
Abstract
Objective
The objective of this research is to determine the effects of mobile telehealth (MTH) on glycosylated haemoglobin (HbA1c) and other clinical and patient-reported outcomes in insulin-requiring people with diabetes.
Methods
A nine-month randomised, controlled trial compared standard care to standard care supplemented with MTH (self-monitoring, mobile-phone data transmissions, graphical and nurse-initiated feedback, and educational calls). Clinical (HbA1c, blood pressure, daily insulin dose, diabetes outpatient appointments (DOAs)) and questionnaire data (health-related quality of life, depression, anxiety) were collected. Mean group changes over time were compared using hierarchical linear models and Mann-Whitney tests.
Results
Eighty-one participants with a baseline HbA1c of 8.98% ± 1.82 were randomised to the intervention (n = 45) and standard care (n = 36). The Group by Time effect revealed MTH did not significantly influence HbA1c (p = 0.228), but p values were borderline significant for blood pressure (p = 0.054) and mental-health related quality of life (p = 0.057). Examination of effect sizes and 95% confidence intervals for mean group differences at nine months supported the existence of a protective effect of MTH on mental health-related quality of life as well as depression. None of the other measured outcomes were found to be affected by the MTH intervention.
Conclusions
Findings from this study must be interpreted with caution given the small sample size, but they do not support the widespread adoption of MTH to achieve clinically significant changes in HbA1c. MTH may, however, have positive effects on blood pressure and protective effects on some aspects of mental health.
Keywords
Introduction
Telehealth (TH) encompasses a range of electronic applications used to exchange medical information from one site to another to improve health care delivery and patients’ clinical status.1,2 The subset of telehealth applications focused on in this paper is the recording of clinical and self-management data and their transmission to health care providers for review and feedback (also referred to as telemonitoring). These make possible the tracking of self-monitoring data and receipt of personalised feedback, potentially facilitating pattern analysis, reinforcing health behaviours, and promoting goal-setting, action planning or problem-solving.3–8 Many of these TH applications are now available for use on patients’ mobile-phones. 9 The added value of mobile TH (MTH) is that the recording, transmission and receipt of feedback can happen in any place, at any time and from a personal device already integrated into peoples’ lives. Although not all mobile applications include features recommended in clinical guidelines 9 or have been approved by a regulatory authority, 10 they have the potential to support timely medical management (e.g. medication dosage review) as well as self-management tasks related to lifestyle (e.g. physical activity, diet), medication taking (e.g. reminders), and self-monitoring (blood glucose (BG), blood pressure (BP)). 11
Recent reviews12,13 have found an evidence-base to support the use of TH (mobile and non-mobile) to improve glycaemic control (HbA1c). Pooled reductions in HbA1c following TH are sometimes, but not always, statistically significant and range between 0.03% and 0.51%.14–22 The majority of reductions are small in magnitude (<0.4%); their clinical significance remains debatable.
A limitation of TH studies underlined in several reviews18,23 is that little attention has been given to other outcomes than HbA1c. HbA1c is the gold standard for monitoring long-term glycaemic control 24 and is used to adjust therapy, assess quality of care, and predict the development of complications, 25 but other outcomes such as BP, body mass index (BMI), medication changes, and patient-reported outcomes are important. In one systematic review of information technology (IT)-based self-management interventions, 26 only five (31.3%) of 16 studies reported on health-related quality of life, BP, or BMI, and only six (37.5%) of 16 studies reported on depression, whilst none reported on anxiety. Some large-cluster randomised, controlled trials (RCTs) have presented findings on quality of life and psychological well-being (i.e. depression or anxiety),27–29 but they remain a minority. TH could have a positive or negative effect on health-related quality of life, health care utilisation, and psychological well-being. 27 The potential effects of TH on medication dosage are also unclear. TH-associated improvements in HbA1c could result in decreased dosages; in contrast, timely medication adjustments and closer supervision could result in increased dosages for tighter BG control.
This study addresses some of the above limitations. It aims to examine the effects of MTH on a range of clinical (HbA1c, BP, daily insulin dose, diabetes outpatient appointments (DOAs)) and patient-reported outcomes (health-related quality of life and psychological well-being). In line with the model of behaviour change used to guide the evaluation, 30 we hypothesised that compared to standard care, the MTH intervention would significantly improve HbA1c, BP, quality of life, and psychological well-being. We did not have a priori hypotheses on the effects of MTH on insulin dosage and DOAs, as increases and decreases in these outcomes could both be appropriate for better health outcomes.
