
Abstract
Objective
The objective of the current study was to examine the feasibility of telemedicine vs. telephone for the delivery of a multidisciplinary weekly family-based behavioural group intervention to treat paediatric obesity delivered to families living in rural areas using a randomized controlled trial methodology.
Methods
103 rural children and their families were recruited. Feasibility measures included participant satisfaction, session attendance and retention. Treatment outcome measures included child Body Mass Index z-score (BMIz), parent BMI, 24-hour dietary recalls, accelerometer data, the child behavior checklist and the behavioral pediatrics feeding assessment scale.
Results
Participants were highly satisfied with the intervention both via telemedicine and via telephone. Completion rates were much higher than for other paediatric obesity intervention programmes, and both methodologies were highly feasible. There were no differences in telemedicine and telephone groups on primary outcomes.
Conclusion
Both telemedicine and telephone intervention appear to be feasible and acceptable methods of delivering paediatric obesity treatment to rural children.
Introduction
The prevalence and incidence of obesity in the United States remain a significant public health concern. Data from the national health and nutrition examination survey (NHANES) from 2009 to 2010 indicate that 16.9% of US children and adolescents are classified as obese (BMI ≥ 95th percentile of the BMI-for-age growth charts) and 31.8% of youth are either overweight or obese (BMI ≥ 85th percentile). 1 These prevalence rates are particularly alarming given that paediatric obesity confers significant risk on the current and future health of children.2,3
As a result, there has been an increasing emphasis on the treatment of paediatric obesity. One well-established treatment model recommended for the treatment of paediatric obesity and overweight is family-based, behavioural group programmes. 4 These programmes have been developed in an attempt to promote healthy weight and alter the trajectory of weight gain, especially among overweight youth. They focus on parents and families as agents and models of behaviour change and target improvements in diet, physical activity, and sedentary behaviour.5,6 Although these programmes have been effective at improving health outcomes among urban and suburban youth, few programmes have been developed for rural youth, and rates of paediatric obesity among this underserved group are disproportionately high.
Rural youth face unique barriers to healthy living7,8 and our own analyses indicate they have higher rates of paediatric obesity. 9 Some of these barriers include lack of nutrition education, poor access to nutritionists and other healthcare providers, limited resources, and fewer opportunities for physical exercise, which all contribute to a higher rate of obesity in this population compared to their urban counterparts. 10 Therefore, obesity treatment programmes are needed which specifically target rural youth and address factors which are unique to this group.
Interventions targeting paediatric obesity specifically among rural children are generally sparse. Some studies have been published on medical/clinical rural obesity services delivered by primary care physicians or other medical providers11,12 or on the perspectives of rural healthcare providers who are faced with the paediatric obesity epidemic. 13 Therefore, a major weakness of the current obesity literature is a lack of focus on treatment outcome among rural children.
To address this need, our team has conducted a line of research assessing the effectiveness of the use of telemedicine (i.e. interactive synchronous video telemedicine) in delivering family-based behavioural group therapy to rural families for the treatment of paediatric obesity.14,15 Although telemedicine is an extremely common method of providing distance learning in rural areas, there are still some communities that do not have this technology, or find its cost prohibitive, leaving a portion of rural children and their families with no access to these services. However, all schools in the state of Kansas do have access to a telephone, making this technology widely available. There are no studies, however, comparing telemedicine to telephone in terms of effectiveness, satisfaction or feasibility of treatment delivery, and only our own studies focus on the use of telemedicine for the delivery of Family based behavioural groups to rural families, rather than individual treatment.
Therefore, the objective of the current study was to examine the feasibility of telemedicine vs. telephone for the delivery of a multidisciplinary weekly family-based behavioural group intervention to treat paediatric obesity delivered to families living in rural areas using a randomized controlled trial methodology. We also examined treatment effects on child BMIz, nutrition, physical activity and quality of life indicators.
