
Abstract
Introduction
Despite the growth of telecommunication applications to provide clinical healthcare services, there has been little attention to the pedagogical framework needed to train healthcare students to deliver these services.
Methods
In this exploratory investigation, perceptions of speech-language pathology/therapy (SLP/SLT) faculty (n = 31), graduate students (n = 16), and telehealth (“telepractice”) clinicians (n = 16) were examined with a 15-item survey regarding the 1) comparative pedagogical importance of four skills common to telepractice and face-to-face service (f2f) delivery, and 2) relative pedagogical value of seven skills and competencies unique to telepractice.
Results
Statistical analyses revealed nonverbal communication skills and knowledge of the literature related to service delivery methods were more important in telepractice than in f2f service delivery. Among seven skills unique to telepractice, participants believed the most important was solving problems related to the Internet and recommended at least two hours of instruction each in telepractice technology, patient confidentiality, and role-playing telepractice. Results suggest that SLP/SLT students may need additional and/or focused academic training in nonverbal communication, telepractice literature, and in solving connectivity issues to enter the telepractice marketplace with sufficient preparation.
Discussion
Further study is needed to compare the relative importance of additional SLP/SLT skills and competencies, describe components of effective healthcare training telepractice programs, and explore effective pedagogical strategies for healthcare telepractice instruction.
Keywords
Introduction
Communication disorders are a significant health issue, with prevalence rates between 5% and 10% of the general population.1–3 That rate is expected to rise in coming years due to hearing loss and cognitive decline associated with increased lifespans, as well as improvements in the medical management of conditions typically associated with speech and/or language disorders (traumatic brain injury, high-risk pregnancies, etc.). 4 To meet the growing demand for speech-language assessment and therapy, speech-language pathologists/therapists (SLPs/SLTs) must increasingly use telecommunication technology (e.g. web-conferencing, email, phones, wireless tools 5 ) in both healthcare and educational settings, a service delivery model known as “telepractice” by members of the American Speech-Language-Hearing Association (ASHA).6,7
The majority of speech-language pathology/therapy (SLP/SLT) telepractice clinicians have learned telepractice skills “on the job” and not in academic training programs, but this trend is changing. According to a recent study, 7 36–41% of SLP graduate programs in the US and its territories now offer academic training in telepractice applications such as live web-based videoconferencing, phone, email, and fax applications, and an additional 39% of such programs have future plans to teach telepractice to students. In Wisconsin, 14% of 108 SLPs reported having received telepractice instruction in their graduate program compared to 41% of 103 SLP graduate students who were currently receiving such instruction. 8
Despite the increase in SLP/SLT telepractice academic training programs, literature on telepractice pedagogy is sparse. Although some SLP/SLT literature provides lists of clinical skills needed to engage in telepractice 9 or describes telepractice training programs for students 10 or SLPs/SLTs in the workplace,11–13 there remain significant gaps in our understanding of telepractice pedagogy.
One major gap is that although some of the clinical skills and competencies needed in telepractice and face-to-face (f2f) service delivery are the same, it is not known if they are equally difficult to perform or equally important to employ within those models – information critical for academic training programs. For example, in both telepractice and f2f service delivery, SLPs/SLTs must be skilled in data collection, nonverbal communication skills, multiculturalism, and in literature knowledge associated with the service delivery model.9,13,14,15 However, data collection may be more difficult within telepractice because of the increased cognitive processing demands16,17 in attending to turn-taking cues and the pacing of the interaction 18 or because of the demands in developing structured written formats to collect or deliver accurate information to the client.19–21
The need for clinicians/therapists to employ nonverbal communication skills22–24 may be heightened in telepractice because it is less natural 25 for students, requiring observation of nuances in facial expression, 26 as well as understanding the effects of clothing, lighting, and amplification of nonverbal behaviours (e.g. leaning forward, frequent nodding) in web-based conferencing.26,27 Similarly, the need for multicultural competency may be intensified in telepractice because the virtual clinic can extend into diverse, underserved areas. 28 Likewise, students’ knowledge of the telepractice literature may be more important than for f2f literature so that they can address client and insurance questions about telepractice efficacy.