Research design and methods
Eligibility and study design
An RCT design was used to compare standard care supplemented with MTH to standard care alone. The study took place in a diabetes clinic in East London, United Kingdom (UK). Inclusion criteria included age 18 or above, poorly controlled type 1 or type 2 diabetes (HbA1c ≥ 7.5%)31–33 with the latest HbA1c collected within the last 12 months, taking insulin, and fluency and literacy in English. Exclusion criteria were previous experience using MTH, regular extended travels (≥3 weeks) outside the UK, home visits by a district nurse for BG monitoring and/or insulin administration, a diagnosis of kidney failure or sickle cell disease, pregnancy, and dexterity/visual problems compromising the use of a mobile-phone. We planned to recruit 248 participants to the study following a sample size calculation. 30
The MTH intervention
Participants allocated to the intervention group were provided with the MTH equipment (BG meter, BP monitor, mobile-phone, and Bluetooth cradle) and training. The mobile-phone software allowed participants to store and transmit diabetes-related data (BG and BP readings, time since last meal, level of physical activity performed that day, insulin dose, and weight) to an MTH nurse (see data recording and transfer steps in Supplementary File 1). Participants were recommended to continue to follow their regular BG and BP self-monitoring routine (a minimum of one clinical reading per month was recommended for those not prescribed self-monitoring BP). Colour-coded graphical feedback on the data recorded could be accessed through the mobile-phone menu, and was automatically displayed following each data transfer. The MTH nurses accessed the data transmitted to the server via a Web portal also accessible to MTH patients. The MTH monitoring service and equipment were provided by a private company. In addition to providing feedback on out-of-range clinical readings (as needed) and education on lifestyle changes (six weekly educational calls), the MTH nurses supported insulin titration; if a more substantial medication review was required, participants were recommended to make an appointment with their diabetes specialist nurse (DSN). This minimised the possibility for patient emergencies to occur as a result of MTH care. A detailed intervention protocol has been published. 30
Standard care
Standard care at the diabetes clinic consisted of follow-up appointments with a DSN every three to four months, and one annual or two semi-annual appointments with diabetes consultants, depending on glycaemic control. A DSN was available during working hours to respond to urgent patient queries.
Measures
The majority of outcomes presented in this paper were assessed at baseline, three months, and nine months (unless indicated otherwise below). The primary outcome of the study was HbA1c. This was measured and analysed blind to group allocation using high-performance liquid chromatography (reference range of 4%–6%). Participants without an HbA1c test result within two months of the desired measurements were invited to have an HbA1c test performed and were aware this was for study purposes.
Secondary clinical outcomes included BP and daily insulin dose (both at baseline and at nine months), and number of DOAs attended with a DSN or consultant (over nine months). Patient-reported outcomes were measured with commonly used, standardised, and psychometrically sound tools. These included assessments of health-related quality of life using both a generic measure (Short Form Health Survey (SF12v2), which includes a Mental and a Physical Component Scale, abbreviated to MCS and PCS, respectively) and a diabetes-specific measure (Diabetes Health Profile, DHP-18; three subscales: Barriers to Activity, Disinhibited Eating, Psychological Distress). Symptoms of depression (Centre for Epidemiologic Studies Short Depression scale, CESD-10) and anxiety (Short Trait Anxiety Inventory, STAI-6) were also assessed.
Trial procedures
Ethics
This study was approved by the Joint University College London/University College London Hospitals (UCL/UCLH) Committees on the Ethics of Human Research, Committee Alpha (09/H0715/69). The RCT was registered with ClinicalTrials.gov (NCT00922376).
Consent
Participants with an appointment in the following two weeks were screened for eligibility and sent recruitment materials. Those who failed to respond or did not respond negatively were approached by a researcher blind to group allocation after their appointment. Participants willing to enrol in the study signed a consent form, and were given a baseline questionnaire to complete alone, or with the researcher.
Randomisation
Randomisation was carried out by a member of the research team upon receipt of the completed baseline questionnaire, and independently of DSNs, using an online sequence generator that generated randomised block allocations (blocks of 20).
