
Abstract
Introduction
We investigated the experience of individuals diagnosed with type 2 diabetes mellitus (T2DM) who participated in an intervention in which the key elements were the provision of a smartphone and self-monitoring software. The interviews focused on use of a smartphone and the effects on motivation for health behavior change.
Methods
This was a qualitative evaluation of participants in a larger T2DM self-management randomized controlled trial (RCT) conducted at the Black Creek Community Health Centre (BCCHC) in Toronto, Canada (ClinicalTrials.gov Identifier: NCT02036892). The study is based on semi-structured interviews (n = 11) that were audio taped and analyzed with a thematic analytic approach. The RCT compared the effectiveness of six months of smartphone-based self-monitoring and health coaching with a control group who received health coaching without internet or smartphone-based assistance.
Results
Qualitative data analyses resulted in derivation of four major themes that describe participant experience: (a) ‘smartphone and software’, describes smartphone use in relation to health behavior change; (b) ‘health coach’ describes how client/health coach relationships were assisted by smartphone use; (c) ‘overall experience’ describes perceptions of the overall intervention; and (d) ‘frustrations in managing chronic conditions’ describes difficulties with the complexities of T2DM management from a patient perspective.
Discussion
Findings suggest that interventions with T2DM assisted by smartphone software and health coaches actively engage individuals in improved hemoglobin A1c (HbA1c) control.
Keywords
Introduction
The prevalence of type 2 diabetes mellitus (T2DM) is predicted to increase to 33% by 2050 while Canada already spends C$25 billion annually on diabetes care.1,2 Similar immediate and projected costs have been identified in most developed countries, establishing the importance of effective T2DM management in reducing financial and human burdens. Several researchers have found that smartphone self-monitoring paired with health coaching is associated with improved glucose regulation,3–7 dietary control 8 and medication adherence. 9 Such interventions appear customizable to multiple ethnicities and socioeconomic strata (SES) 10 as indicated in a pilot trial (Wayne and Ritvo, 2014) where a diverse SES population with hemoglobin A1c (HbA1c) levels > 7.0% demonstrated clinically significant reductions (p = 0.04).11
The promise of smartphone-based monitoring is to optimize the patient’s time outside of treatment, by motivating improved glycemic control at modest costs. This combination was demonstrated in a mobile phone health coaching intervention that increased glycemic control (p = 0.01) and patient satisfaction (p = 0.04), while saving 8.8% in net treatment costs. 7
The most precise quantitative assessments of smartphone-based health coaching must be derived through randomized controlled trials (RCTs), but RCTs only produce modest levels of patient feedback. We recently completed an RCT and, to provide more in depth feedback, undertook semi-structured interviews with n = 11 intervention participants.
In this study, we follow qualitative studies where T2DM patients were interviewed after a health coaching intervention with education, peer support, and coaching frequency determined by adherence level re: target behaviors. Participants described health coaches as effectively assisting with more autonomous and confident self-management. 10
In the practice of health coaching, questions remain about how it differs from other counselling approaches and what intensity and duration result in stable, long-term benefits. A recent cluster randomized trial evaluated telephone-based health coaching in general medical practices (n = 59) in Victoria, Australia with poorly managed T2DM patients (n = 473). 12 Based on two days of training with a general practice nurse, the health coaches delivered a median of four coaching sessions/participant over 18 months, averaging 30 min/session. Trial results showed no significant between-group differences in health outcomes (HbA1c, lipid profile, weight and psychometrics) 12 possibly due to inadequate intervention intensity (i.e. too little training and/or too few sessions). Similar factors might explain negative findings associated with telephone-based health coaching services with patients (n = 2698) with cardiorespiratory illness. Contrary to objectives, researchers found increases in hospital admissions, hospital use, and intervention costs in subjects vs. matched controls, 13 again employing low levels of intervention intensity, (between 2–4 contacts monthly and one telephone call per three months).
The trial we report on followed a more intensive protocol than the two studies just described, with smartphone and health coach contacts summating to one hour of contact weekly per patient. Training and supervision were also more intense as health coaches received continuous supervision throughout the trial, totaling 100 hrs. per coach, delivered by a registered clinical psychologist (PR). These intensity titration data are intended to contribute to the literature on how much smartphone and counseling interactions are needed for significant and sustainable benefits.
