
Abstract
Introduction
Despite a growing literature base, substantial investment, and policy changes within governments, the integration of telehealth into routine clinical care has been limited. The availability of appropriate systematic education and training for practitioners has been highlighted as necessary for strong adoption. However, the availability and nature of telehealth-related education and training for practitioners is not understood. By reviewing the literature, we aimed to describe the delivery of education and training in telehealth, with particular focus on content, modes of delivery, types of institutions, and target clinician groups.
Methods
We performed searches using PubMed, Scopus, Embase, Web of Science, PsycINFO, the Cochrane Library, and ERIC. We included studies that were focused on the delivery of telehealth-related academic or vocational education and training. We extracted information pertaining to country, programs and their participants, and tabulated the results.
Results
Altogether 388 articles were identified, of which nine studies were selected for final review. Programs from five countries were represented and articles were spread across telemedicine and clinically oriented journals. Education and training in telehealth has been provided as both university level and vocational courses using conventional classroom based delivery methods and e-learning. Reported curriculum items included terminology, clinical applications, the evidence-base, and technological aspects.
Conclusions
Published evidence in peer-reviewed literature on telehealth education and training is limited. According to this review, a number of topics relating to telehealth have been covered by existing education programs both within tertiary and professional development levels.
Introduction
Despite a large literature base, and some formal evidence, to support the use of telehealth in a few well-established areas, such as radiology and dermatology, a substantial work is still needed for the field to mature. 1 Nonetheless, many governments and health systems have made attempts to introduce telehealth services, a few of which have become large and well-integrated, such as the Ontario Telemedicine Network in Canada 2 and Veteran’s Affairs Telehealth in the USA. 3 The interest in telehealth to improve health care services is global. A number of European countries have implemented various telehealth projects; and some countries have conducted large research studies to establish an evidence base.4,5 Global organizations such as the World Health Organization (WHO) have been promoting telehealth, particularly in low and middle income countries in Asia, Africa, and Latin America, as a new way to address critical health challenges.6–8
Some governments have made important policy changes to encourage and incentivize the use of telehealth. For example, the Australian federal government introduced reimbursement for certain video-based consultations involving general practitioners, specialists, Aboriginal health workers, nurse practitioners, and midwives. 9 In the USA, 46 states and Washington DC provide reimbursement for some video-based consultations under their Medicaid programs and this supports the healthcare costs of those on low incomes and those living with certain disabilities. 10
Alongside the increase in use of telehealth, a flourishing industry of medical, technology, and clinical service businesses has grown. The size of the market is difficult to estimate reliably. One group of analysts have suggested that it could be as large as USD$43.4 billion by 2019; 11 while those in another group were more conservative in their estimate of USD$36.3 billion by 2020. 12
Despite substantial investments and policy changes, the extent of adoption of telehealth is often less than expected; 13 a review of activity since the 2011 introduction of reimbursement for telehealth in Australia found that only 35,565 (0.24%) of total eligible consultations have been conducted using video-based telehealth. 14 While the barriers to adoption are wide-ranging, in this paper we focus specifically on skills development. Because using telehealth implies a change in practice, it should be supported by appropriate education for current and future practitioners. The literature suggests that education and training (E&T) in telehealth is needed and valued,15–18 although the area has not been formally reviewed. Therefore, the key objective of this study is to review the literature published in peer review literature relating to the provision of E&T in telehealth for current and future practitioners. Our main interest was to understand the types of education available, content of E&T, methods of delivery, types of target groups, and types of providers. The review also assessed the quality of studies included in the study.
Methods
Search strategy
Search strategy.

MeSH: medical subject heading.
Inclusion and exclusion criteria
We included articles that focused specifically on the delivery of telehealth-related academic education at undergraduate or postgraduate level together with vocational continuing professional development (CPD).
Articles describing patient education, the use of telehealth for education (rather than education about telehealth itself), or technical aspects were excluded. Papers relating to education in health or medical informatics were also excluded, unless they had a focus specifically on telehealth. We also excluded papers which aimed to assess the level of knowledge and skills of practitioners in telehealth. Similarly, studies examining the educational needs of practitioners in telehealth were also excluded.
