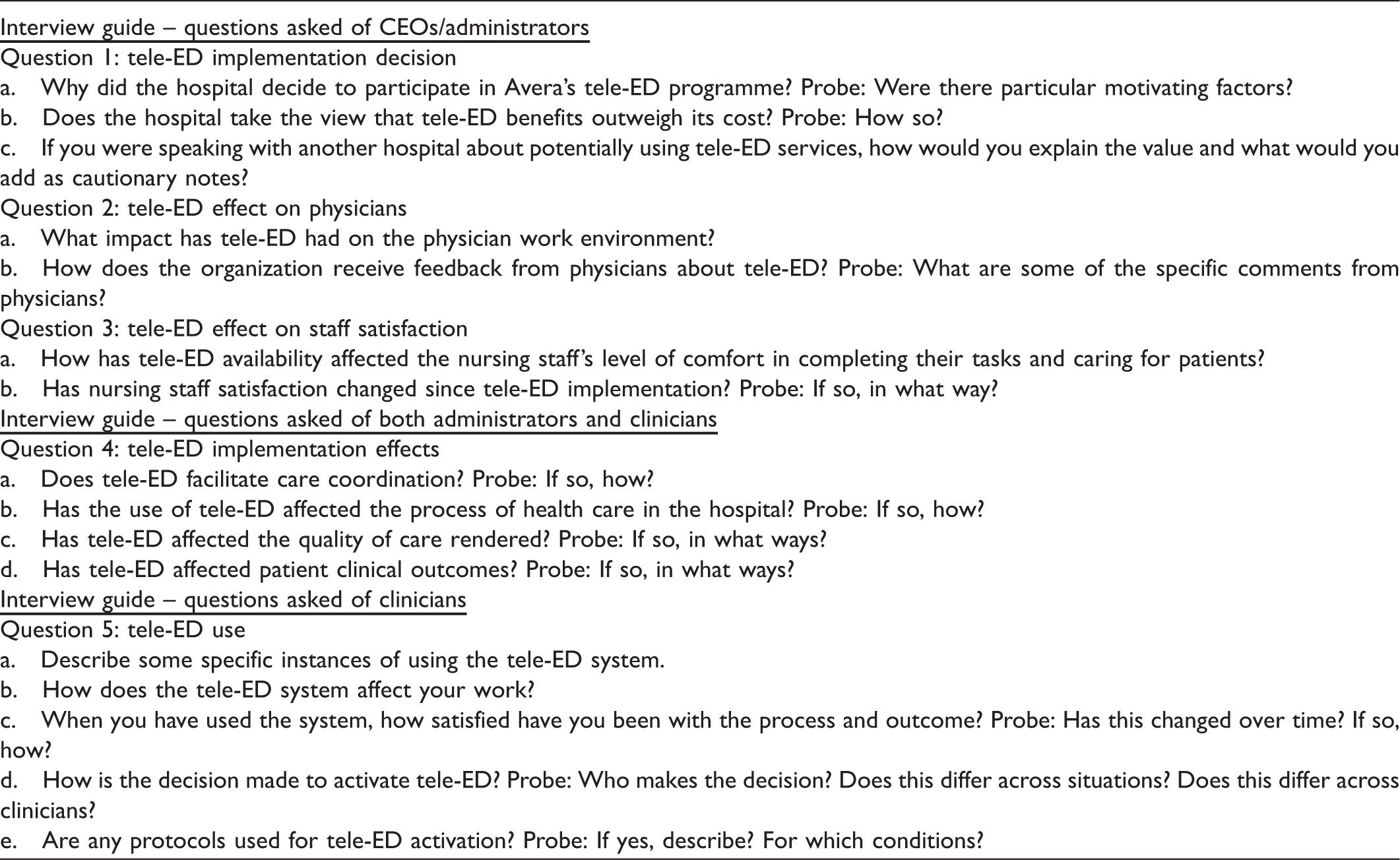
The questions asked in semi-structured interviews about tele-ED.