Methods
Study design
This qualitative evaluation was part of a larger T2DM self-management RCT (2011–2015) (ClinicalTrials.gov Identifier: NCT02036892) undertaken at the Black Creek Community Health Centre (BCCHC) in Toronto, Canada. The objective was to compare the effectiveness of six months of smartphone use with health coaching vs health coaching of equal intensity without smartphone support. The smartphone software used (Connected Wellness Platform) was provided by NexJ Systems, Inc. Using in person, semi-structured interviews following study completion, participants reflected on their smartphone-based experiences in relation to the role of the health coach in the enhanced intervention arm. Interviews (approx. 30–40 min.) were conducted by a trained interviewer, and reviewed by two additional members of the research team to ensure standardized technique.
Setting and participants
The study site (BCCHC) is located in a lower income neighborhood of Toronto, and employs an interdisciplinary team of medical and social service providers. The BCCHC catchment area serves a high proportion of recent immigrants from ethnic minority backgrounds. After completing the trial, individuals were invited by phone or in person to participate in qualitative face to face interviews. Efforts were made to reach n = 26 intervention participants, and n = 11 were contacted. All the participants who were reached were invited and they agreed to participate in the study. Overall, the n = 11 subjects included two males (mean age = 63.5 ± 4.9) and nine females (mean age = 55.8 ± 8.8) from a wide range of socioeconomic backgrounds.
Ethical approval
This study received ethical approval from York University’s Human Participants Review Subcommittee (HPRC) and all participants provided informed consent. To maintain confidentiality, personal information was removed from transcripts and audio interview recordings were stored in a locked cabinet in locked offices. Transcripts were transferred between locked password protected computers, with encrypted USB Keys.
Interview collection and analysis
Interview questions were developed by the lead investigator (PR) from prior research and modified by other team members (SP and NW) (Appendix 1). Interviews were conducted (SP), transcribed verbatim (SP), and reviewed for accuracy by the entire investigative team (FA, NW, PR, SP). Saturation–the point where no new information is detected with additional interviews–was evaluated and agreed on by all research team members, in accord with study goals. 14
Coding and analyses were performed using NVivo (v. 10; QSR International) employing a thematic analytic approach15,16 that thoroughly explored relevant themes surfacing during the interviews. Thematic analysis provides a systematic identification of emergent patterns, and logically organizes qualitative data into broader common and representative themes. 15 Our analytic strategy of constant comparison included code development (SP and FA) as the basic analytic unit (capturing important aspects of data) and, based on codes, the derivation of broader themes (team discussions) illustrating a coherent view of collected data. 15 All participant perspectives and T2DM self-management experiences were explored in the context of changes in HbA1c levels, a reliable index of long-term glucose control. 17
Results
Thematic analysis identified four major themes: ‘smartphone and software' pertained to phone utility and self-activation through awareness, feedback, self-management and monitoring. The ‘health coach' theme focused on participant experiences with smartphone interactions in relation to perceived health coach qualities, roles and influences on diet, blood glucose monitoring and exercise. The additional two themes were ‘overall experience' (of program) and ‘frustrations managing chronic conditions'.
Theme 1: Smartphone and software
Discussions focused on (a) smartphone utility, or direct use in behavioral tracking with the smartphone, and (b) self activation, or processes related to personal monitoring, feedback, awareness and self-management.
Smartphone utility
Participants discussed exercise tracking, food tracking (via photo journaling), health coach communication and self-generated/coach-generated reminders. Individuals emphasized the benefits of self-monitoring changes in blood glucose, diet and exercise. ‘I liked sending all the information to my health coach. I didn't have to tell her' (Participant #11 – change in HbA1c: –2.0%).
Participants viewed meal photographing as conveying helpful dietary feedback. Co-monitoring with the health coach was helpful in modifying portions. ‘I could just take a picture … a visual record of what I have eaten' (Participant #1 – change in HbA1c: –0.6%).
Applications were viewed as user friendly, although most participants had never used a smartphone that enabled behavior tracking and feedback. Some participants described learning to use the system as a challenge, while others found it easy from the start. ‘It was not hard to use, the health coach explained everything' (Participant #7 – change in HbA1c: –1.7%).
Reminder messages could be programmed to appear on the patient’s smartphone at predetermined times, a function that was appreciated by several participants. ‘It was a helpful reminder of keeping a check on my blood … what I eat … what I shouldn’t' (Participant #4 – change in HbA1c: –1.1%).
Self activation
Processes identified by participants and associated with self-activation were: self-awareness, feedback, and self-management. The smartphone increased self-awareness of habitual behaviors, especially dietary choices. Having pictures of their food increased awareness of portion size and carbohydrate intake. The application also helped them connect blood sugar levels to food choice.
Participants identified the feedback as motivating. When participants shared meal photographs, they received immediate feedback from coaches on where improvements could be made.