Follow-up assessments
Three- and nine-month follow-up questionnaires were sent by mail to participants, and clinical data were collected from the medical records.
Training
MTH nurses received training to 1) use the equipment (demonstrations and hands-on experience), 2) deliver the intervention (i.e. familiarisation with intervention protocol requirements), and 3) remotely connect to and navigate patients’ electronic diabetes medical records. An engineer visited intervention participants within two weeks of randomisation to deliver the MTH devices and training (see details in Supplementary File 1).
Statistical analysis
Baseline differences between groups were examined using independent Student t tests and Chi-Square tests. Hierarchical linear models (HLMs) were used to compare mean changes in primary and secondary outcomes between MTH participants and controls. Random effects accounted for within-participant correlation, and were fitted using a first-order autoregressive covariance structure which assumes a steady decrease in correlations between measurements with time. Baseline differences were adjusted for and entered as covariates (fixed effect). A significant treatment Group by Time interaction was interpreted as evidence for differential treatment effectiveness. For all outcomes, we calculated Hedges g standardised effect sizes for mean group differences at follow-up, and 95% confidence intervals (CIs). A Mann-Whitney test was used for between-group comparisons on the number of attended DOAs.
All analyses were conducted on an intention-to-treat (ITT) principle. For the primary outcome, HbA1c, a sensitivity analysis was performed that included only MTH participants with monthly data transfers to verify the robustness of the findings. Monthly transmissions were not a minimum protocol requirement, but were considered to be an indicator of regular engagement with, and receipt of, the MTH intervention. For all analyses the level of significance was set at p < 0.05.
There were less than 5% of missing data. Data were missing completely at random (Little's test), suggesting the imputation method used was unlikely to influence results. 34 Stochastic regression imputation was used (using Markov Chain Monte Carlo methods) to impute data at the scale level. Missing primary outcome data or unreturned questionnaire data were not imputed.
Results
Several recruitment challenges (high non-attendance rates, exclusions due to poor English, gatekeeping by health care professionals, changes to discharge policy) were experienced and are reported in another paper.
35
In total, 205 (70.5%) of 291 people invited to take part in the study and confirmed to be eligible refused to participate. Eighty-one (94.2%) of 86 enrolled participants returned their baseline questionnaire and were randomised to the intervention (n = 45) and control (n = 36) groups. Figure 1 is a Consolidated Standards of Reporting Trials (CONSORT) diagram of the study flow.
CONSORT flowchart.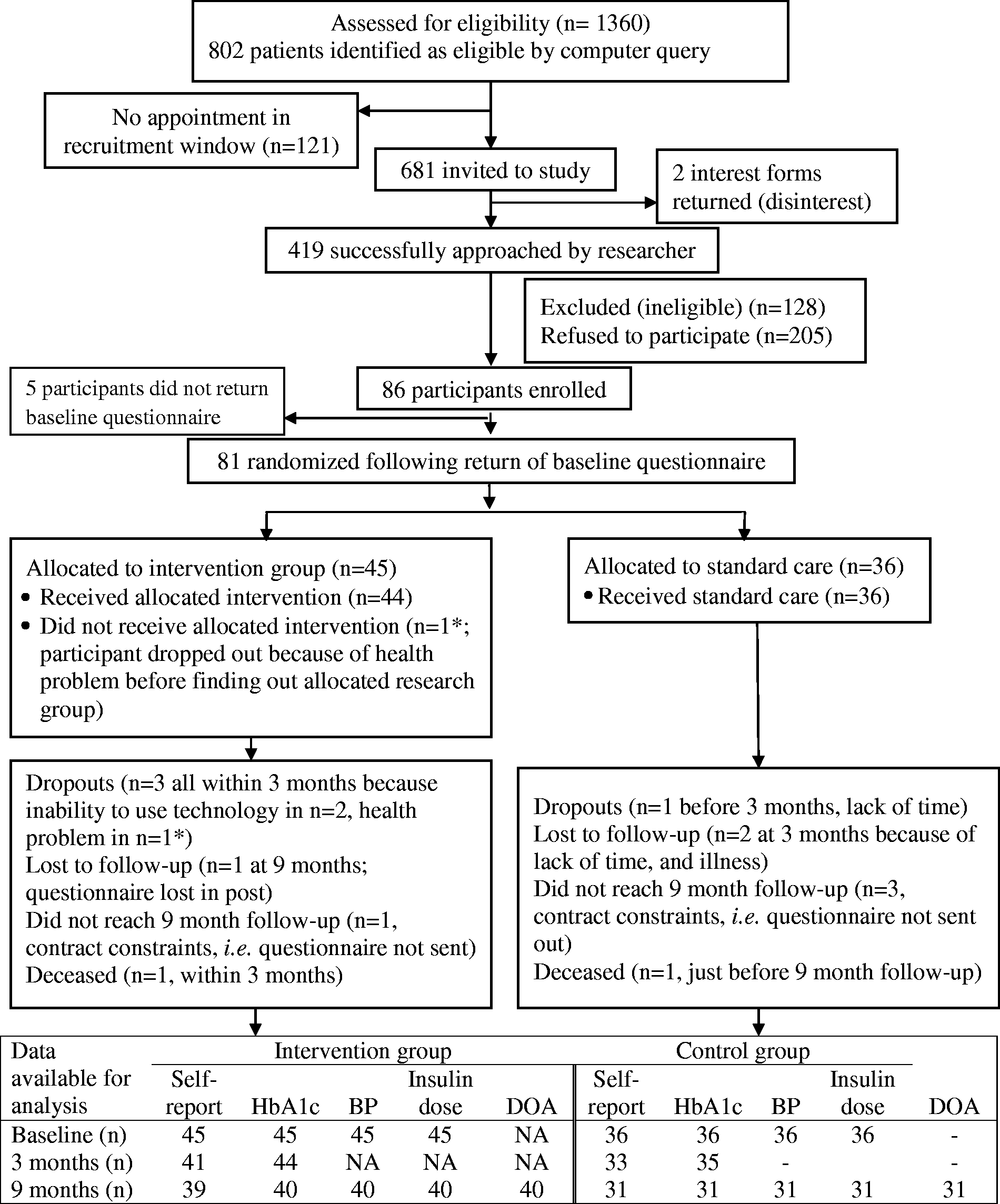