Methods
School recruitment
Recruitment flyers were sent to all rural elementary schools in the state of Kansas. Interested schools contacted researchers via a toll free number and their eligibility for the rural status was confirmed (city and/or county with a population of <20,000). The qualified schools identified an on-site representative for the project, who completed training in human subjects research, conflict of interest, and Health Insurance Portability and Accountability Act (HIPAA). The first 11 schools to complete these steps were recruited for the study and randomly assigned to telemedicine or telephone. Schools were provided with measurement equipment (scales, stadiometers) specifically for this project (see Measures). Randomization occurred at the school level, such that all participants from each school were assigned to a single modality. Randomization was completed by the statistician using a random numbers table. All study procedures were approved by the relevant institutional review board.
Training of on-site representatives
After being recruited, each school identified an on-site representative to be the lead of the study at that particular school. These staff members were typically a nurse, gym teacher, or computer teacher. They received project specific training regarding recruitment, consent, and intervention procedures. They were also given an intervention manual and all necessary forms, and were trained regarding the anthropometric measurement protocol, including calibration techniques and the importance of taking measurements in triplicate.
Recruitment of participants
Each school then sent recruitment letters home to their elementary students. Recruitment letters were sent home with children by school personnel to determine which families were interested in participation, and interested families signed consent forms and completed baseline measures. Inclusion criteria were: child with BMI of >85th for age/gender, family living in a rural area (city and/or county population <20,000), child attending a school with phone and internet capabilities, and the family having access to a phone. Exclusion criteria were family moving to a non-rural area, child having physical limitation or receiving an injury which significantly limited physical mobility, child having a significant medical issue, or child and parents having significant developmental delay or cognitive impairment that was known to the school. No children who met the inclusion criteria had to be excluded.
The intervention
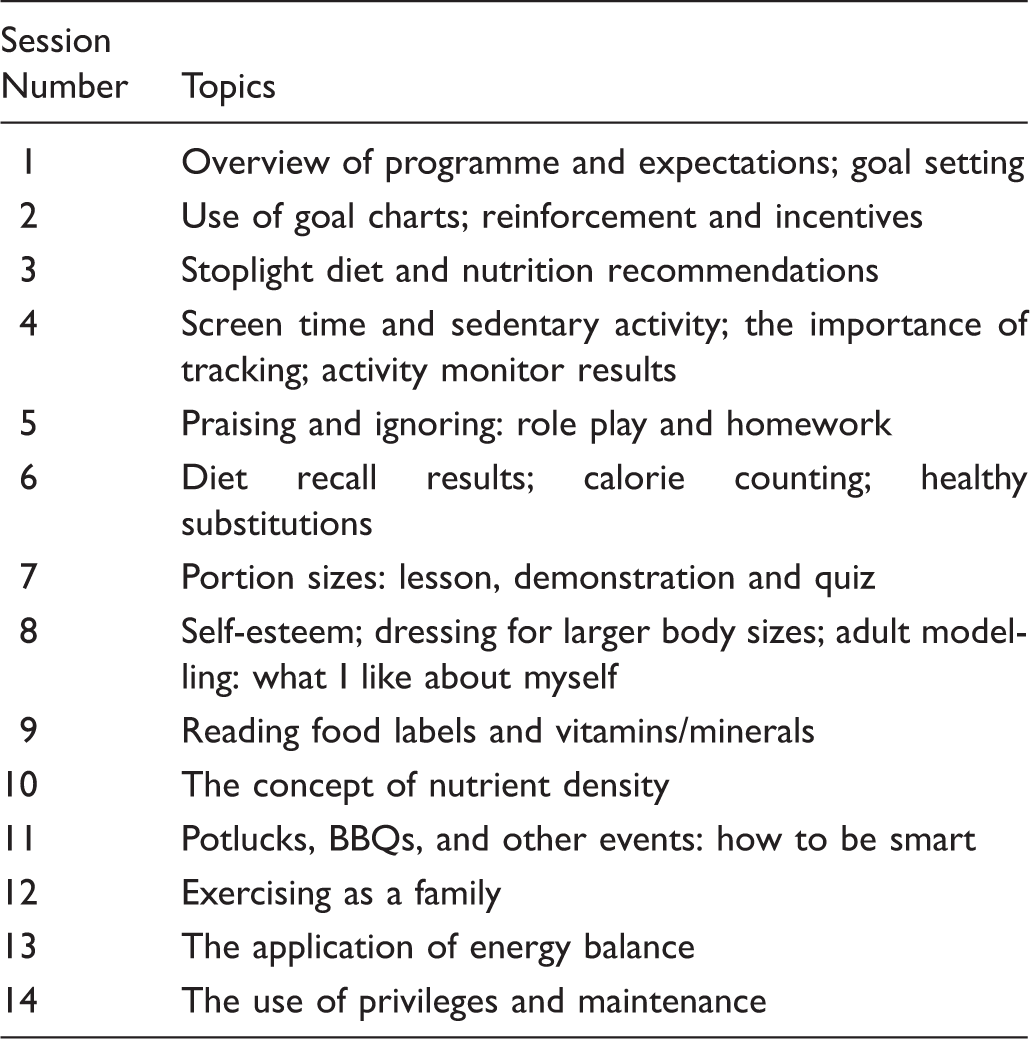
Groups were scheduled according to the convenience of the participating families and the on-site school representative (typically in the evenings). Each group session had specific objectives outlined in a treatment manual and began with a short introduction and review of weekly goals and progress led by both the off-site leader and the on-site school representative. Then, the off-site leader (a clinician member of the research team) met with the parents via the randomized modality (telemedicine, telephone), and simultaneously the on-site school representative met with the children in the next room to cover their manualized topics. All group meetings lasted approximately one hour. The parent and child groups covered the same topics, but the parent group was more didactic and the child group more activity-based.
Session topics.
