
Abstract
Introduction
In this paper, we evaluated patients’ perspectives on the use of a system for home tele-rehabilitation, designed for subjects with low computer literacy suffering hand impairment due to rheumatic diseases.
Methods
After a clinical trial assessing device effectiveness, the Psychosocial Impact of Assistive Devices Scale (PIADS), Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) and Individually Prioritised Problem Assessment (IPPA) questionnaires were administered to evaluate the system’s impact on each patient’s life, and the results were correlated with clinical indices. Patients were asked to continue self-administered rehabilitation with common objects. One year later, a semi-structured telephone interview gathered data on their experience.
Results
The system received a positive QUEST score (4.5 ± 0.3) and a modest PIADS score (0.84 ± 0.8) due to the small impact on adaptability and self-esteem. The IPPA (3.7 ± 3.4) revealed improvement in the ability to perform tasks considered important, which was significantly correlated (r = 0.60; p < 0.02) with the clinical Health Assessment Questionnaire (HAQ) index improvement. The interviews revealed a positive engagement effect, enhanced by the need to develop skills to be able to use the device (technological challenge) and by the perception of more attention by the medical staff. This may explain the significant dropout rate (80%) from the post-trial rehabilitation of the patients who used the device.
Discussion
The system was largely accepted by the patients. The results suggest that the need for information on their rehabilitation progress and the technological challenge deserves further study to make patients more autonomous in cases of continuous rehabilitation.
Introduction
Rheumatoid arthritis (RA) and systemic sclerosis (SS) are rheumatic diseases likely to create severe hand functional deficits, compromising patients’ quality of life. Pharmacological treatments are currently associated with rehabilitation, followed by adapted physical therapy, 1 leading to a gradual recovery and a sustained maintenance of movement ability. Recovery is a slow process, and home rehabilitation is a necessary measure for containing costs, provided that good compliance is guaranteed. Tele-rehabilitation platforms, like those presented by Pani et al. 2 or Giansanti et al., 3 aim to solve this problem by providing remote supervision of self-managed home rehabilitation sessions.
Most existing studies reporting on platforms for quantitative monitoring of rehabilitation, even those that are not properly tele-rehabilitation, provide an effectiveness evaluation. Little effort is usually spent on analysing the patients’ experience with such devices, their perceived satisfaction of care and the impact of these technologies on their lives after the end of the trial. This is a critical aspect that should be evaluated, especially when the platforms are designed to be used by people with low computer literacy, as is usual for elderly people who are at higher risk for rheumatic diseases. In fact, several platforms make use of complex technologies, such as virtual reality (VR) systems, to achieve a greater patient involvement through motion-based, amusing games,4,5 whereas some others require the support of a PC or a game console, along with an external connection to exploit the tele-monitoring features over the Internet. 6 Some others are simply not suited for people with hand deformities 7 or who have difficulties in setting up the system for a rehabilitation session. 8 In this work, we focused on the patient’s evaluation of a tele-rehabilitation system, presented in Pani et al., 2 by means of validated questionnaires and field research consisting of a semi-structured interviews performed one year after the end of the trial. We tried to match these results with the clinical trial outcomes and pinpoint some key attention points requiring advanced investigation.
Methods
The tele-rehabilitation system presented in Pani et al.
2
has been expressly designed to support self-managed home rehabilitation sessions for patients with hand functional impairments caused by rheumatic diseases. The system is based on a patented device
9
(see Figure 1). It includes a set of sensorized tools for the execution of up to seven strength and dexterity hand exercises. Considering that many rheumatic patients are in their old age, most of them with low computer literacy, the system has been conceived to be stand-alone, easy to use, self-contained and with embedded connectivity features (an integrated general packet radio service (GPRS) module), exploiting a store-and-forward paradigm.
A patient involved in the clinical trial during a training session in the outpatient clinic (the connection with the PC, through a Bluetooth link, is enabled only for outpatient clinic examinations, and disabled for rehabilitation at home).