Demographic and clinical characteristics of study participants at baseline.
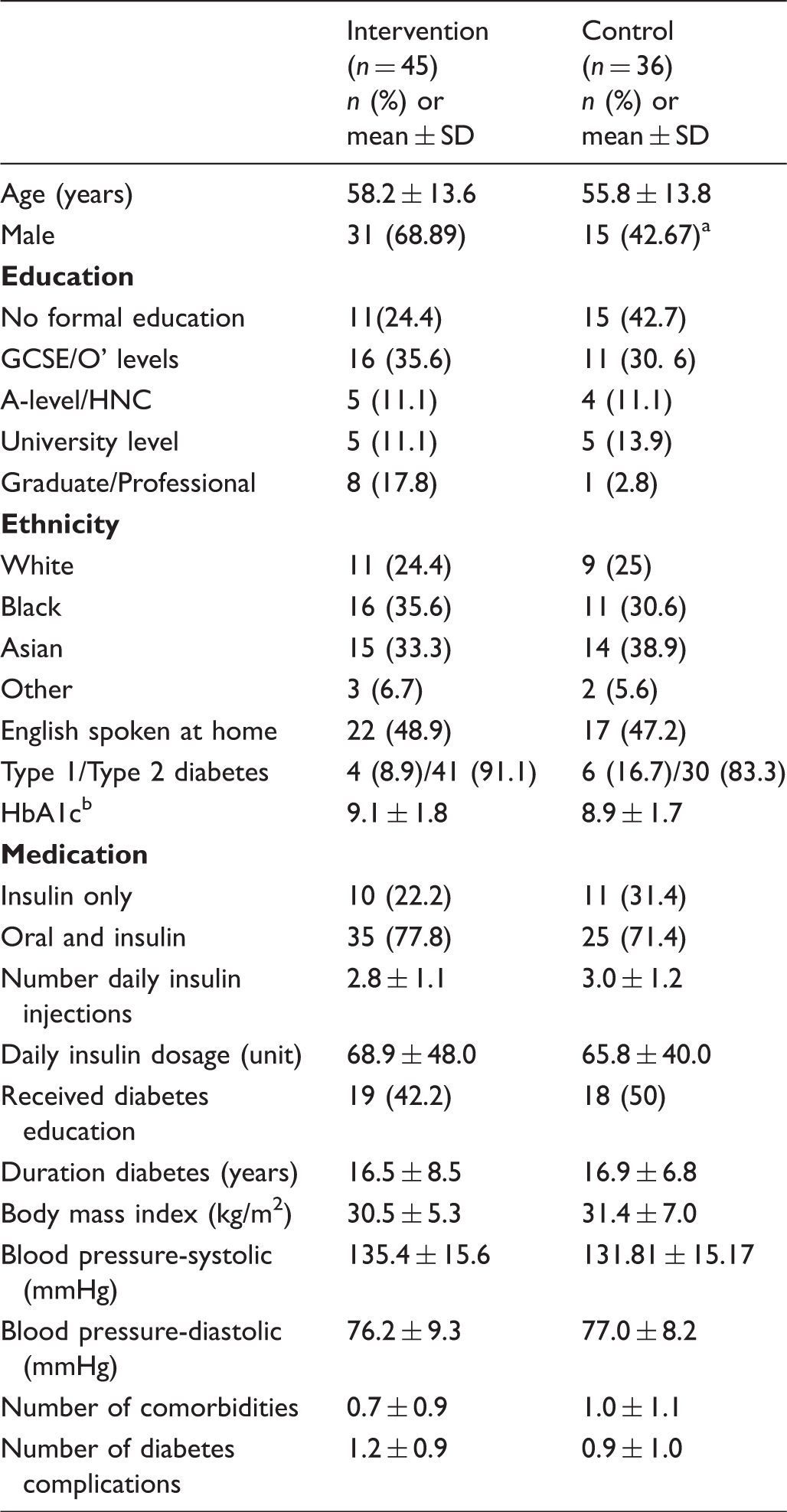
There was a significant difference in gender distribution between groups (t = 6.13, p = 0.013).
One eligibility criterion in our protocol was for the most recently measured HbA1c in the last 12 months to be ≥7.5% at the time of recruitment. There were 16 (19.8%) participants (five of whom were in the mobile telehealth (MTH) group) who had an HbA1c below 7.5% by the time baseline HbA1c was collected. To maximise sample size, these participants were not excluded from the analyses. Regarding blood pressure, 34 (41.9%) of the sample at baseline had a blood pressure greater than the threshold above which initiation or intensification of hypertensive is required (140/80 mmHg).
GCSE: General Certificate of Secondary Education; HNC: higher national certificate.
ITT analyses
Changes in primary and secondary outcomes.
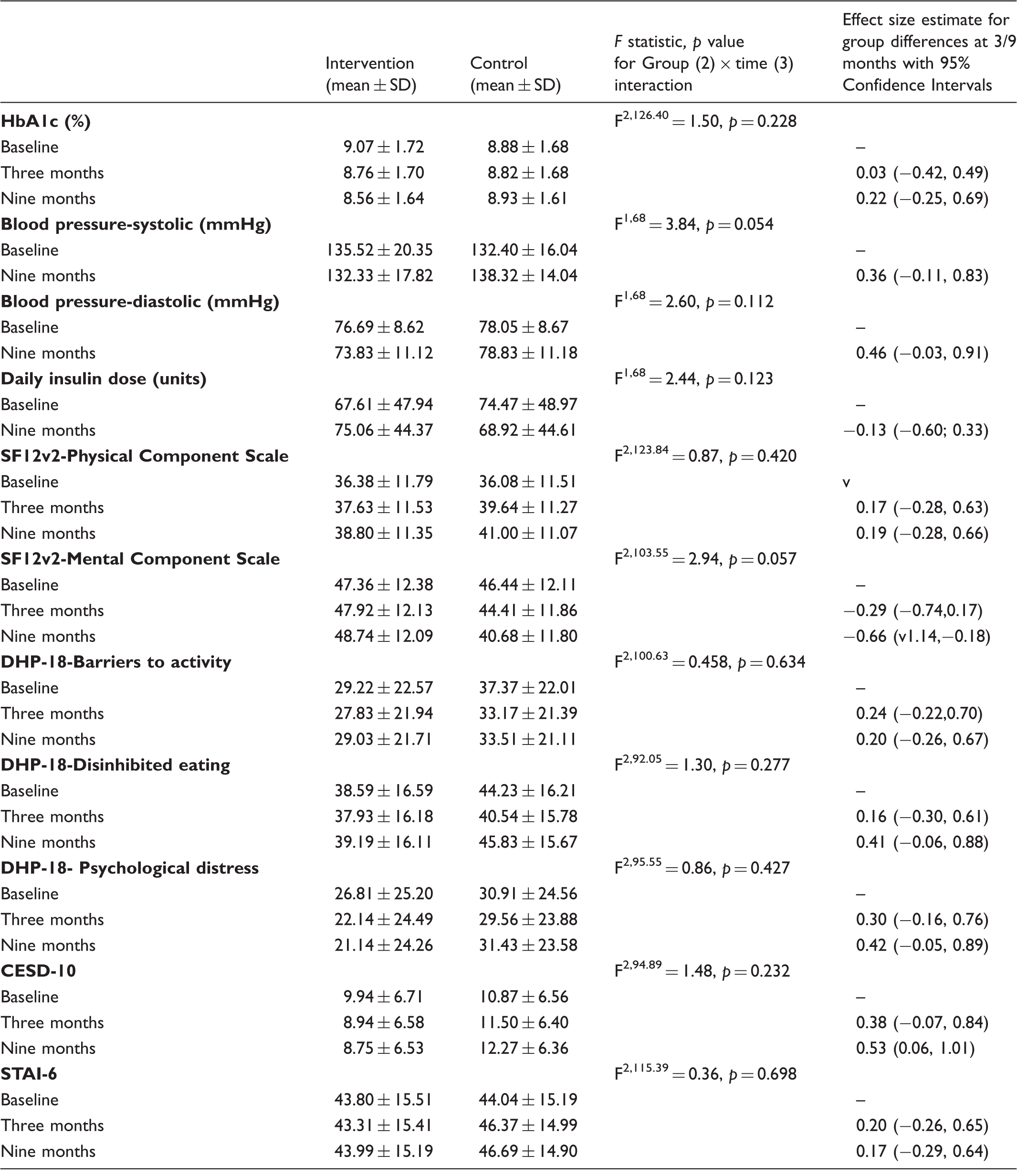
DHP-18: Diabetes Health Profile; SF12v2: Short Form Health Survey; CESD-10: Depression scale; STAI-6: Anxiety Scale. The DHP-18 includes three subscales on barriers to activity, disinhibited eating, and psychological distress. For the SF12v2 and DHP-18, scores are transformed to a 0–100 scale as per scoring instructions. For SF12v2, higher scores represent better quality of life; For the DHP-18, CESD-10 and STAI-6, higher scores represent worse quality of life, and more severe symptoms of depression and anxiety. Consistent with other research in this area, 36 the trial start date was taken as the date on which mobile telehealth (MTH) equipment and training was provided to intervention participants. For controls, the trial start date was the return date of the completed baseline questionnaire.
None of the Group by Time interaction effects for secondary outcomes were significant, although the borderline p values for BP (systolic, p = 0.054) and for mental health-related quality of life (SF12v2-MCS, p = 0.057) could indicate a trend in favour of MTH. The mean reduction in systolic BP from baseline to nine months in interventions was 3.2 units compared to a 5.9-unit increase for controls. SF12v2-MCS scores remained relatively stable in MTH participants during the nine-month intervention period (from 47.36 ± 12.38 to 48.74 ± 12.09), compared to a worsening in controls (from 46.44 ± 12.11 to 40.68 ± 11.80). The effect size for group differences at nine months was particularly large for this outcome (Hedges g = −0.66) and CIs did not cross zero, lending further support to an MTH effect on mental-health related quality of life. Similarly, scores on the depression scale (CESD-10) improved over nine months for MTH participants (from 9.94 ± 6.71 to 8.75 ± 6.53) compared to a worsening for controls (from 10.87 ± 6.56 to 12.27 ± 6.36). Although the p value for the Group by Time interaction was not significant, the effect size for mean group differences at nine months was large (Hedges g = 0.53) with CIs that did not cross zero, which could indicate a potential effect of the MTH intervention.