Modality 1: phone
Parents and children sat around a speakerphone to communicate with the research team for all group meetings. If the school did not have an adequate speakerphone, one was provided to them.
Modality 2: telemedicine
Telemedicine (or interactive synchronous video telemedicine) allows for real time communication of audio and video. Parents and children sat around a large TV screen to communicate in real time with the research team for all group meetings. All schools were already outfitted with this technology due to their involvement with a state wide distance learning programme, which is common in rural areas/states.
Measures
All measures were completed just prior to the start of the intervention (baseline) and immediately following the eight-month intervention (post-intervention), with the exception of demographics, which were only collected at baseline. Also, child BMIz and parent BMI were collected at the eight-week time point in addition to baseline and eight months. Demographic information was self-report and included the target child's birth date, gender, grade level, and ethnicity as well as maternal and paternal age, marital status, education, occupation, and income level.
Feasibility measures
Several measures of feasibility were collected, including attendance/retention, and satisfaction (via a paper and pencil measure). For satisfaction, five items were on a scale of 1 (low) and 10 (high) and covered satisfaction with different aspects of the programme. One item was yes/no (overall, do you think this project helped your child to be healthier), and three items were open ended.
Child BMIz
Height and weight were measured by school nurses via a Harpenden Holtain stadiometer, Model 603 (Holtain, Crymych, UK) and a portable seca digital scale (seca, Hamburg, Germany). Height and weight were calculated as the average of three independent measurements and used (along with age and gender) to determine BMIz, which was used for primary outcome based upon previous similar research,17,18 and BMI percentile for children (which was used for educational purposes) based on the Center for Disease Control's (CDC) growth charts. 19
Parent BMI
Parent height and weight were measured on identical equipment using standardized procedures as mentioned above at both baseline and eight months. Parent BMI was calculated based upon the standard CDC formula. 19
24-hour dietary recall
The 24-hour diet recall is a standardized three-pass method, developed by the US Department of Agriculture for use in national dietary surveillance. This measure has been shown to be a valid and reliable representation of a child's overall diet. 20 Dietary recall data were gathered over the phone by trained Master's and PhD level researchers who were deemed reliable in diet recall procedures by a registered dietician. Prior to the phone call, parents were asked to sit with their child and write down information regarding their child's food intake regarding two weekdays and one weekend day at each time point. All dietary data were analysed using NDSR software version 2005 developed by the Nutrition Coordinating Center, University of Minnesota, Minneapolis, MN, USA. Daily intake of calories, percent calories from fat, fruit and vegetable servings, sugar-sweetened beverage servings, and servings of ‘red’ foods (foods with more than 12 grams of sugar and/or 7 grams of fat 16 ) were assessed.