Results
Analyses were first conducted to examine the characteristics of the 21 CAHs using the tele-ED services. The number of staffed beds ranged from 15 to 25, with over half of the institutions having 25 staffed beds (the maximum permitted in CAHs). The number of full-time equivalent (FTE) staff ranged from 24 to 316 and averaged 113, annual admissions ranged from 112 to 1963 and averaged 502 and annual ED encounters ranged from 417 to 7633 and averaged 1957. On average, hospitals had 2.6 tele-ED encounters per month and 72.9 total ED encounters per month for an average 3.5% rate of tele-ED activation. Nonparametric (Spearman) correlation analyses found that there was no relationship between the rate of tele-ED activations and number of hospital beds or FTE staff. There was a statistically significant inverse relationship between the rate of tele-ED activation and total hospital admissions (r = –0.49, p = 0.02), total number of ED encounters (i.e. combined tele-ED and non-tele-ED encounters, r = –0.44, p = 0.04) and total ED encounters per month (r = –0.53, p = 0.01). In other words, higher tele-ED activation rates were associated with lower total admissions, total ED encounters and ED encounters/month. The rate of tele-ED activation in these hospitals did not change over time (r = 0.03, p = 0.87).
Principal discharge diagnoses and tele-ED activation.
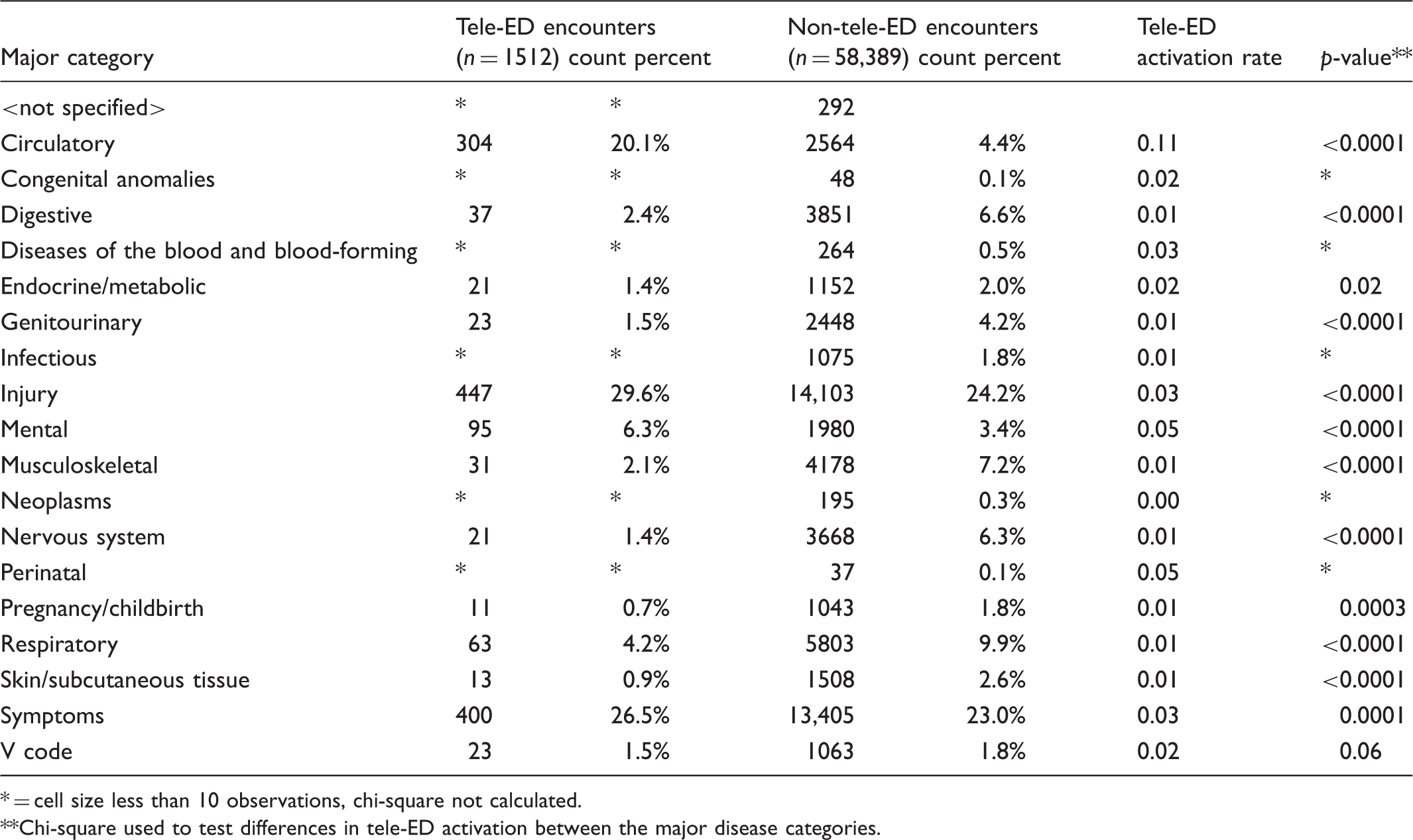
= cell size less than 10 observations, chi-square not calculated.