Since the focus of this study was to examine the reported published evidence in peer-reviewed literature, we did not include literature reported in grey literature. The searches were constrained to articles published in the English language, between 2004–2014, for which abstracts were available. We elected to review the literature for the most recent 10 years, because the rapid changes in technology in recent years and the use of such technology in health care delivery may reflect the current status of telehealth E&T which is the focus of this study. We excluded review papers, however all relevant papers contained within reviews were considered for inclusion.
Data extraction and analysis
All papers were reviewed independently by each author (SE and NRA). Disagreements were resolved by discussion. Characteristics of each study (aim, country, target group, number of participants, mode, type, level, length, provider, type of evaluation, results) were extracted. The information was then tabulated. Subsequently, the content, topics, and learning activities were explored in detail and tabulated.
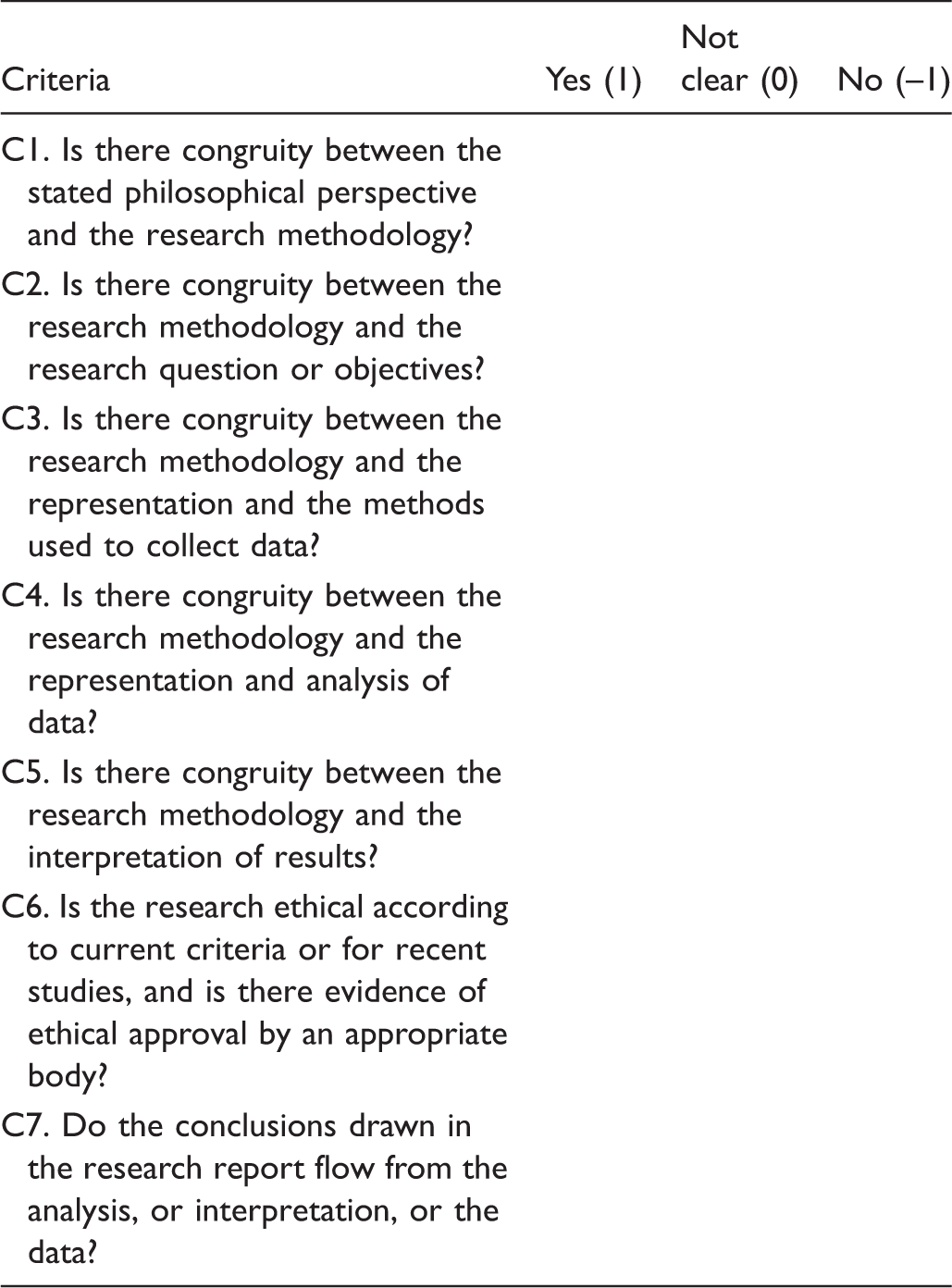
Joanna Briggs Institute Qualitative Appraisal and Review Instrument (JBI QARI) critical appraisal checklist for interpretive and critical research.