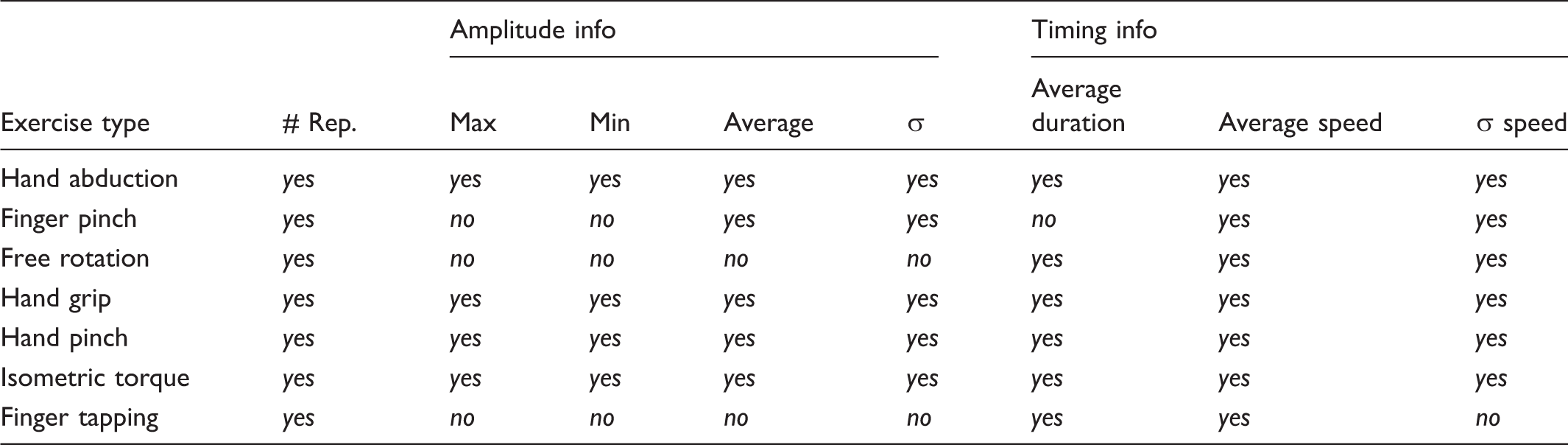
Main statistics collected during the rehabilitation session (σ is the sample standard deviation).
The clinical trial
Baseline distribution of demographic and clinical characteristics of rheumatoid arthritis (RA) and systemic sclerosis (SS) patients according to allocation in experimental and control arms.
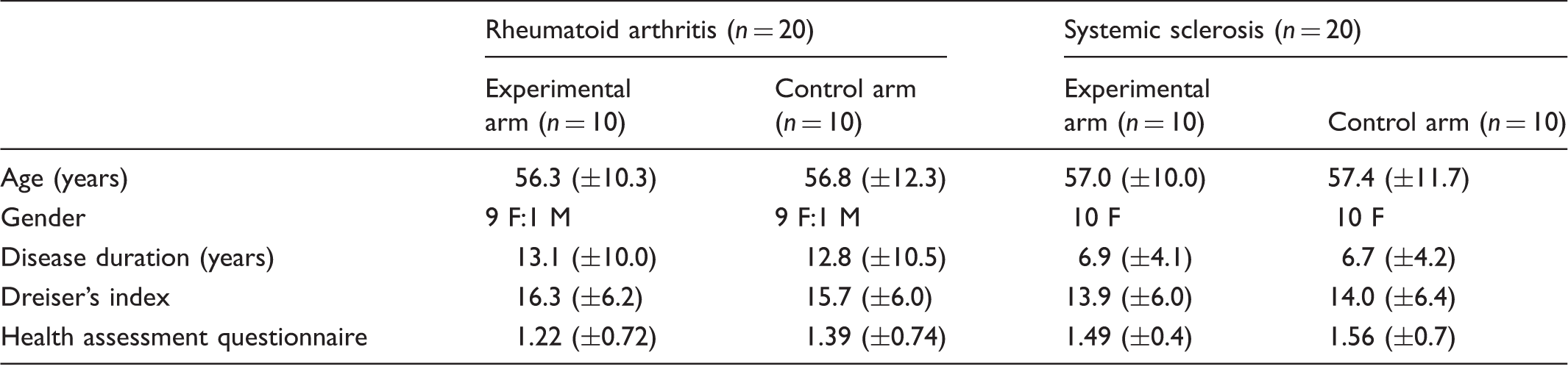
Numbers represent mean (± standard deviation).