Chi-square used to test differences in tele-ED activation between the major disease categories.
Odds ratios of principal discharge diagnosis on activation of tele-ED, adjusted for patient age and hospital characteristics.
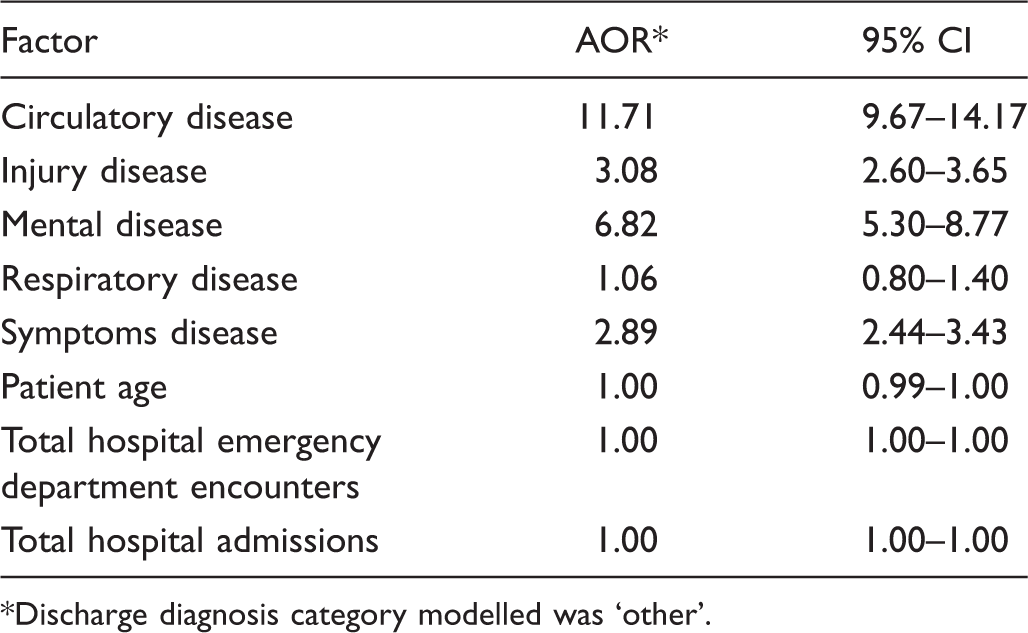
Discharge diagnosis category modelled was ‘other’.