The smartphone supported self-management and monitoring, as individuals monitored patterns of behaviors, giving them a chance to ‘think twice’ about consumption. ‘I eat, I take the picture, and then … I poke myself … how high the sugar is … ' (Participant #7 – change in HbA1c: –1.7%).
Theme 2: The health coach
All participants shared positive experiences about their smartphone interactions with health coaches, emphasizing the understanding and encouragement received in the behavior change process. Analysis of discussions revealed four subthemes: (a) overall qualities; (b) supportive role; (c) working together; and (d) focal contact activities.
Overall health coach qualities
Various descriptions of the health coach included: strong, meticulous, confident, responsible, respectful and hardworking, especially in terms of monitoring and providing feedback. Appreciation was expressed in multiple forms, with representative descriptors being: best, nice, positive, generous, supportive, helpful and dedicated. ‘Very persistent (with) monitoring what I have been eating … as soon as I sent a picture they would call back immediately' (Participant #5 – change in HbA1c: +0.5%).
Health coach supportive role
Individuals described health coach support as having someone ‘always by their side’. This helped reduce feelings of isolation and being misunderstood. Trust was important in relationship strengthening as individuals discussed their diabetes management but also felt comfortable discussing personal struggles. ‘I think this study helped me emotionally a lot, more than physical, I feel emotionally happy. That is important to me' (Participant #9 – change in HbA1c: –0.4%).
Working together
Good listening skills were mentioned by participants who felt ‘being heard’ by the health coach built trust and therapeutic alliance. Their logged behaviors on the smartphone provided the ability for participants and health coaches to communicate by phone and in person. This feedback was perceived valuable in meeting personal goals. For example, a photo-journalled meal allowed participants to pause, think, and communicate with the coach. On the health coach side, there could be reference to specific food pictures, specific blood glucose readings and specific exercise sessions; a strong tie appeared to develop in relation to program specific activities (diet, exercise, glucose monitoring, medication). ‘We talk about everything that is going on in my life. What happened? why is (my sugar) … a little bit higher (or) lower' (Participant #11 – change in HbA1c: –2.0%).
Some participants became more critical of their own behaviors related to food and exercise in ways that served productive discussions. Participants were activated by the co-monitoring with health coaches who were perceived as always watching (despite not being physically present) which increased the client’s feelings of accountability to follow through with change. It was like the doctor looking at you. I have to do this, I have to test my blood sugar, I have to test my pressure, how much exercise … . Your meal, what you eat … you have this eye looking at you on the phone (Participant #6 – change in HbA1c: +0.1%).
A few participants felt uncomfortable at the start because someone was ‘watching’ their diet and blood glucose levels via smartphone. With time they realized benefits and became comfortable with health coach observation. ‘(Smartphone) was my watcher. Somebody is watching you through your eyes … it was so interesting' (Participant #9 – change in HbA1c: –0.4%).
Focal activities
All participants agreed that the health coach assisted with diet, glucose testing, medication, and exercise. Individuals also discussed more specific ways in which their coach helped improve their self-management.
In terms of diet, individuals worked on portion control, monitoring carbohydrate intake and ethnic specific food choices. Participants described how health coaches addressed various domains of diet, such as amounts/types of food consumed in routine and celebrative situations. ‘She teach me how to eat, what I had to eat' (Participant #3 – change in HbA1c: –7.1%).
On the issue of medication, few subjects spoke in detail, explaining that medications were mostly discussed with their health coach at the start and thereafter the main emphasis was on healthy behaviors. ‘We never discussed medication, I let (the health coach) know what I was taking, and brought them in' (Participant #5 – change in HbA1c: +0.5%).
All participants discussed blood glucose monitoring. Their conversations included daily glucose readings and insights on using food and exercise logs for interpretation. ‘(If) my sugar (is) high, (health coach) will explain … there can be things to eat or something to drink to make sure it's okay' (Participant #2 – change in HbA1c: –2.0%).
Exercise was also part of participant conversations with health coaches, who encouraged participants by teaching techniques tailored to individual preferences and needs. ‘The exercise was an important part of the treatment, so (the health coach) was very aware that I'm doing the right exercise, how many times, (Participant #10 – change in HbA1c: +0.2%).
Theme 3: Overall experience
Overall experience highlights factors that influenced participants after intervention completion. This theme reflects what participants ‘took away’ from the program. They described increased control and confidence in dealing with their condition and a substantial gain of knowledge about diabetes management. ‘When I first came here … I was in really bad shape. [My] sugar was very high. The A1c was high … ' (Participant #11 – change in HbA1c: –2.0%).
When discussing the program, participants described it as helpful and were motivated to participate in other programs where financial costs and burdens were nonexistent. ‘The program is a big motivation in my life … it’s a positive thing for me … with all that’s going on I need positive things' (Participant #6 – Change in HbA1c: +0.1%).