Accelerometers
The ActiGraph (Actigraph LLC, Pensacola, FL) is a small, light-weight device, worn on an adjustable belt over the non-dominant hip, that measures physical activity duration and intensity. The ActiGraph has been shown to provide valid assessments of physical activity for adults and children during daily-living activities. 21 Participants were asked to wear the activity monitor for at least six hours a day for a minimum of three days during a one-week period. All data were run through Santech MeterPlus software, which accounts for age and gender cut-offs when determining moderate or vigorous activity (for specific cut-offs, see Troiano et al. 22 ). Data are reported as average minutes of moderate to vigorous activity per day.
The Child Behavior Checklist
Previous data have indicated that children with overweight/obesity are more likely to have psychological issues. 23 As the current study examined two modalities with the same intervention, we were interested in comparing outcomes on a measure of global behavioural issues, such as the child behavior checklist (CBCL). The CBCL 24 is a standardized measure that assesses parental report of child competencies and behavioural or emotional problems. Values for total score, internalizing behaviour, and externalizing behaviour were assessed.
The Behavioral Pediatrics Feeding Assessment Scale
Previous data indicate that children with overweight/obesity have higher rates of mealtime behaviour problems, 25 such as those measured by the behavioral pediatrics feeding assessment scale (BPFAS). As the current study compared a behavioural intervention delivered via telemedicine or telephone, we were interested in comparing outcomes on a measure of mealtime behaviour problems, such as the BPFAS. The measure is composed of 35 items: 25 describe the child's feeding behaviour and 10 describe parent's feelings about or strategies for dealing with eating problems. Parents are also asked to rate on a scale from 1–5 how much they agree or disagree with each statement, as well as whether or not each of the 35 items are a problem. Thus, the measure results in a child frequency score, child problem score, parent frequency score and parent problem score. Higher scores are suggestive of more problematic feeding behaviours. Previous research has shown the BPFAS to be a valid and reliable representation of a child's and parent's mealtime behaviour. 26
Obesity-related quality of life
Obesity-related quality of life was assessed via child self-report (sizing me up (SMU)) and parent-proxy report (sizing them up (STU)). Both measures were composed of 22 items each, used a four-point Likert scale, and have acceptable reliability and validity in previous studies.27,28
Results
Overview of analyses
Group comparison analyses were planned a priori and conducted by an independent statistician. To assess differences in primary outcome (BMIz) between intervention groups, the adjusted two-sample t-test was used. This statistical analysis is consistent with recommendations for the analysis of cluster randomization trials in health research. 29 To assess changes in anthropometric outcomes (child BMIz, parent BMI) by group from pre- to post-intervention, an adjusted t-test for matched pairs was used. Results are presented as mean (standard deviation) unless otherwise indicated.
Participants
Demographics of randomized sample.