Discharge disposition and tele-ED utilization.
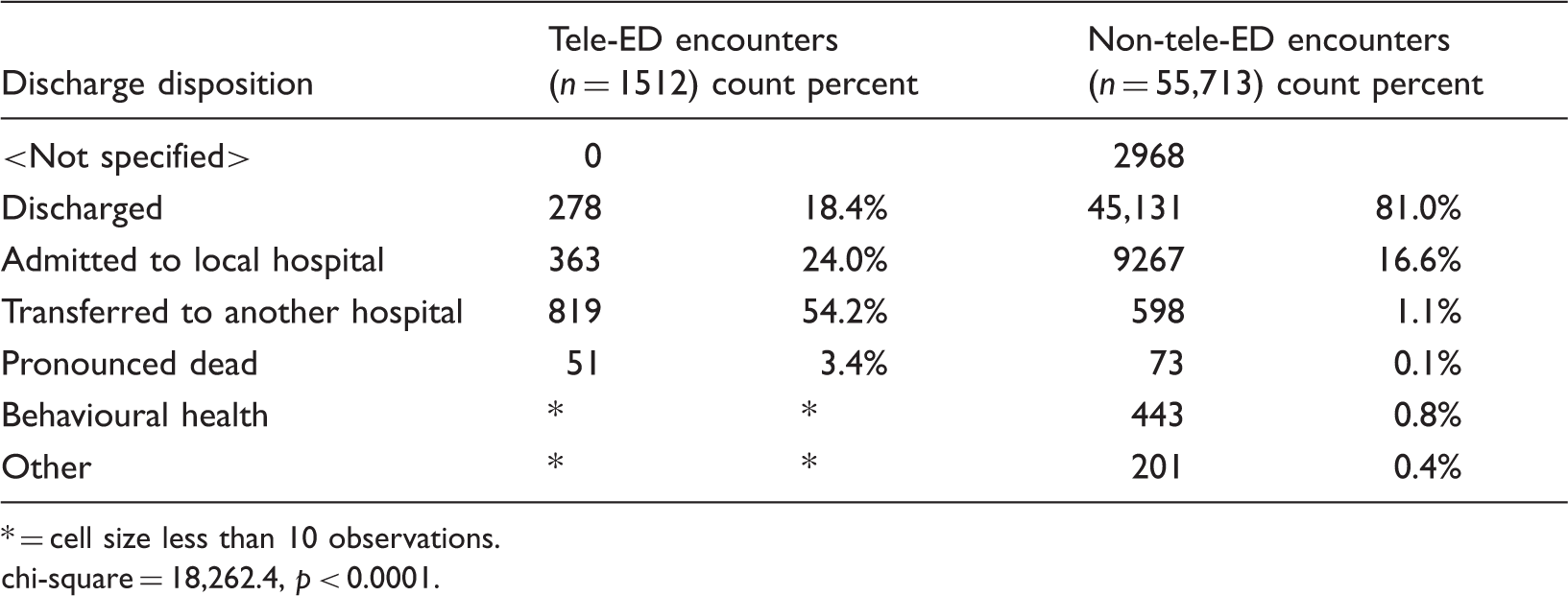
= cell size less than 10 observations.
chi-square = 18,262.4, p < 0.0001.
Encounter characteristics – discharge disposition, by diagnosis group.
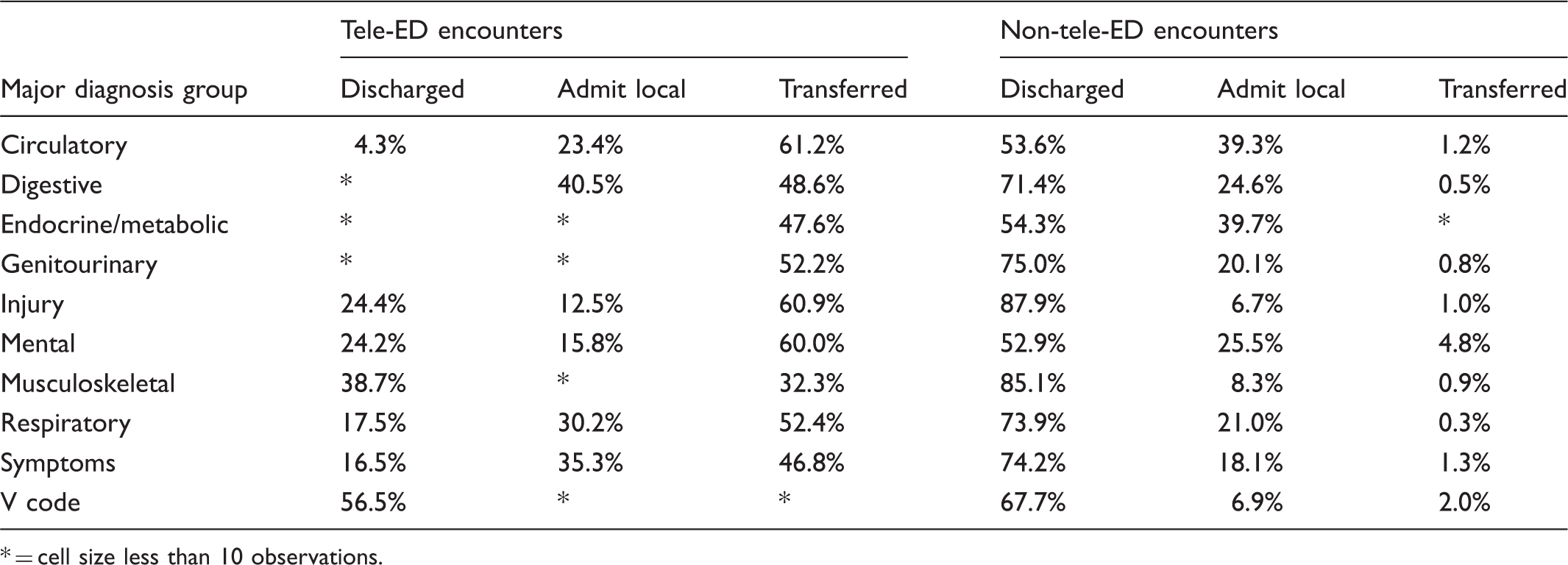
= cell size less than 10 observations.