Those in the EA, after a short training period in the outpatient clinic, underwent an autonomous rehabilitation therapy at home with the tele-rehabilitation device. The geographical distribution of the patients’ houses is depicted in Figure 2. Tele-monitoring data were checked twice per week, allowing investigators to contact patients by phone in case of loss of workout sessions or worsening trends in exercise statistics during the week, possibly providing feedback on how to modify the protocol (e.g. if patients reported pain, the physician advised them to reduce the intensity). The patients in the CA performed the same type of rehabilitation, exploiting common-use objects (bottles, coins, etc.), without any form of remote control. They used the tele-rehabilitation device in the outpatient clinic three times, for functional assessment at the beginning, halfway through and at the end of the trial, under the supervision of a trained kinesiotherapist.
Patients’ distribution across the regional territory. The position of the rheumatology unit in Cagliari is marked with a red diamond mark.
At the end of the trial the patients in the EA had to give back the device, and patients of both arms received a maintenance protocol based on the type of exercises (and tools) used by the patients from the CA. Patients were asked to continue with the protocol whenever they were free of joint inflammation.
Evaluation of patients’ perceptions and satisfaction
Both the patients’ perceptions of the rehabilitation device and its impact on their daily lives were investigated. Three validated questionnaires were administered to the people enrolled in the EA who completed the trial (18 out of 20 patients (two dropouts); age, 56.7 ± 10.3 years; 17 female and one male). The CA was excluded because the questionnaires were conceived for patients who regularly used the device. The chosen questionnaires were the Psychosocial Impact of Assistive Devices Scale (PIADS), 14 the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) 15 and Individually Prioritised Problem Assessment (IPPA). 16
One year after the end of the trial, both study arms (CA and EA) underwent a semi-structured interview to better investigate some existing aspects and discover new ones based on the participants’ experiences. The exclusion criteria were cognitive impairment, dropout from the trial and unavailability to carry out the interview. Overall, 31 patients out of 40, 15 belonging to the EA (56 ± 10, only one male) and 16 belonging to the CA (56 ± 13, no males), were included in the study.
Validated questionnaires
The PIADS 14 is a 26-item questionnaire, which we administered at the end of the trial, that measures the impact on quality of life of using assistive technologies. The items can be grouped into three subscales, pertaining to competence, adaptability and self-esteem. For each item, the respondents must provide a score ranging from –3 ‘negative impact’ to +3 ‘positive impact’; the final score is the mean.
The QUEST, 15 which we administered at the end of the trial, rates the patient’s satisfaction with two aspects of the product and associated services, contributing to a single global score. The 12 satisfaction items were scored from 1 to 5; the final score is the mean.
The IPPA 16 assesses the effectiveness of an assistive technology in relation to those activities that the patient considers relevant. At the beginning of the trial, patients were asked to define up to seven tasks they had difficulties with, scoring both their importance and their difficulty from 1 to 5, thus obtaining a global baseline score. At the end of the trial, patients were asked to score the same tasks again (only difficulty level), without viewing their given baseline scores. A difference between the baseline and the follow-up scores reveals a perceived improvement.
Semi-structured interview
We were interested in patients’ daily rehabilitation routine after a certain amount of time from the end of the trial, and their opinions about their past experience in the trial. Our intention was that this would provide indications about the patients’ satisfaction with care in terms of paradigm and instruments. To this aim, the semi-structured interview is a valid instrument because:
It is well suited to the exploration of attitudes, values, beliefs and motives.
17
It has the potential to overcome the poor response rates of a questionnaire survey.
18
The participant is a conduit from which information is retrieved.
19
A relatively homogenous group will have shared experiences about the topic.