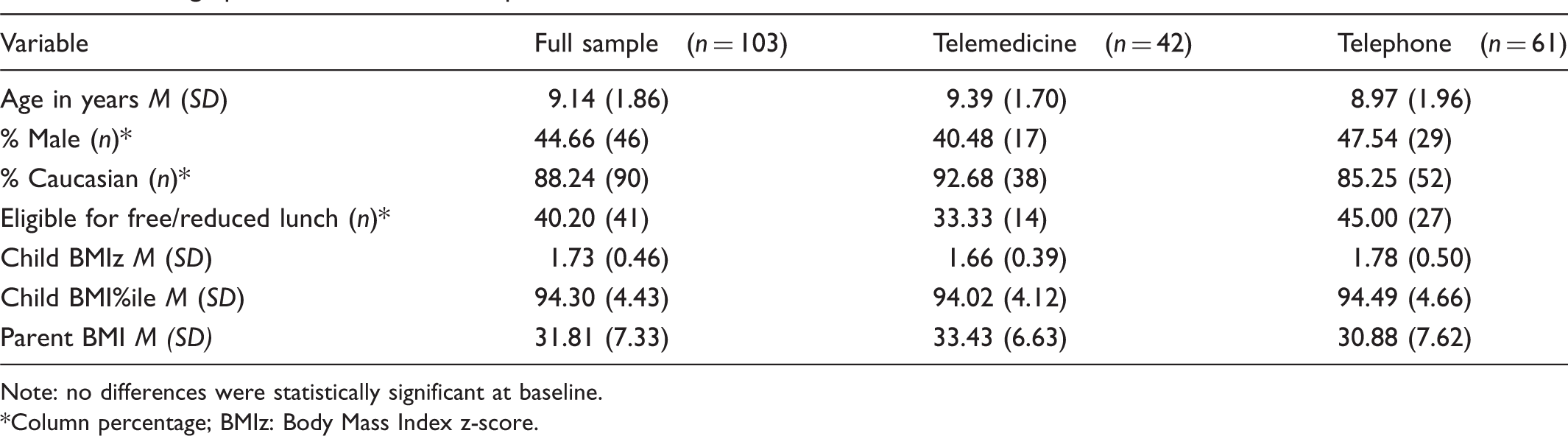
Note: no differences were statistically significant at baseline.
Column percentage; BMIz: Body Mass Index z-score.

Consolidated Standards of Reporting Trials (CONSORT) diagram.
Feasibility measures
Satisfaction
Satisfaction was rated on a 10-point scale with 10 being highest. There were no significant group differences in level of satisfaction following completion of treatment. Mean satisfaction score for the overall intervention at post-treatment was 7.77 (1.58) for the telephone group and 8.33 (1.63) for the telemedicine group. Regarding whether they found the programme helpful in facilitating the improved health of their child, 95.74% of participating parents in the telephone group responded ‘yes’ and 93.55% of the parents in the telemedicine group responded ‘yes’. Across both groups, parents were extremely satisfied with the group leaders (M = 8.93, SD = 1.55), with the handouts (M = 8.63, SD = 1.39), with the topics covered (M = 8.31, SD = 1.74) and with the degree of feedback they received during the programme (M = 8.13, SD = 1.81). When asked what parts of the programme helped the most, some representative quotes include ‘(he is) more aware… being active and has a better understanding of why we don't let him have lots of candy and sugary/fatty snacks and foods’ and ‘keeping track of what he ate, going through and seeing how much exercise it would take to burn off calories’. When asked what parts of the project they liked the most, they consistently stated the activity monitors (‘liked the activity monitors’), the dietary tracking devices suggested (‘resources for tracking dietary habits’), and the group meetings (‘getting together with others with the same problem’). When asked what could be done to improve the program, parents had many ideas, including increased contact (‘continue with the kids maybe once a month or once a quarter during school’), and increased content on certain topics (‘give more recipes’). Interestingly, several parents in the telephone group wrote spontaneous comments requesting at least one face-to-face meeting (‘have real person instead of phone call’; ‘video conferencing or at least 1 personal visit’; ‘have a real person instead of a call’, ‘make at least one face-to-face visit to make the program more meaningful’ and ‘I think for my kids anyway it would have worked better if it wasn't all done on the phone’).