A second major gap is that among the clinical skills and competencies unique to telepractice, little is known about their relative importance and which should receive the most focus by academic training programs. Among the many skills and competencies unique to telepractice, some of the most frequently cited9,14,29–31 are: technology competence and confidence in telepractice applications and software; solving technology problems; developing a personal clinician–client relationship at a distance; and addressing client concerns about telepractice. Although each skill may be important for the effective use of telepractice, it stands to reason that they will differ in their relative importance. For example, technology competence and problem-solving are critical because of the need to minimize potential adverse effects of web-based conferencing service delivery and interruptions of that delivery on the completion accuracy, 32 efficiency, 18 and degree of learning 33 for assigned tasks, as well as managing the restricted pan and tilt of the camera. 28 Similarly, developing a personal clinician–client relationship may be particularly important to address because, as implied by transactional distance theory, 34 when the “teacher” and “learner” are separated by time and/or space, the dialogue is altered. Furthermore, if SLPs/SLTs are to meet the increasing need to utilize telepractice in the marketplace, it is imperative that they address common SLP/SLT perceptions of telepractice as an impersonal and ineffective delivery system, adversely impacted by the loss of direct physical contact and subject to technology failures, 23 or fears of telepractice by clients, especially those with minimal exposure to technology 28 or who may need written supplemental text cues.22,35 Despite the value of each of these skills, there is little to guide academic training programs as to their relative need within telepractice.
A third gap is that although current telepractice training programs for students10,36 or SLPs/SLTs in the workplace11–13 commonly report training students/employees in telepractice technology (applications, etc.), confidentiality, or providing some form of trial practice in telepractice, there are, as of yet, no agreed-upon guidelines for how extensive this training should be.
In summary, literature on telepractice pedagogy is urgently needed, particularly in our understanding of the relative importance of the many skills and competencies associated with telepractice. We were thus motivated to initiate an exploratory study of the perceptions and recommendations of SLP/SLT faculty, students, and SLP/SLT telepractice clinicians regarding effective telepractice instruction for SLP/SLT graduate students. Our research questions were: 1) What aspects of clinical instruction are most important when teaching SLP/SLT graduate students about telepractice service delivery? 2) How many hours of instruction should SLP/SLT graduate students receive in telepractice technology, confidentiality issues pertinent to telepractice and the Internet, and in telepractice role-playing?
Methods
To address these questions, we developed a 15-item survey (four demographic, three open-ended, and eight Likert content questions) within Survey Monkey. (The three open-ended questions provided the context for a future qualitative study and are not considered in the current investigation.)
Survey development
The current investigation focused on the eight Likert content questions, four of which explored whether data collection skill, nonverbal communication skill, multiculturalism competency, and knowledge of literature pertinent to the delivery system were more (or less) important in telepractice than in f2f service delivery. In the fifth Likert question, we addressed the relative importance of seven skills and competencies unique to telepractice: technology competence; solving technology problems; developing a personal clinician–client relationship at a distance; addressing client concerns about telepractice; telepractice concerns and fears of SLPs/SLTs; managing the tilt and pan of the camera; and providing written text cues. Three Likert questions explored the recommended number of training hours in technology, role play, and confidentiality. Although many skills and competencies are needed for telepractice, we selected these for this initial investigation because they were frequently discussed within the best evidence resources in patient care for SLPs/SLTs9,14,16 and additional questions would likely have significantly reduced the survey’s completion rate. 37
The survey was piloted by two SLP/SLT faculty, each with two semesters of experience instructing graduate students in telepractice. No significant changes to the survey were proposed. Invitations to participate in the study were then sent by email to approximately 3900 potential participants, including ASHA Special Interest Groups (SIGs) (Voice and Voice Disorders; Higher Education; and Telepractice) and authors of journal articles and presentations on telepractice in speech-language pathology. Respondents had 10 weeks to respond to the survey, available during the winter of 2013. Reminder notices were posted on the SIG listserves at both four and seven weeks following initial posting of the survey.
Participants
Demographic characteristics of participants (n = 63).