20
The patients were contacted by phone by a bioengineer with a good knowledge of the system but not involved in its original design. Except for one question, concerning feedback received while performing the exercises, the questions were the same for both groups. Questions were about:
Health status, asking if they are still performing the rehabilitation protocol; Motivation, to determine the habits of the patient concerning rehabilitation and desired feedback both during the rehabilitation period and now; Preferences and expectations: what the patients would have done to improve the rehabilitation process, and what they expected when the trial started; Way of interacting with the device or daily objects (depending on the group).
Results
The clinical results of the trial are reported by Piga et al. 11 They showed statistically significant improvement in hand functional parameters, with a better result in the group using the device, probably due to ergonomics, engagement and remote supervision. The HAQ and Dreiser’s indexes were used as major outcomes for their disability and showed statistically significant improvements. The mean HAQ score was 1.28 at baseline, corresponding to moderate/severe disability, and showed a decrease of 0.39, which represents an improvement well above the minimum value (0.22), indicating the change was clinically important. 21 The Dreiser’s index mean value at the beginning of the trial was 14.7 points, whereas at the end a reduction of five points was obtained. All these results highlighted a progressive and statistically significant (p < 0.05 using repeated-measures and mixed-models ANOVAs) reduction of the subjective and objective disability, for both RA and SS patients.
Questionnaires and semi-structured interviews
The PIADS showed a mean score of 0.84 ± 0.8 points overall. The individual results in the three subscales (Figure 3) show that the patients considered the use of the device beneficial to their ability to perform common tasks (0.88 ± 0.8 in the competence subscale and 0.85 ± 0.9 in the adaptability subscale), whereas the aspects related to self-esteem were the least affected (0.76 ± 0.9).