Attendance
The overall attendance rate for the sample was 89.40%. No significant differences in attendance or sessions completed were found. Participants in the telephone group completed 88.41% of sessions and participants in the telemedicine group completed 90.82% of sessions.
BMI/z, diet, and physical activity measures
Changes in child BMIz.

change from pre-programme to eight months.
Child diet and physical activity change by group over time.
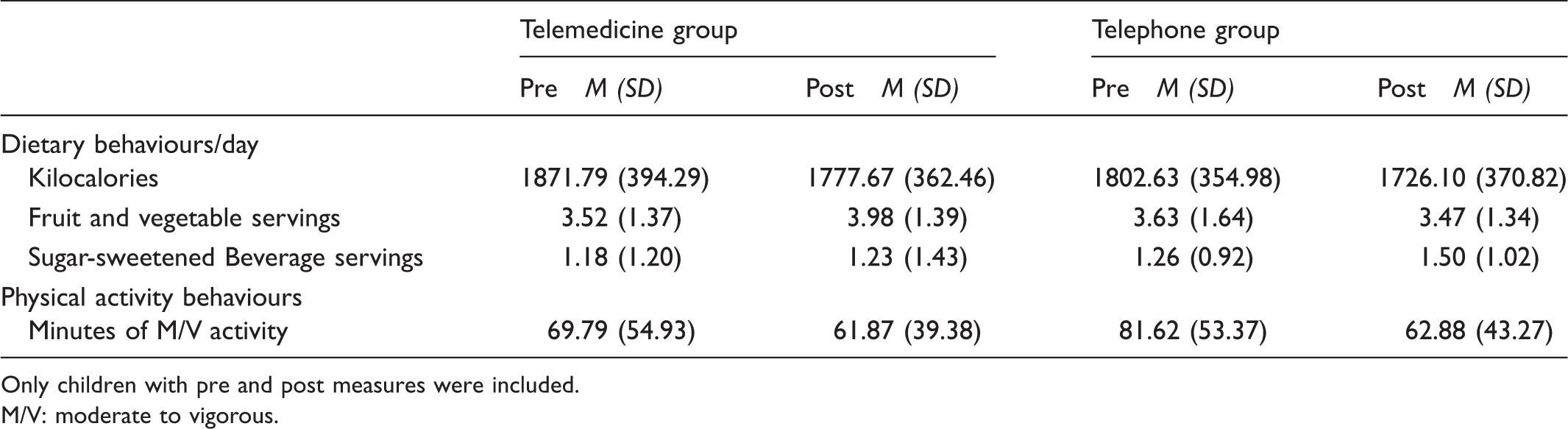
Only children with pre and post measures were included.
M/V: moderate to vigorous.
Psychological feeding and quality of life measures
There were no group by time changes from pre-treatment post-treatment for the child behavior checklist, the behavioral pediatrics feeding assessment scale, or the two measures of quality of life (sizing me up and sizing them up) (Table 4).
Discussion
The objective of the current study was to examine the feasibility of telemedicine vs. telephone for the delivery of a multidisciplinary weekly family-based behavioural group intervention to treat paediatric obesity, which was delivered to families living in rural areas using a randomized controlled trial methodology. Results overwhelmingly indicate that both modalities were feasible for the delivery of family-based behavioural group treatment to rural areas. Satisfaction was extremely high and approximately equivalent across both modalities. Parents were positive about all aspects of the programme, especially their group leaders. Open ended questions did reveal that many parents in the telephone group desired some face-to-face contact and felt that it would likely improve outcomes for their children. In terms of attrition, another of our measures of feasibility, there was slightly higher attrition in the telephone group compared to the telemedicine group, but in general, attrition from both groups was extremely low. Attrition in prior paediatric weight management interventions has ranged from 0–42% at six months post baseline and at 12–52% at 12 months. 30 Our low attrition rates (10%) could be attributed to the fact that our intervention was designed to be accessible and convenient for a rural population who often have poor access to health-related resources. 10 Even so, it is remarkable that an intervention that is only slightly effective with lowering child BMI had such low attrition, which clearly speaks to the high need for treatment programmes in these rural communities. This fits with the observations of our team members, who all reported that families were extremely grateful to be receiving such an extensive treatment programme at such a convenient location. Similar to prior studies utilizing telemedicine for paediatric weight management,15,31 no significant technological problems were noted in the telemedicine or the telephone groups.