Adjusted odds ratios of tele-ED activation and principal diagnosis on discharge disposition.
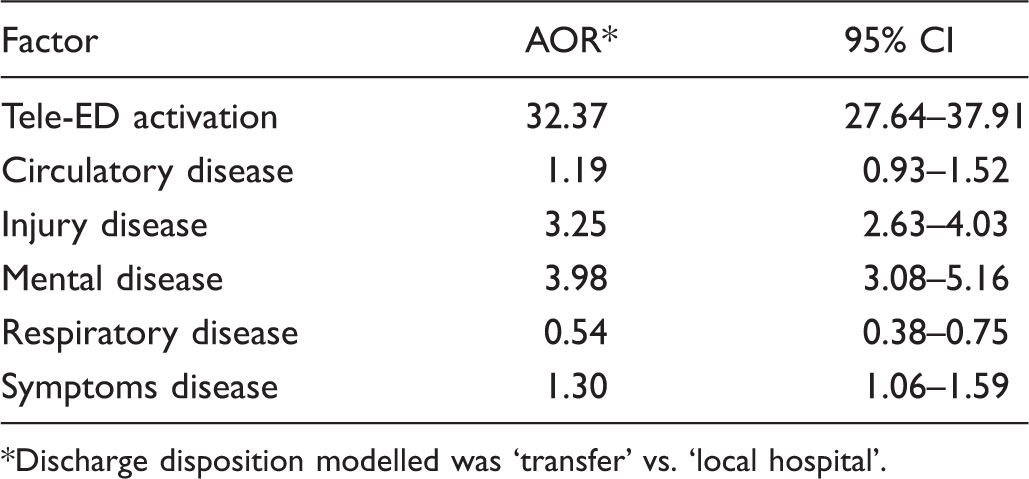
Discharge disposition modelled was ‘transfer’ vs. ‘local hospital’.
To further understand factors related to tele-ED service activation, we conducted phone interviews and site visits with 81 clinicians and administrators at 26 rural hospitals that used these tele-ED services. A qualitative inductive approach was used to identify in what situations it is used most, when and why clinicians use it or do not use it, barriers to clinicians using it, changes over time in the pattern of use and key incidents that affected its use (e.g. a particularly compelling outcome). Several themes related to tele-ED use were particularly uniformly expressed. First, interviewees were almost universal in describing how beneficial tele-ED services were to facilitate transfer when needed. Second, nurses particularly valued tele-ED hub personnel documenting care during emergent cases, relieving them to focus on patient care. Third, tele-ED hub involvement was highly valued during time-urgent critical cases such as chest pain, stroke symptoms, trauma, multiple patients needing simultaneous attention for serious injuries and while local physicians were en route to the ED. A fourth theme emerged in interviews at some but not all hospitals: that the tele-ED hub involvement was perceived as drastically improving outcomes for at least one local patient. Themes related to changes in use over time varied, with some hospital interviewees expressing immediate and continued enthusiasm and interviewees at other hospitals describing less resistance as familiarity grew and user satisfaction increased.
Discussion
The findings from the current analyses point to several situations in answer to our research question of ‘when does the tele-ED service get activated?’ First it is clear that the patient’s diagnosis is an important factor triggering tele-ED use. In particular, patients presenting at rural EDs with circulatory, injury, mental and symptoms diagnoses were significantly more likely to have tele-ED services activated. This was especially the case for patients with certain diagnoses. Specifically, tele-ED was activated for 22% of patients diagnosed with ischemic heart disease, 17% of those diagnosed with cerebrovascular disease and 18% of patients diagnosed with poisoning.
The second situation related to tele-ED activation involves the patient’s disposition. Patients for whom tele-ED was activated were much more likely to be transferred to another hospital than patients where the tele-ED system was not activated. Tele-ED encounters were also much more likely to be admitted to the local hospital than non-tele-ED encounters, who were much more likely to be discharged.