PIADS scores for the three categories separately.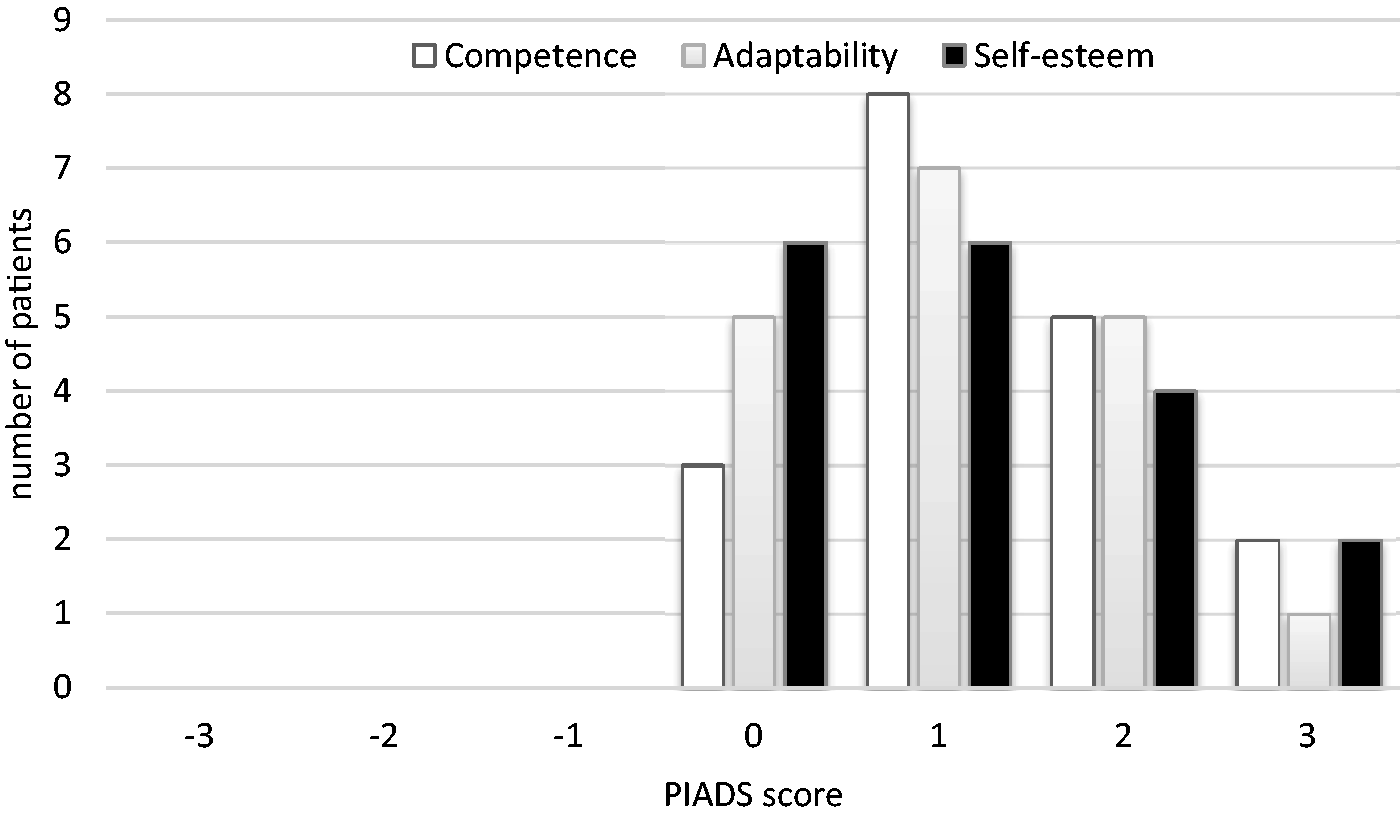
The QUEST result was 4.5 ± 0.3. As can be seen in Figure 4, from the analysis of the individual questions, both weight and size had the worst scores because the device weighed 6 kg (too much for some patients) and it was bulky (a bit large to be easily stored between consecutive sessions). Both these minor problems are related to the prototypical version of the device.
Average and standard deviation of the answers to the individual QUEST questions (error bars represent the standard deviation).
On the IPPA, a score of 3.7 ± 3.4 was achieved, with the individual results ranging from 0 to 11.6. Detailed results are shown in Figure 5. When the pre-test results (17.7 ± 3.9) were compared to post-test results (13.9 ± 4.8), by means of Student’s t test for paired samples, the pre-test/post-test effect was statistically significant (p < 0.001). This showed how almost all the patients improved their perceived ability to perform the tasks they identified as important at the beginning of the trial. We also evaluated the relationship between these results and the clinical questionnaires to investigate whether there was a correlation between the clinical improvements and the perceived benefit derived from the use of the device. Probably because of the small sample size, no statistically significant correlation emerged when analysing the RA and SS patients separately. By joining the groups, and considering only the HAQ because it is not disease-specific, a statistically significant correlation between HAQ improvement and IPPA was found (p = 0.02, using linear regression, r = 0.60). It is worth noting that IPPA is the only questionnaire that intrinsically measures a perceived improvement after rehabilitation. This result revealed how the rehabilitation intervention similarly influenced both the patient’s perception, measured by the HAQ, and the different aspects measured by the IPPA.