The Group by Time interaction was not significant for daily insulin dose. There were no significant differences in the median number of DOAs attended during the study with DSNs by MTH participants (median = 1) and controls (median = 2) (U = 581.50, z = −0.47, p = 0.637), or in the median number of DOAs attended with diabetes consultants by MTH participants (median = 1) and controls (median = 1) (U = 626.00, z = 0.073, p = 0.942).
Sensitivity analysis
A sensitivity analysis carried out for the primary outcome, HbA1c, included 22 MTH participants with at least one monthly data transfer. 30 Mean HbA1c (%) at baseline, three months, and nine months for the 22 MTH participants were 8.90 ± 1.43, 8.79 ± 1.43, 8.35 ± 1.43, respectively. Results confirmed the ITT findings (F2, 80.72 = 1.88, p = 0.160 for the Group by Time interaction; Hedges g values were 0.00 (95% CI −0.53, 0.53) at three months and 0.38 (95% CI −0.16, 0.92) at nine months.
Discussion
This study investigated the effects of MTH on clinical and patient-reported outcomes. Recruitment challenges are detailed in another paper with data on reasons for refusal, exclusions, and the contextual factors that hampered recruitment, 35 and the sample size underlines the need to interpret findings cautiously. Failure to reach the targeted sample size is not uncommon and happened in 45% of Health Technology Assessment and UK Medical Research Council-funded RCTs. 36 The majority (55%) of sample sizes in diabetes MTH studies are smaller 38 than 80, making this study one of the larger evaluations.
Supplementing standard care with MTH did not result in statistically significant improvements in HbA1c. This lack of effect was supported in ITT and sensitivity analyses. The trends in HbA1c were, however, in the expected direction and a larger sample size may have yielded significant results. Several reviews15,19,39 have underlined the limited evidence-base to support the widespread adoption of TH to achieve clinical improvements in glycaemic control, yet other work has suggested the opposite.29,36,40
Several factors can help explain the above inconsistencies. First, the ability for the MTH nurse to make changes to medication dosages may vary across studies. In the current study, although the MTH nurse recommended appropriate insulin adjustments to MTH participants, they were asked to schedule an appointment with their DSN if more substantial dosage changes were required, which could also explain the non-significant effect of MTH on insulin dose. A similar study 41 proposed that this model of care may have limited the effect of MTH on HbA1c. This is also supported in a review 18 in which TH interventions supporting changes in patients’ prescriptions had a greater impact on HbA1c. Second, inconsistencies in findings across TH studies may be related to intervention content. A greater number of self-monitoring of BG (SMBG) elements (e.g. patient education, provider education, structured SMBG profile, SMBG goals, feedback, data used to modify treatment, interactive communication or shared decision making) has been associated with greater effectiveness in reducing HbA1c. 42 Future syntheses of the literature may benefit from considering these differences in intervention content. The application of behaviour change taxonomies to this area of research may help determine the most effective active ingredients in MTH studies. 43 Third, HbA1c is a measure of long-term glycaemic control as it reflects BG levels over the past 8–12 weeks. 25 The use of other indicators to measure BG control over shorter time periods (e.g. glycaemic variability, time in range) have been recommended 44 and may yield more consistent findings on the effects of MTH on diabetes control, particularly for studies with shorter intervention periods. Finally, differences in intervention fidelity may help explain inconsistencies in findings. Intervention fidelity data are rarely reported, yet those from the current study 35 revealed that the MTH intervention was delivered at a lower dose than intended, and this may have limited the effects of the MTH intervention.
Only approximately half of ‘telediabetes’ studies measure BP as an outcome 45 and intervention effects are inconsistent. A meta-analysis of TH studies 18 found no significant effect on BP. In this study, poorly controlled hypertension was not an inclusion criterion, and 41.9% had baseline BP readings above the threshold to initiate or intensify hypertensive medication (i.e.140/80 mmHg). This may have limited the magnitude of BP changes and may explain the borderline significance of the findings. These trends in the data are noteworthy, however, given they occurred in a study with little emphasis on BP. The protocol 30 required that lifestyle advice be provided only once to a patient above the recommended threshold, after which a visit to the doctor to adjust hypertensive medication was encouraged. In addition, MTH usage data showed that BP readings were infrequently transmitted, 30 minimising clinical intervention opportunities. Personalised feedback is believed to make self-monitoring of clinical readings more actionable. 4 This is the mechanism that may have resulted in the encouraging trends observed in BP.