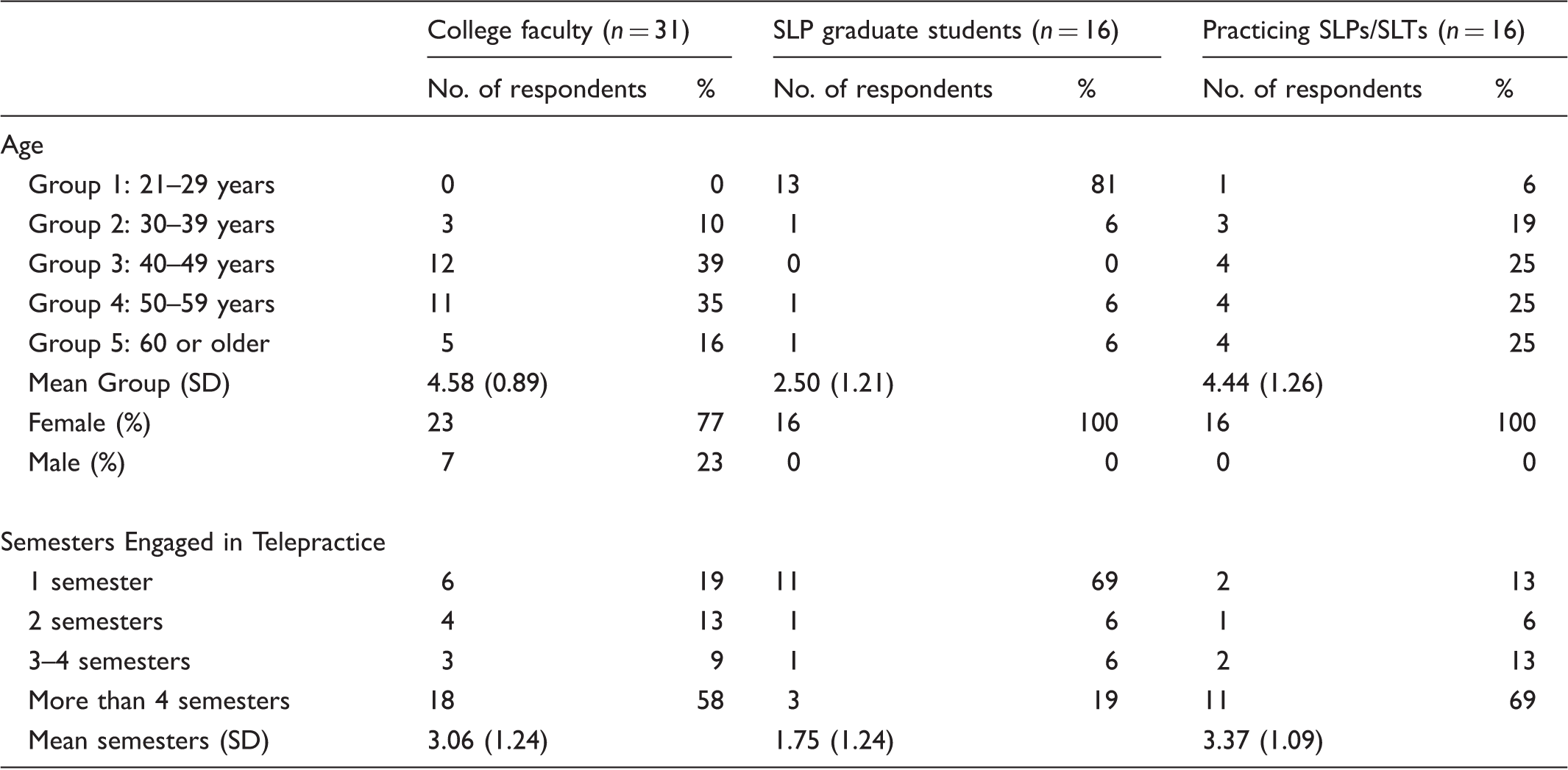
SLP/SLT: speech-language pathologist/therapist; SD: standard deviation.
Analysis
The comparative difficulty/importance between telepractice and f2f service delivery for the four selected skills and competencies common to both delivery systems were analysed with a Kruskal–Wallis H-test because of their ordinal rankings. Comparisons of the relative pedagogical importance of the seven selected clinical issues unique to telepractice were obtained with a chi-square test of goodness-of-fit comparing weighted mean (WM) differences of the ranked responses. WMs were calculated by applying a single numerical value (1–5) to each Likert description (e.g. with “More than 4 hours” being given a weight of “5” and “Less than 1 hour” being given a weight of 1), and then calculating the mean. WMs were calculated to identify the recommended number of training hours in technology, role play, and confidentiality.
Results
Question 1: Most important aspects of telepractice instruction for SLP/SLT students
Importance and difficulty of tasks in telepractice compared to face-to-face sessions.