IPPA questionnaire score distribution.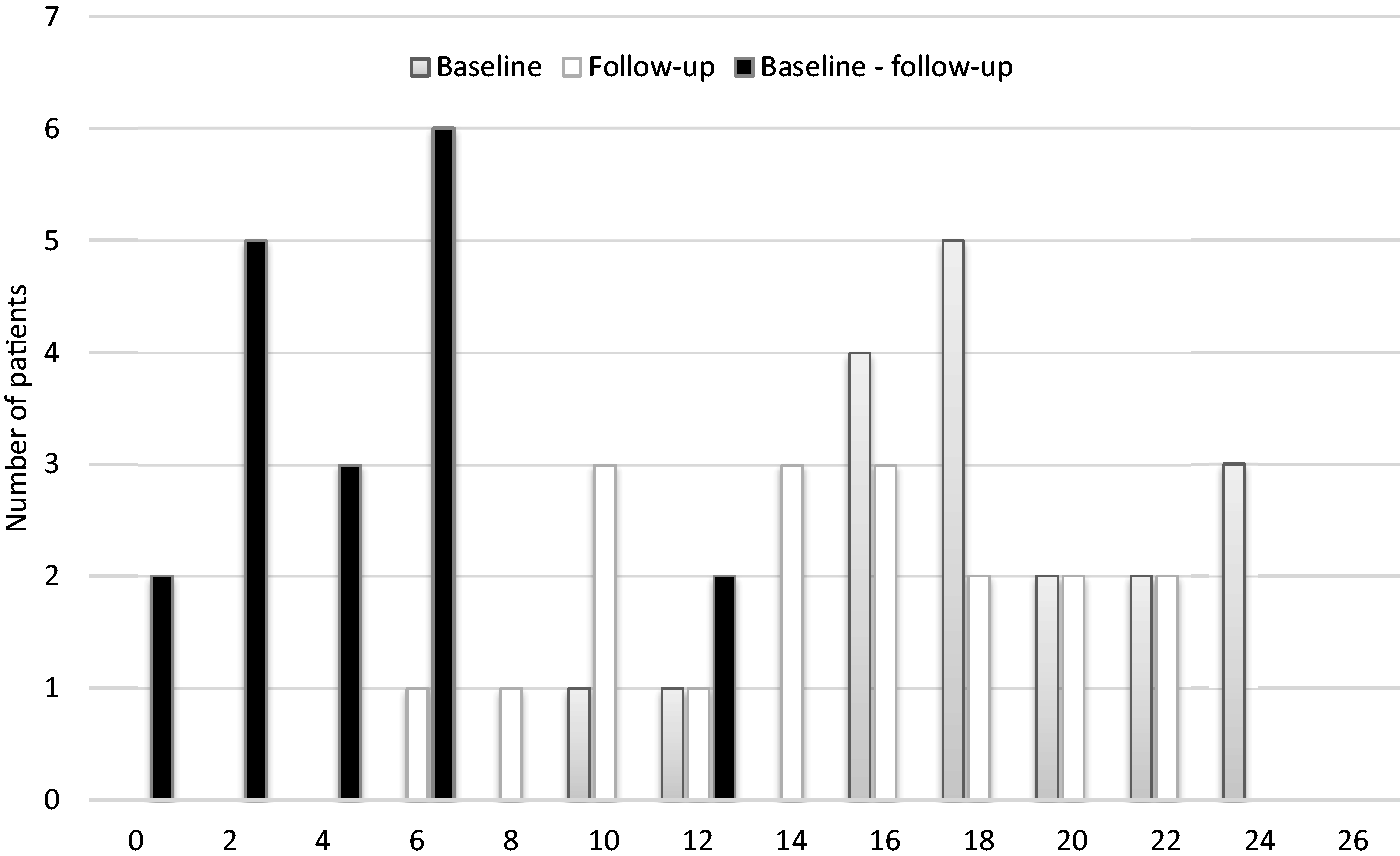
From the semi-structured interviews, we found other interesting results for the two arms of the trial (EA and CA). After the end of the trial, patients gave up the maintenance protocol more in the EA (80%) than in the CA (56%); 60% and 31%, respectively, gave up after a while, and 20% and 25% gave up immediately. Among those who did not, the percentage of patients exercising seldom (13% and 25%, respectively) was higher than that of patients performing the suggested exercises almost every day (7% and 19%, respectively), though it should be mentioned that everyday training was not required.
When asked about the perceived advantage of exercising with the device versus common objects, 80% of the EA patients considered the device better because of aspects such as motivation, engagement, routine and feedback, whereas 13% had no preference. In contrast, 44% of the CA patients thought the objects were better because of the perceived complexity of the device and the easier availability of the objects and 25% thought the device was better for various reasons (motivation, rehabilitation effectiveness, comfort and constraint). Regarding the possibility of having the device available at home, only two patients in the CA would have chosen this, and two were uncertain. In contrast, 53% of the EA patients would like to own the device, two were uncertain and 33% would not like to have the device because they had no time to follow a rehabilitation programme.