Results
The electronic searches identified 377 articles and an additional 11 were identified by the manual search. The abstracts of all 388 papers were reviewed with 30 meeting the inclusion criteria and 358 excluded. Based on full-text reading, a further 21 papers were excluded leaving a final set of nine studies for inclusion in this review (Figure 1).
PRISMA Flow Chart.
Characteristics of studies
Characteristics of included studies.

CPD: continuing professional development; JMIR: Journal of Medical Internet Research; JTT: Journal of Telemedicine and Telecare; PG: postgraduate; TJeH: Telemedicine Journal and eHealth; VHA: Veterans’ Health Administration.
Out of nine papers, eight studies aimed to evaluate some aspect of telehealth E&T. Seven studies set out to evaluate participants’ satisfaction and one study aimed to investigate the effect of a telehealth E&T program on students’ professional careers. 18 Another study examined the feasibility of a short online course in telehealth for mental health professionals. 20 The study published by Ishibashi et al. in 2011 2 4 aimed to describe the delivery of an e-Health education program to a group of participants from the Pacific Islands. All eight studies that evaluated aspects of telehealth E&T used either paper-based or online surveys for gathering information. Surveys consisted of questions with Likert scale responses and open-ended questions. In terms of results, seven studies presented outcomes of the evaluation. All seven studies indicated positive outcomes relating to participant satisfaction, relevance, feasibility, and learning outcomes. Two studies did not present results in the papers.21,24 In terms of the number of participants, all but two studies provided the numbers of study participants. Silva et al. 21 and Ishibashi et al. 24 did not present the number of participants. The total number of participants in the review was 1023.
Assessment of the quality of studies.

Type and content of E&T
Five studies described the delivery of short continuing professional studies19,20,23–25 while the remaining four described the delivery of formal university courses.
Details of curriculum.

LMS: PPT: Powerpoint; VC: videoconferencing; WHO; World Health Organization; ITU: International Telecommunications Union; ODA: Official Development Assistance.
In addition to theory and didactic learning, offerings included the development of hands-on practical skills and exposure to practical telehealth activities. One CPD course and one university undergraduate course incorporated a practical session within their E&T.18,24
How is education provided?
Five studies used online platforms as the delivery mode19,20,22,23,25 while two studies used classroom-based face-to-face delivery methods.17,24 The remaining two studies used blended learning.18,21
The duration of telehealth courses varied: university courses were based on standard university semesters while the length of CPD courses differed widely. For example, the length of CPD courses in the review was one week, 10 weeks, three months, and six months.
A range of learning activities was reported, including classroom-based lectures; brief presentations; asynchronous online presentations; live webcasts; online discussion forums, individual and group presentations; online and paper based assignments; and practical sessions. Both university courses and CPD courses have used the aforementioned learning activities. Only two studies used on-site practical sessions as learning activities in their E&T programs.17,24 The former was run as a part of a semester-based university undergraduate course, the latter was a professional development course provided to telehealth coordinators from the Pacific Islands.
Studies reported the use of a range of learning platforms, tools, and equipment. These included live videoconferencing; animation techniques; chat room facilities; PowerPoint presentations; CD and DVD technology; and photographic equipment. Two studies identified their online learning platforms (Blackboard and Moodle).18,23
Only one study specified the course fees of students. 23
Who provides telehealth education?
Universities as well as other public and private organisations were responsible for the delivery of telehealth E&T. In most cases, universities offered telehealth courses within their formal degree programs. However, as our review showed, universities were also responsible for delivering telehealth CPD courses.20,23,24 Telehealth CPD courses were also delivered by professional organisations such as health departments, or the Veterans’ Health Administration (VHA).20,24,25
Who is the education provided to?
Target groups included undergraduate and postgraduate students studying at universities, and various professional groups. Two studies described E&T for undergraduate students17,22 while one study related to the delivery to postgraduate students. 18 Another study targeted the delivery of telehealth education to both postgraduate and undergraduate students. 21 The background of undergraduate students was diverse including: physiotherapists; speech pathologists; occupational therapists; and students of a bachelor of health sciences degree. Postgraduate level telehealth courses targeted health professionals such as medical doctors, registered nurses, medical educators, and telehealth service coordinators.