These findings suggest a conundrum involving tele-ED activation and discharge disposition. Namely, is tele-ED activated more when it appears a patient will be transferred? Or once tele-ED is activated is it more likely that the clinicians involved will determine that the patient needs to be transferred? Our quantitative data cannot definitely answer this question. However, our interview data with users of these tele-ED services illuminate some patterns. Interviewees uniformly described how beneficial tele-ED services were to facilitating transfer when needed. They described the tele-ED hub personnel coordinating all arrangements for transfer, permitting the remote ED clinical staff to maintain ‘hands-on’ care for the injured or seriously ill patient. This was especially valued because remote EDs frequently have limited clinical staff to handle critical situations such as serious trauma or multiple critically ill patients. Thus, when the remote ED clinical staff suspect that a patient needs to be transferred, they appear to activate the tele-ED service to help speed those arrangements.
The interviews also help elucidate the frequent activation of tele-ED related to certain diagnoses. ED staff are well aware of the need to urgently treat and/or transfer patients with ischemic heart disease and cerebrovascular disease. Interviewees described protocols in many remote EDs that included activation of tele-ED for all patients presenting with certain conditions. In fact, Avera Health provided guidance to remote ED personnel recommending tele-ED activation for all patients presenting with: acute head injury; advanced airway management – intubation; all resuscitations; advanced burn management; dizziness with unstable vital signs; multi system trauma evaluation and resuscitation; serious or complex medical emergencies; and shock of any etiology. While not specifically called out in this policy, it is likely that patients presenting with chest pain or possible stroke symptoms had tele-ED activated at many CAHs. Our quantitative data found that all patients diagnosed with these two conditions where tele-ED was activated were either admitted locally or transferred to another hospital, indicating that tele-ED activation occurred for patients needing serious, timely attention.
Another situation with a high rate of tele-ED activation was for patients with a mental diagnosis. When tele-ED was activated, 60% of patients with a mental diagnosis were transferred to another hospital. Multiple interviewees described valued assistance provided by tele-ED hub personnel to conduct assessments and find placements for patients needing hospital admission. This pattern illustrates the interaction between the patient’s diagnosis and discharge disposition in explaining use of tele-ED services by remote EDs.
The largest limitation of the current study is that the data do not include disease severity. Our data show that 81% of ED encounters when tele-ED is not activated were discharged from the ED rather than being admitted to a hospital. Clearly, tele-ED activation is not needed for the vast majority of ED encounters and the fact that so many were discharged is indicative of the frequent low-acuity diagnoses in ED cases. In contrast to this data limitation, a strength of the data is its generalizability to CAHs and rural hospitals nationally. The characteristics of the CAHs in this study are very similar to the national average for CAHs in terms of number of beds and staff, although the CAHs in this study average fewer ED encounters annually than the national average.10,11 The pattern of diagnoses and discharge dispositions in the current data are also similar to those nationally in the National Hospital Ambulatory Medical Care Survey-ED (NHAMCS-ED) database for rural hospitals. 12 Specifically, we compared the data in Table 2 on diagnosis categories between the non-tele-ED percentages in these CAHs and the non-metropolitan statistical area (MSA) percentages in the NHAMCS-ED data and found similar percentages. In addition, we compared the data in Table 5 on disposition categories in these two datasets and found similar percentages, with the exception that more patients presenting in Avera CAH EDs were admitted locally (16.6% vs 10.0%), with concomitantly fewer discharged or transferred (82.1% vs 88.4%). Thus, in comparing these two key variables in the current dataset with a nationally representative dataset, we believe there is evidence that the current findings on data from Avera CAHs are generalizable to patterns in EDs in rural hospitals nationally. In addition to the generalizability of the study setting, the qualitative findings are consistent with earlier studies showing that remote ED staff are satisfied with the process and interaction with the hub,4,6,13 that remote ED providers view consultations as improving patient care,4,6,14–17 that this model of tele-ED care is comparable to traditional care in terms of patient outcomes,5,6 and that it enhances patient throughput and transfers7,13 and reduces avoidable transfers. 4
Medical emergencies challenge any health care system, but more so in rural areas where time and distance to definitive health care are usually longer.18,19 Rural hospitals, especially CAHs, have few clinical staff available during emergent conditions. 20 Tele-ED services can provide invaluable support during times of emergency. 2 Although only activated in 3.5% of ED encounters on average, our findings provide evidence that tele-ED activation is well reasoned and related to those situations when extra expert assistance is particularly beneficial.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: two co-authors are employed in the health system that provided the data.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: this research was funded by a grant from The Leona M. and Harry B. Helmsley Charitable Trust (Grant #2010PG-RHC032).