Compared with the maintenance programme, 87% of the EA asserted that using the device made them more motivated because they knew the medical staff were monitoring them. The same opinion was shared by 31% of the CA, revealing they preferred using the device for this reason. However, 62% of the CA did not think this fact motivated them to prefer the device to the common objects.
Interestingly, all the EA patients thought the device was simple to use (40% reported some difficulties limited to the first days) but also 50% of those in the CA thought the device was as easy to use as the objects. Some 13% of the patients in the CA thought the device was even easier because ‘it reminds you what to do with no need to read the instructions every time’. It should be noted that CA patients used the device only three times in the outpatient clinic for the functional assessment.
The great majority of patients were satisfied with the way they were followed by the medical staff (87% in the EA and 69% in the CA). A few of those in the CA would have preferred to go more often to the clinical centre. Almost all the patients in the two groups would have appreciated more feedback about their progress in the rehabilitation, either through direct access to the information or through communication with the medical staff. The EA were equally split between the two choices, whereas in the CA 25% were neutral and 50% preferred feedback from the clinicians, which was perceived as more safe (patients in the CA were worried about their ability to understand the progress of their rehabilitation from looking at an automatic feedback output).
Discussion
Beyond its validity as a rehabilitation instrument, discussed in previous works,2,11 the obtained results are interesting from different points of view. The analysis of the questionnaire scores, compared to the clinical indexes, revealed how the clinical functional improvements did not affect either the evaluation of the device and service provided (QUEST) or the psychological aspects related to ordinary life experience (PIADS), despite the evident positive influence on daily activities (IPPA).
The semi-structured interviews enabled a deeper analysis. Though patients in the EA largely thought the device was better than the objects for exercising, the patients in the CA thought the opposite, and the motivations had a different depth. CA patients had this preference because they thought daily objects are common, easy to find and easy to use and move, whereas EA patients had their preference because the device entailed a daily scheduled meeting, an engagement, real-time feedback concerning the way they conducted exercises, and was motivating because doctors were always able to check their results. This dichotomy found confirmation in the compliance with the prescribed protocol (measured as the ratio between the performed rehabilitation sessions and the required ones), which was very high: 91.2 ± 7.6%. Furthermore, the patients clearly took advantage of the possibility to exercise whenever they wished during the day, rather than being limited to the strict schedule of a rehabilitation centre, as Figure 6 demonstrates.
Distribution of executed training sessions during the day.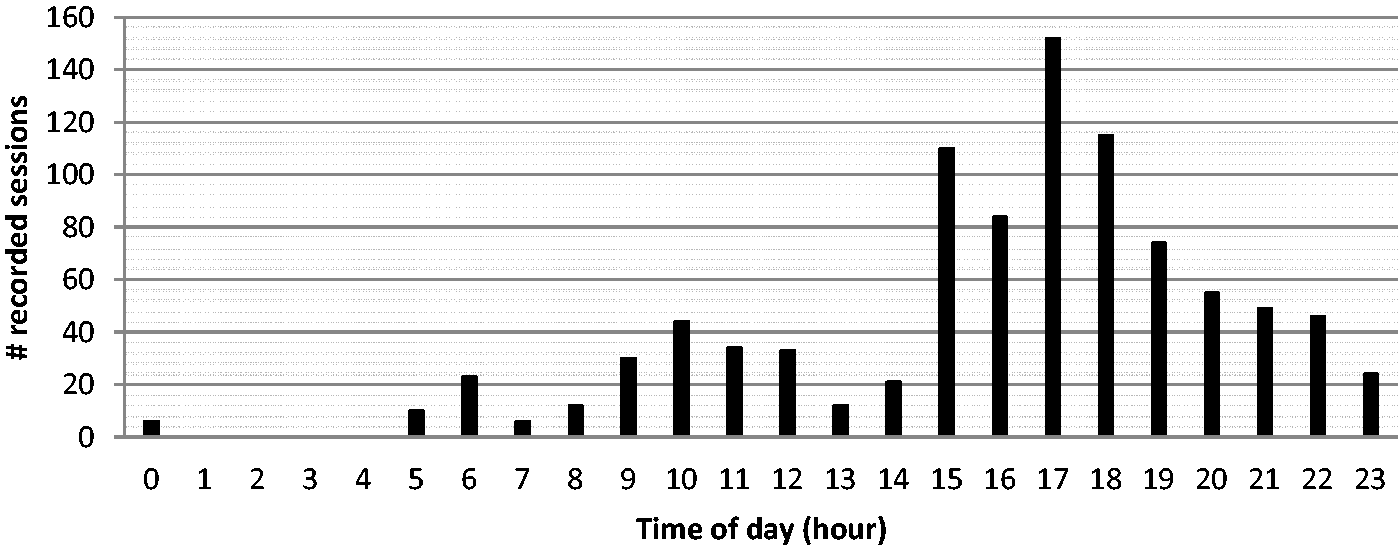
The patients in the EA perceived a greater engagement of the medical staff in their therapy. This is very important when separated by a long distance because patients do not feel left alone with their device but perceive the constant (remote) presence of the medical staff. This perception probably contributed to the greater number of dropouts (80%) in the post-trial rehabilitation protocol with common objects in the EA, regardless of the benefits achieved.