Regarding outcome measures, there were no statistically significant differences between the two groups on any of the outcome measures. This suggests that there were no differences between the two modalities (telemedicine and telephone) on these measures. This is important because although a great number of schools have access to interactive synchronous video telemedicine equipment, there are still a significant proportion of schools that do not have access to this technology. Because the current study demonstrated that the two methodologies are approximately equivalent, future intervention dissemination efforts can use both technologies when trying to reach children in rural areas.
For both modalities, our results indicate that mean child BMIz decreased slightly (but not significantly) during active treatment (from baseline to eight weeks) and that baseline levels were maintained at eight months. These are small but meaningful changes, as research indicates that children slowing weight gain, weight maintenance, and/or weight loss should all be considered ‘successful’ outcomes in paediatric weight management. 32
It is interesting to note that parents were obese (BMI ≥ 30) at baseline, despite the fact that only child BMI percentile was an inclusion criteria. These findings corroborate previous research which indicates that parents of obese children are often obese themselves.33–36 Prior research indicates that interventions with an emphasis on parent and/or family involvement are effective for treating paediatric overweight/obesity,30,37 and may be more effective than programmes that target the child alone. 37 Parents serve as important role models for health behaviours for their children38–40 and parent weight loss has been shown to predict child weight loss in family-based interventions.41,42
Regarding dietary outcome, our results indicated that the overall number of kilocalories decreased in both intervention groups by about 100 kilocalories per day. This degree of calorie deficit is equivalent to approximately one pound per month of weight loss. Also of note, children were exceeding national recommendations United States Department of Agriculture (USDA) for 30% of calories from fat both before and after the interventions. These results are unsurprising as data indicate that for most American children approximately 30% of total energy intake comes from foods with high levels of fat and sugar. 43 Children were consuming over six red foods per day at baseline, and this only decreased slightly post-intervention. The traditional stoplight diet recommends no more than four red foods per week. 16 Although the average number of red foods decreased in both groups on average between baseline and follow-up, the average number of sugar-sweetened beverages increased in both groups. Prior research has indicated a connection between daily servings of sugar-sweetened beverages and BMI, particularly in girls.44–46 Children were also far below the national recommendation of five servings of fruits and vegetables a day both before and after the interventions. 47 Although several of our nutrition related behaviours trended in the expected direction, results clearly indicate the need for more effective intervention components related to nutrition behaviour change that would enable participants to meet the national nutritional guidelines.
Our results regarding physical activity indicated that the child participants were quite active on average both pre- and post-intervention. Children in both groups met the national recommendation of 60 minutes of moderate to vigorous physical activity per day at all time points. 48 Considering that prior research has indicated that only 42% of children age 6–11 meet the recommendations for 60 minutes of moderate to vigorous physical activity, 22 the children in our study were quite active.
Results from the CBCL indicate that children were psychologically healthy at baseline in both groups, and remained psychologically healthy at post, with no significant differences in outcomes by group. CBCL scores obtained in the current study were lower (more healthy) than those obtained from other studies of urban and suburban children with higher degrees of obesity.49,50 Overall, prior research has indicated that children who are obese are significantly more likely than typical weight peers to have psychosocial problems, such as low self-esteem, depression, body dissatisfaction, loss-of-control eating, dissatisfaction, and decreased health-related quality of life. 51 Thus, future research should assess why findings between rural and urban overweight and obese children seem to differ with regard to child psychopathology.