Theme 4: Frustrations in managing chronic conditions
Participants expressed frustrations in managing chronic conditions with a particular focus on: (a) medication and blood glucose; (b) diet/weight; and (c) comorbidities. These points emerged as challenges, although they existed prior to joining the program.
Medication and glucose measurement
Both injection and oral medication were noted as a combined adherence challenge and the self-administration of multiple medications was deemed frustrating. There was a common pattern of aversion to medications, as well as honest disclosures of adherence lapses. ‘I used to feel weak. [medication] is helpful, but to be honest, I don’t take it' (Participant #7 – change in HbA1c: –1.7%).
Participants were further frustrated by having to check blood sugar levels in relation to medications and were not often confident their regulation was accurately reflected in readings, ‘My sugar was sky high … I would eat half a sandwich and my sugar would double to 22 [mmol/l]' (Participant #8 – change in HbA1c: –1.1%).
Diet/weight loss
Participants struggled with modifications in diet and with weight loss goals, specifically mentioning cooking practices and diet restrictions, and their impact on family members. ‘Doctor just wants you to eat leaves and egg whites; I couldn’t handle it' (Participant #8 – change in HbA1c: –1.1%).
Comorbidities
Individuals suffered comorbidities (e.g. chronic pain, mental health difficulties, hypertension) further hindering diabetes management. ‘I have type 2 diabetes, high cholesterol, macular degeneration, and carpal tunnel. I have a lot on my plate' (Participant #6 – change in HbA1c: +0.1%).
Discussion
This study described experiences of T2DM patients enrolled in a RCT that assessed a health coaching intervention that used smartphone software to aid the tracking of health indices, emphasizing self-management. We intended to expand knowledge on how patients with T2DM interpreted the role of a health coach and the use of health tracking software. It is notable that the health coaches were highly regarded by subjects who used positive adjectives (nice, positive, generous, supportive, helpful, hardworking, persistent) in descriptions. We interpret these findings as reflecting the positive therapeutic alliance that was established with the assistance of smartphone support. Therapeutic alliance, developed in smartphone interactions that involved multiple channels of contact, was emphasized in supervision and training; its development was linked to a supportive, non-confrontational approach.
Findings suggest that the smartphone-based behavior monitoring software helped individuals track behavior and communicate with their health coach, and, generally, adopt an active role in improving health. In contrast to studies where intervention technologies are perceived to have effects independent of personal contact between providers and patients, our results suggest the smartphone self-monitoring software enhanced the relationship with the health coach.
Furthermore, in the themes emerging from qualitative analyses, there was clear evidence that the overall intervention was most effective when software use was optimally coordinated with personalized health coaching interactions. This was especially evident in output linking perceptions of smartphone use with perceptions of health coach behavior in a mutual feedback system. The positive impact of the smartphone tracking appeared enhanced by health coaching, while, reciprocally, positive coach interactions were enhanced by smartphone tracking.
Subjects Changes in Hemoglobin A1c (HbA1c).
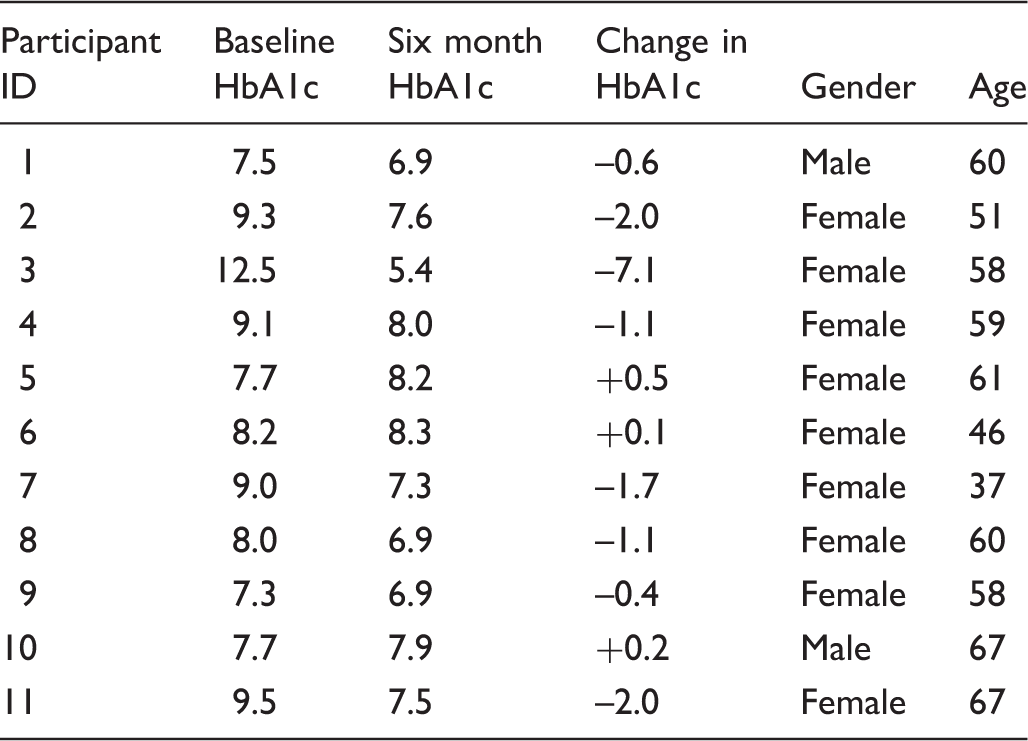
Participants in this subsample had a clinically significant mean HbA1c reduction (–1.38%, standard deviation (SD) = 2.08). However, positive views of smartphone functionality were expressed by individuals who did not achieve significant benefits, either in terms of glucose regulation or personal support, and negative views were expressed by individuals who demonstrated considerable benefits (in each area). These findings provide some confirmation that participants were not biased by their overall glucose regulation.