The reports of the EA suggest that they were more autonomous, curious to be informed about their improvements and more competent in executing the exercises. All these aspects were also reinforced by their sense of competence. In fact, at the starting point, the patients thought they might have been unable to use the device because of their limited skills. Their ability to develop this skill (in about one week, as evidenced from the interview, thanks to the simple user interface and the absence of any computer or external device) could have played the role of a challenge, 22 motivating them to carry on with a different level of involvement. They were able to understand the advantages of such a device (real-time feedback, constant monitoring), and they would never go back. The need for information and the technological challenge are aspects that need to be studied more deeply to make patients more autonomous, especially those with long rehabilitations. In such cases, a technological device such as that used in this study plays a fundamental role.
Beyond the patients’ perspective, the tele-rehabilitation system presents other concrete advantages. Considering that, with respect to the rheumatology unit in Cagliari, the most distant patient lived 250 km away (a distance that cannot be covered in less than approximately 2 hours and 45 minutes), the adoption of tele-rehabilitation can be considered well suited to the Sardinian geographical context and other rural areas, lessening the inequality of access to traditional care. From a cost perspective, the solution is also successful. A single rehabilitation session, similar to the one possible with this device, in a therapy centre costs approximately €13 (the cost is established by the Sardinian Regional Health Department). A protocol similar to the one followed in the trial, usually limited to 20 sessions per hand, would cost approximately €500 (plus travel costs). Patients are not likely to spend that much money every month. The running costs of the devices, i.e. device connectivity and 24/7 server costs, were approximately €15 per device per month (hence per patient), which yields a total of €45/patient for the duration of the whole trial (versus the €1500 for the conventional treatment for the same period). Even considering the device cost (but keeping in mind that devices can be re-assigned over time), which is approximately €700, and the cost of the medical personnel, which cannot be easily computed but is limited by the large number of patients who can be followed by a single therapist, the approach is quite promising in terms of sustainability. Remarkably, for the time being, the medical personnel would be insufficient to follow every patient with traditional approaches (considering that, in the region, the prevalence of rheumatoid arthritis is 550 per 10,000 inhabitants and that of systemic sclerosis is 3.5 per 10,000 inhabitants23,24).
As a report on patients’ perspectives, there are no major limitations in this study, but a minor limitation would be the small number of patients enrolled. Therefore, caution is advised in interpreting our results as they may be related to the size of the population under study. Second, a formal cost analysis was not performed, so the data reported should merely be considered an estimate.
In conclusion, our results suggest the possibility of using the same approach on different diseases or traumas whose treatment requires long-term rehabilitation.
Footnotes
Acknowledgements
The authors wish to thank Dr A. Dessì for her support with the validated questionnaires, Ms D. Porru for her help in carrying out the telephonic interviews, and all of the patients who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Region of Sardinia, Fundamental Research Programme, L.R. 7/2007 ‘Promotion of scientific research and technological innovation in Sardinia’ under grant agreement CRP2_584 Re.Mo.To. Project.