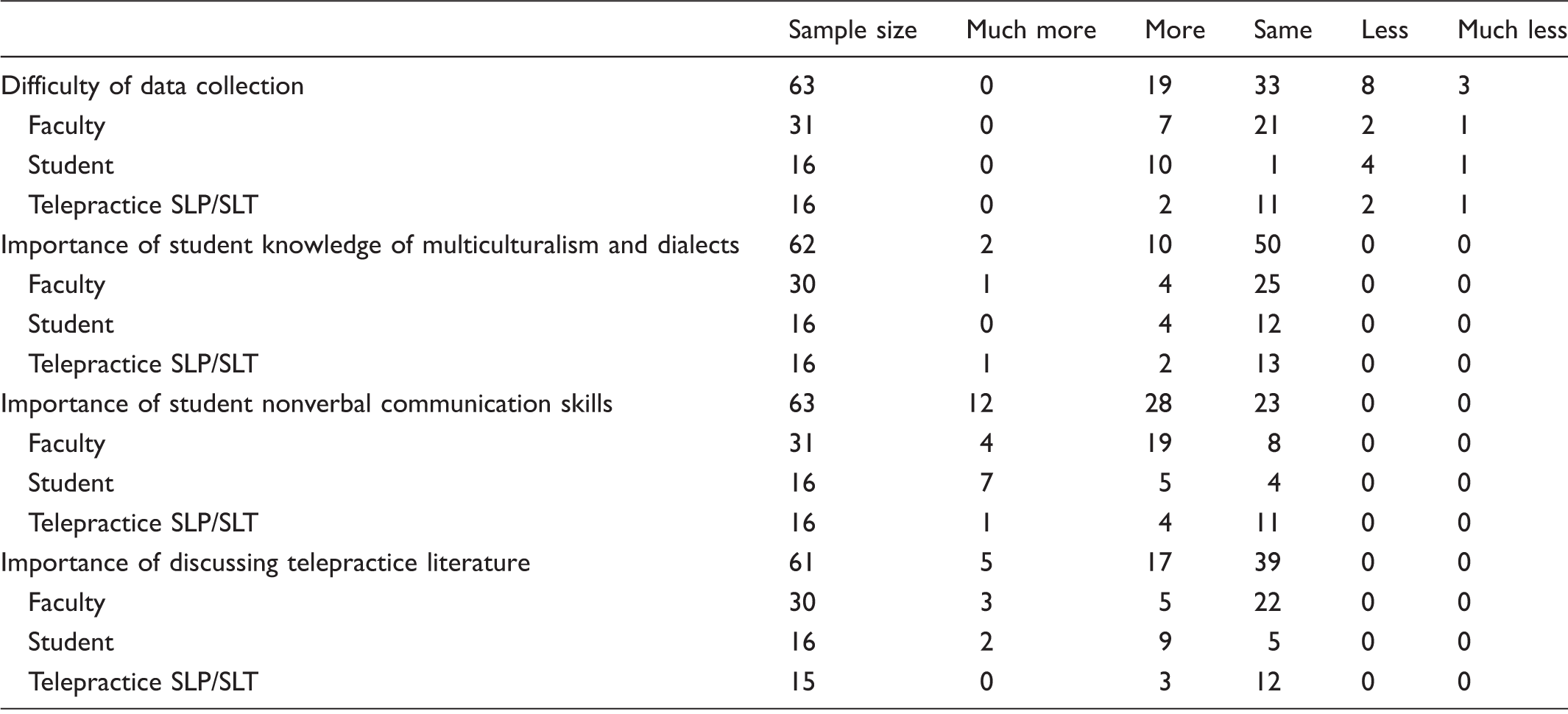
SLP/SLT: speech-language pathologist/therapist.
Likert scale rankings and weighted means of telepractice issues.

Weighted mean calculation: 1–5 scale with “More than 4 hours” weighted “5” and “Less than 1 hour” weighted 1.
SLP/SLT: speech-language pathologist/therapist.
Question 2: Hours of instruction needed in technology, confidentiality issues, and telepractice clinical role-playing
Hours of training students need in telepractice.

Weighted mean calculations: 1-5 scale with “More than 4 hours” weighted “5” and “Less than 1 hour” weighted 1.
SLP/SLT: speech-language pathologist/therapist.
Discussion
Because of the number of SLP/SLT academic telepractice training programs is growing, there is a need for investigations exploring telepractice pedagogy. Although ASHA has described many skills and competencies SLPs need to deliver telepractice clinical services,9,14,16 it is unclear which, if any, of these skills and competencies might require additional attention by academic training programs. In this exploratory investigation, we examined participants’ perceptions of a small subset of those skills and competencies, exploring their comparative importance in f2f service delivery as well as relative importance to each other. Participants believed that, compared to f2f service delivery, academic training programs should pay increased attention to teaching students: the nuances of nonverbal communication skills; literature associated with this service delivery model; solving problems associated with the Internet; and possibly how to address clients’ fears about telepractice.