As indicated previously, controversy in this new field of health coaching revolves around the intensity required to achieve benefits, with intensity often referenced as the duration/frequency of coach/client contacts and the duration/frequency of coach training.11,12 There is also variety in terms of the health coaching approach selected.3–12 As intensity directly maps onto intervention costs, it is instructive for trials to demonstrate the relative benefits of lesser vs. greater intensity levels. In this trial, the focus was on coaching with continuous smartphone monitoring compared with equivalent contact between coach and subject without smartphone use. The intensity range was purposefully set at a relatively high level to explore optimal intensity per subject (in relation to results achieved).
Quite apart from what frequently occurs in psychotherapeutic interventions, subjects rarely demanded more time from health coaches than deemed appropriate (by coaches). This finding is notable given no exclusions of subjects due to psychiatric diagnosis. Also, we did not restrict discussions between health coaches and subjects. Instead, discussions included psychological contexts on how the participant was managing life stressors which often affected how he/she could engage in adopting/adhering to health related behaviors.
A key interactive feature was the 24 hour/7 day per week ‘tether’ maintained via the electronic client/coach co-monitoring. In their own words, despite the distance between them, clients never felt alone on their journey to improve health. With real time mutual access to health monitoring data, there were few interactions where the participant could express frustration without the implicit obligation to self-mobilize. Thus there was minimal cognitive space for participants to imagine the health coach helping that did not also involve their own self-activation. Even when the health coach led the subject in personal exercise sessions, directly or electronically, the subject focused on ‘doing’ rather than solely discussing.
Smartphone connectivity represents a new context for precise health intervention as each client/coach contact leaves a digital record describing what was done and not done. While digital data analyses require participants to use smartphones with some frequency, intensity of smartphone/software use, itself, provides information related to benefit. In another study, we use data mining tools to quantitatively explore tracker use in relation to benefit. As in the current study, we are intent on understanding subgroups and their specific intervention experiences.
There were study limitations common to all qualitatively oriented investigations. The specificity of verbal reports cannot be equated with quantitative outcomes, nor with mechanisms that explain associations between experience and outcome. Nonetheless, the qualitative approach provides a detailed perspective on what some participants experienced during interventions. These participants are, of course, were willing to participate in two studies (the RCT and this interview study), which may differentiate them from other participants whose blood sugars were significantly dysregulated. In future studies, it may be possible to identify and recruit additional groups of patients and in doing so, derive results more representative of the general population of diagnosed patients.
Conclusion
In this qualitative study, it is evident that the smartphone monitoring software substantially enhanced the therapeutic alliance with patients who held their intervening coaches in high regard. Future studies can address how smartphone use enhances relationships and how different intensities and approaches to health coaching integrate effectively with smartphone use.
Footnotes
Acknowledgements
The authors would like to acknowledge the generous collaboration of Jean Fraser, Fred Franco, Neil Gillman and Ashley Maurer who served as health coaches (with S. Pludwinski and N. Wayne). We were greatly assisted by the supportive expertise of Michelle Westin, Manager of the Diabetes Education Program, Cheryl Prescod, Executive Director, and Dr. Howard Ho, at the Black Creek Community Health Centre in Toronto, Ontario.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided by the Public Health Agency of Canada and the Federal Development Agency of Southern Ontario.