Effects sizes for mean group differences at nine months on the mental health dimension of the SF12v2 (0.66, CI 95% –1.14 to 0.18) and CESD-10 Depression Scale (0.53, CI 95% 0.06–1.01) were large and in favour of MTH, with CIs not crossing zero. Scores on these measures deteriorated over time for controls whilst remaining more stable in MTH participants. Although the study was not primarily designed to examine these effects, the patterns observed could be indicative of a protective effect of MTH on mental health, possibly through the social support received through MTH contacts. Evaluations of TH interventions that do not focus on social support often do not measure it, but qualitative interviews following teleconsultations have suggested TH may increase perceived social support. 46 This may be an added advantage of TH that future studies would benefit from examining.
There have been some concerns about the potentially detrimental effects of TH. TH may increase the burden of illness work or isolate patients, by decreasing face-to-face contacts with health care providers, or may undermine an individual’s choice and independence.47,48 In light of these concerns, the lack of effects of the tested intervention on the physical dimension of health-related quality of life (SF12v2-PCS) and on diabetes-specific quality of life (DHP-18), or on measures of depression and anxiety, can be considered reassuring. The omission of psychological variables from TH evaluations has been critiqued23,27 and our data add to this small body of evidence in this area. Overall these findings are in line with other work reporting on quality of life or psychological well-being.20,27,29,49 A review of psychological, self-management and educational interventions in diabetes 50 underlined the need for interventions to clearly address negative mood for improvements in psychological well-being, which was not the case in this study.
Similar to another study, 28 MTH was not found to influence the number of DOAs attended at the clinic. Studies on TH for diabetes have often focused on measures of hospitalisation or inpatient stays.51–53 Fewer studies have measured outpatient visits. In those that have, TH has generally been associated with increases in outpatient visits.52,53 As in our study, these studies required patients to visit their regular diabetes provider for medication reviews. They recruited participants at risk of or frequently using inpatient and emergency services, however, and facilitated appointment scheduling for intervention participants, both of which may have influenced the findings. In contrast, another study 51 in which TH care coordinators facilitated scheduling of outpatient visits found that their number was significantly reduced in intervention participants compared to controls. These conflicting findings suggest that in some studies, TH may result in appointments that prevent further health deterioration, whilst in other studies TH may prevent health problems from occurring altogether. A range of factors including patient and disease characteristics, service use before TH, the TH monitoring protocol and model of care, as well as the compensation model for health providers, are likely to influence findings on outpatient appointments.
This study is not without limitations. It is a comprehensive evaluation that relies on a range of psychometrically valid tools. Failure to reach the targeted sample size is the most notable drawback, particularly given the number of outcomes measured. As mentioned above, however, this is not uncommon in this area of research and it is important for clinical evaluations to include patient-reported outcomes too. As a result, these findings need to be interpreted with caution. The low response rate limits the generalisability of the findings, 54 although importantly refusal reasons do not differ from other studies, including those with a higher participation rate. 35 It may be more appropriate to consider the analyses conducted as exploratory. Also, the focus on DOAs with DSNs and consultants working at the clinic was based on the data available. MTH participants may have visited their general practitioner to discuss their diabetes. This is unlikely, however, as patients are referred to their DSN by their general practitioner for diabetes-related care. Finally, this study did not examine the relationship between MTH usage data and treatment effectiveness. Results of the sensitivity analysis suggest that there is little relationship between variations in MTH usage and HbA1c, but research studies with larger sample sizes allowing for multiple testing may benefit from considering the moderating effect of MTH usage on outcomes.
Footnotes
Acknowledgements
The views expressed are not necessarily those of the Department of Health for England. The authors would like to thank participants who agreed to take part in this study, as well as the health care professionals at the diabetes clinic who offered their help during this study.
All authors were equally involved in the design of the study. JB was responsible for study implementation and data collection under the supervision of SN and SH. JB is the primary author of this paper, and revisions were made by SN and SH. JB, SH and SN approved the final version of the paper and take responsibility for the content of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Policy Research Programme of the Department of Health for England.