Results from the BPFAS, which is designed to assess mealtime behaviours, indicate that the children and parents in both groups did demonstrate some mealtime behaviour difficulties at baseline, and that these problems decreased slightly in both intervention groups, suggesting that our interventions may improve mealtime behaviours in this population. Prospective studies have indicated that problematic eating behaviours early in life may be a risk factor for overweight and obesity in childhood.25,52 One cross-sectional study found that parents of overweight and obese children are more likely to report problematic mealtime behaviours than parents of children with a normal weight. 53 Overall, there is a lack of research investigating mealtime behaviours in children with overweight/obesity using measures that have been validated for use with this population.
Results for quality of life indicated that our sample had a high (healthy) quality of life at baseline, and that this value remained high at post-intervention. This was true for both parent reported and child self-reported quality of life. Previous research on these measures with treatment seeking overweight and obese paediatric populations indicates scores ranging from the mid-50s to the mid-70s on the five subscales across both the parent report and child report forms. 54 For the current study, however, our mean scores were primarily in the 80s for both parent and child report, indicating that rural status may somehow protect weight-related quality of life among treatment-seeking overweight and obese youth. However, a relatively recent study assessing the reliability and the validity of ‘sizing me up’ (the child self-report measure) with a community-based non-treatment-seeking sample found scores very similar to our own. 55
The clinical implications of this study are many. First, for rural families facing the issue of paediatric obesity, both the telemedicine and telephone methods appear to be feasible for the delivery of empirically supported interventions. Both of these intervention modalities are highly scalable and would allow for the treatment of a large number of families without the inconveniences of travel time or cost – an important clinical implication. Families from rural areas who commit to this type of intervention are likely to show up for treatment, be satisfied with the treatment, and to encounter few technical difficulties. Children who participate are also likely to improve at least some of their health behaviours and to maintain their body mass, as are parents (which argues for including them in the intervention programme). However, data also clearly indicate that the rural intervention needs to be improved if it is going to result in meaningful body mass changes for children. Potential strategies to do this could include increased monitoring accountability between the family and the group leader. In our face-to-face programmes with urban children 56 we spend a great deal of time reviewing monitoring forms kept by the families each week. However, doing this remotely proved to be a challenge.
Limitations
This study does have several limitations. First, our sample was relatively small, a common problem encountered in rural studies. All participants were from rural areas in only one state, so our findings may not generalize to rural areas in other states. Related to this, our sample was predominantly Caucasian, but this was reflective of the population from which the sample was drawn and therefore expected. Also, some of our measures (CBCL, BPFAS) were not obesity specific, which would likely have strengthened our study.
Conclusion
In summary, the current study addresses the key health issue of paediatric obesity among an underserved rural population, examining the effectiveness of family-based behavioural groups delivered via telemedicine or telephone. Results indicate no statistically significant differences between modality (telemedicine/telephone) and also suggest trends toward desirable changes in anthropometrics and health behaviours. The fact that our families achieved body weight/mass maintenance is important to note, as successful treatment of paediatric obesity is not necessarily measured only in terms of weight loss. Also, our high satisfaction ratings and notably low attrition indicates that a group-based, remotely-administered health behaviour intervention – as opposed to individual, in-person sessions, which have limited feasibility for rural populations – allowed families to feel sufficiently ‘connected’ that they remained committed to our eight-month programme, representing an important opportunity for enhanced dissemination of similar programmes. Future research will need to examine these findings with larger and more diverse samples, and to determine specific methods to increase treatment effects. Current national data indicate that 83% of all homes have internet access 57 and that 58% of children aged three to 17 use the internet at home, 58 making a home based telemedicine intervention programme particularly interesting for addressing these limitations.
Footnotes
Acknowledgements
We also wish to thank all of the wonderful families who participated, and the rural schools who were excellent partners in this important work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: funding from the National Institutes of Health (NIDDK 081016).