CPD courses targeted a range of professionals including: health policy makers; telehealth service coordinators; medical doctors; engineers; clinical psychology trainees; nurses; public health professionals; private sector informatics professionals; and information technology professionals.
Discussion
While the enthusiasm for using telehealth as a new way of delivering health services is continuing, the lack of its integration into health systems has been a constant concern. Several studies have emphasized the importance of E&T as a key consideration.15–18 According to Ehnfors et al. the single largest dilemma for nurses and other health professionals is the identification of future core competencies that will be required to work in a technology-infused health care environment. With the introduction of new technology in health care, care processes must be re-evaluated and hence new competencies and skills may be require. 26
Educational theorists have emphasized the value of systematic instruction to deliver information and knowledge through which domain-specific problem solving skills are developed.27–29 Educational research in various domains have provided ample evidence to suggest that education is effectively used to develop these skills that are later translated into practical utility.30,31
We found a very limited number of studies in the field. Only nine studies reported the formal delivery of programs. Compared to other aspects of telehealth research (e.g. feasibility, clinical efficacy, effectiveness, economics etc.) E&T-related research has been paid scant attention. Studies included in this review were all descriptive studies examining aspects such as E&T methods, perceptions of participants, and feasibility.
This review showed that research relating to telehealth E&T has taken place in only a few countries. It is surprising that Canada, countries in Scandinavian region, Europe, or Africa where telehealth activities are substantive were not represented at all. This could be explained in many ways: it may be due to lack of telehealth E&T; or lack of interest in research relating to telehealth E&T. This may also be due to the lack of interest in reporting about E&T programs.
In fact, there seem to be some education programs in telehealth taking place in various places. For example, there are some American Telemedicine Association (ATA) accredited telemedicine training programs in the USA. The Centre for Health and Technology at the University of California and the Telemedicine Learning Center at San Diego have been providing education for a number of years.32,33 There are some private providers who offer online telemedicine education in the UK. 34 A recent report indicated that several medical schools in France have introduced telemedicine in their medical curriculum. 35 The Australian Centre for Rural and Remote Medicine (ACRRM) has been providing online telehealth modules for clinicians and practice managers. 36
This review found that there are two main types of E&T: formal university courses and CPD. These are traditional methods of providing E&T in any field and are not unique to telehealth. While higher education establishments such as universities provide more structured and conventional education focusing on degree qualifications, CPD is are generally used for providing short professional skills to practitioners.
We found that online learning was the most common approach for both university level and CPD courses. The flexibility and other advantages offered by online delivery methods may explain this choice. Online education may be particularly attractive for busy practitioners who would choose to take up short CPD courses for developing knowledge and skills. However, it also seems that practicing telehealth requires certain hands-on skills. Feedback of the participants of a telehealth practicum shows that the practical sessions helped them to develop specific skills that were relevant for practice. Also the observation of real-life telehealth consultations may be an effective way to gain exposure to the modality. Therefore, it is important to consider the value of developing practical skills through E&T too. In that sense, blended learning options may be appropriate for telehealth E&T.
The education components covered a wide range of topics, involved participants in different learning activities, using diverse techniques and learning materials. However it is unclear whether the design of curricula, learning activities, and techniques were driven by the specific needs of the participants.
The target groups of telehealth E&T in the higher education sector have included nurses and allied health professionals. However, it is also essential to educate future medical practitioners for telehealth, and this appears not to have occurred. The likely best way to provide appropriate knowledge and skills to future medical professionals would be to incorporate telehealth education as a standard component in the medical curriculum.
There may be a number of reasons for lack of interest in telehealth E&T. There are no widespread and well-established professional careers in the field and this does not attract sufficient interest within the education sector to develop and offer telehealth education programs. Lack of careers may also result in low demand from students who may fear limited professional prospects.
Conclusions
The lack of E&T to provide systematic knowledge and skills has been highlighted as a key issue. This review suggests that there is very limited published evidence relating to the delivery of telehealth E&T. Compared with research into clinical aspects and technology in telehealth, E&T has so far been paid scant attention.
Integration of telehealth involves a significant change in traditional practice, therefore requires a systematic change management approach. The provision of relevant knowledge, skills, and competencies to current and future telehealth practitioners is an important way to address this transition.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.