The relationship between providers’ nonverbal communication skills and client outcomes in healthcare service delivery is well-documented,39–43 affected by proxemics (physical distance), kinesics (body movements such as head nodding and facial expression), and paralanguage (communication elements such as speech rate, prosody, and volume). 39 Our results imply that academic training programs may wish to consider providing students increased focus on nonverbal communication skills. Given that nonverbal behaviours account for approximately 55–65% of interpersonal communication,42,43 the additional nonverbal demands in telepractice (e.g. understanding how dialogue and turn-taking are altered by physical distance; how cameras in web-conferencing adversely accentuate aspects of clothing, jewellery, lighting, and head-nodding) may heighten the importance of this skill set. Because competent nonverbal communication is fundamental to the development of clinician–client trust and rapport, 43 allowing the clinician to project confidence in the treatment she is providing, 27 such additional focus when there are increased demands is not an unexpected finding.
Understanding the literature associated with telepractice was found to be a more important competency than understanding the literature associated with f2f service delivery. The reasons for this apparent difference were not explored in this survey but perhaps knowing the literature associated with telepractice could assist SLPs/SLTs with reimbursement challenges, a major barrier to telepractice implementation by SLPs/SLTs,14,44 or in educating potential clients about the efficacy of telepractice. Another potential reason for this belief could stem from reports that knowledge of the telepractice literature assists the SLP/SLT in the development of functional client goals for telepractice clients. 45
Among the seven skills and competencies surveyed unique to telepractice, participants believed the most important to teach was solving problems related to the Internet connection (e.g. interrupted Internet access, delays in transmission, computer failures, dropped signals), and suggested that students should receive, on average, two hours of technology “problem solving” instruction to address these issues. Major limitations in telepractice applications, particularly video-conferencing, have been reported, including, but not limited to, problems of low bandwidth, network congestion, variability in audio and video quality, as well as delays in the audio/video signals. 31 Because a major barrier to the expansion of telepractice in the healthcare marketplace is SLPs’/SLTs’ limited ability to manage technological challenges and failures,30,46 additional attention to this skill in academic training programs may have merit but additional studies are needed to ascertain whether two hours of instruction is sufficient and/or effective.
Although statistical significance for addressing client fears and concerns about telepractice was not reached once correction for Type I error was applied, the high value for the WM obtained for this skill suggests SLP/SLT training instructors may wish to address it with their graduate students. Some clients, such as young children, may be comfortable with the technology used in telepractice while older adults (60 years old or more) may rarely use computer technology 47 or may be anxious about using it. 45 However, although “digital fluency” may be related to psychological factors such as anxiety, which may prevent older adults from using technology, students should appreciate other variables such as education, socioeconomic status, and accessibility, which may also play a significant role in clients’ comfort with technology. 48
Published telepractice pilot training programs include telepractice aspects of confidentiality as related to HIPAA 38 and practice (i.e. role playing) of telepractice, but it is often unclear how much training is provided in these areas. Our findings, though limited to “educated guesses,” revealed participants believed students should have approximately two hours of instruction related to confidentiality and HIPAA. 38 However, with the increasing availability of non-secure platforms with which to utilize telepractice, it is possible that two hours could be considered a minimum. Similarly, we also found that two hours of practice (via role playing) is recommended before students implement telepractice with clients.
Limitations and conclusions
There are significant limitations to this investigation, including a small sample size largely restricted to members of the ASHA. Moreover, the skills and competencies reviewed in our survey were limited to a subset of a substantial number found in the literature, requiring considerable caution be taken in appraising these results. Importantly, this was an exploratory investigation limited to only perceptions of the participants. Empirical studies are needed to provide evidence of critical differences between the skills and competencies needed in telepractice versus f2f service delivery, the true extent of skills training needed, and the most effective pedagogical strategies in which to teach them.
Nevertheless, these data provide preliminary context to reports that telepractice demands additional training than does training for f2f service delivery. SLP/SLT academic training programs may wish to consider providing students additional training in nonverbal communication, telepractice literature and research, solving problems in Internet connectivity, and possibly communicating with clients who are wary of technology and/or telepractice.
Footnotes
Acknowledgement
The authors gratefully acknowledge the statistical advice and support of James Schreiber, PhD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.