
Abstract
Background
Access to dental care is important for overall health, but can remain problematic for those in rural or isolated locations. It can be difficult to encourage clinicians to choose or continue a rural health career. Teledentistry is showing some promise as a strategy to support rural, isolated and new health care workers. This study aims to explore the quantitative and qualitative framework associated with teledentistry in an effort to uncover the interaction of multiple influences on its delivery and sustainability.
Methods
A systematic search of the literature was undertaken and studies were included if they evaluated consultative teledentistry, reports on implementation of teledentistry in practice or attitudes to teledentistry. Studies were evaluated qualitatively.
Results
Thirty-nine studies were included focusing on the accuracy, effectiveness or description a teledentistry project in practice. Five main themes were identified in the qualitative analysis: (1) using information and communication technology (ICT), (2) regulatory and system improvements, (3) accuracy of teledentistry, (4) effectiveness, including increasing access to clinical services, efficiencies and acceptability, and (5) building and increasing clinical capacity of the dental workforce.
Conclusion
Teledentistry provides a viable option for remote screening, diagnosis, consultation, treatment planning and mentoring in the field of dentistry. Rapidly developing information and communication technologies have increasingly shown improving cost effectiveness, accuracy and efficient remote assistance for clinicians. There is high acceptability for teledentistry amongst clinicians and patients alike. Remuneration of advising clinicians is critical to sustainability.
Introduction
Access to a dental practitioner is important for prevention and treatment of dental disease, as good dental health contributes to overall quality of life. 1 Despite increases in training places worldwide for dentists and oral health professionals, dental care in the majority of countries, is provided by private general practitioners who tend to be concentrated in affluent suburbs or city centre sites, meaning obtaining dental care can be difficult for those living in disadvantaged areas or rural locations.2,3
Recruitment and workforce sustainability are often an issue and some countries with large sparsely populated rural areas have grappled with how to overcome medical and dental provider shortages in these rural areas. Various government policies to encourage clinicians to consider a career in a rural location have included financial incentives, providing ongoing professional development, mentorship schemes and subsidising travel to professional development meetings have all been shown to increase the recruitment and retention in the short term.4–7 However, making sure that inexperienced, newly qualified dental and oral health practitioners, working in rural and remote locations, have adequate clinical advice and support can be difficult to organise on a sustainable basis.
It is clear that more targeted support is required to ensure that new practitioners in rural locations have the advice and support they need to avoid feelings of isolation and stress. There is increasing evidence that teledentistry could support a program of advice and education for rural dental practitioners and serve rural communities by providing access to specialists previously unattainable.
The rich literature in telemedicine has been shown in over 80 systematic reviews that have indicated that it can be an effective model for providing healthcare advice and help with treatment planning. A recent overall assessment of these reviews has found that the technology is still expanding, but more focus is needed on patient perspectives, economic evaluation and innovation. 8
As an adjunct to telemedicine, recent quantitative systematic reviews on teledentistry have shown that it can be effective for different dental specialties and it is a useful adjunct to some clinical applications.9,10 However, its implementation into practice is still largely not understood. In this study, through the use of qualitative research methodology, for the first time in this area, we aim to uncover a broader narrative to delineate the personal and social forces that impinge on teledentistry affecting its delivery, sustainability and evaluation in dental services. Qualitative research methodology has the ability to capture these narratives and their context and derive practical guidance to support future program development.
Methods
A systematic search of the literature was undertaken to find articles on the use of telemedicine in dentistry according to the PRISMA statement guidelines for reporting systematic reviews. 11 Teledentistry was defined as using communication technology to relay diagnostics or treatment information in seeking advice, direction, supervision and/or mentoring in the treatment of dental diseases, between two or more clinicians using a purposeful integration of information technology.
Articles were included if the study utilised telemedicine techniques within dental practice in both general and specialist dental settings and if there was a research question about consultative teledentistry, it reported on attitudes to teledentistry (health professional or patient) or it provided a clinical description of teledentistry in practice. No limits were placed on study type or language. Studies were excluded if they were about telemedicine only, editorial only, animal studies, used information technology for people outside dentistry, non-clinical scenarios such as patient to patient communications, one way communication only such as online education, reports on prospective ideas and futuristic speculation (including protocols). Conference presentations were not included, unless further information could be gathered from the authors. Descriptive studies were included in an effort to provide completeness of data for qualitative assessment of the literature.
Search strategy
Literature searches were conducted in MEDLINE, Embase, CINAHL, PsychINFO, AMED, EBM Reviews, ERIC, Global Health and PREMEDLINE databases. We also searched the grey literature. Reference lists in all included articles were also searched.
Database searches were conducted on 5 January 2015 and typical search strings are provided in Appendix A. All databases had no limits placed by year or language. The EndNote reference manager (Version X7.2, Thomson Reuters, released September 2014) was used to store and view retrieved references.
Two authors screened titles and abstracts and excluded those studies which did not meet the inclusion criteria. The full texts of relevant studies were independently reviewed by the research team for inclusion and any disagreements were resolved through discussion.
Quality assessment
A modified Downs and Black criterion scale, which examines validity, bias, power and other study attributes, was used to assess the methodological quality of the included papers. We modified the original Downs and Black scale, 12 as described and recommended in prior methodological systematic reviews, 13 to exclude items that were not applicable to the designs of eligible studies. For example, items specific to randomised trials were removed for observational studies. A percentage quality score was calculated by dividing the total score received by the maximum score possible for each study. Meta-analyses were not undertaken because of the clinical heterogeneity and differences in measurement outcomes in the included studies.
Data extraction
Data extraction was undertaken independently by the team using a specified data extraction form. Studies were categorised by their outcome measures as either ‘accuracy’ or ‘efficiency’ of Teledentistry to assist in analysis. Accuracy was defined as; the evaluation of precision of methods in teledentistry, e.g. comparing caries detection through teledentistry and in-person diagnosis. Effectiveness was defined as; the evaluation of the efficiencies of teledentistry, for dental practices as well as the satisfaction rates for participants involved, such as time and travel advantages. A qualitative data analysis was undertaken of all included studies, through thematic synthesis of the results and conclusions. For each paper all text under the headings ‘results/findings’ and ‘conclusion/discussion’ were entered verbatim into Hyperresearch 2.8.3 (ResearchWare Inc., Randolph, MA) software. For each study, two authors independently coded the text and recorded concepts that focussed on all aspects of conducting teledentistry for patient care. A grounded theory approach, 14 including a negative case analysis, 15 was used in the analysis to achieve a higher level of analytical abstraction, the concepts were examined for similarities, variations and relationships with one another. This informed the development of an analytical schema of themes. Whilst we were interested in understanding the domains of satisfaction in teledentistry, the themes were still allowed to develop deductively, they were not set ‘a priori’ to ensure that all aspects of teledentistry were analysed.
Results
Literature search and study characteristics
Our search yielded 6898 citations, of which 1705 were duplicates and excluded. 5111 were ineligible after title and abstract review. The majority of these studies were excluded for not using information communication technology, information technology not used clinically and unidirectional communication. Of the potentially eligible 82 studies, 39 studies involving 4290 patients were eligible for inclusion in the review after full text analysis (Figure 1). Nineteen studies focused on the accuracy of teledentistry, 10 studies focused on the effectiveness of teledentistry and 10 studies provided case studies or clinical reviews.
Flow chart of search results and selected studies.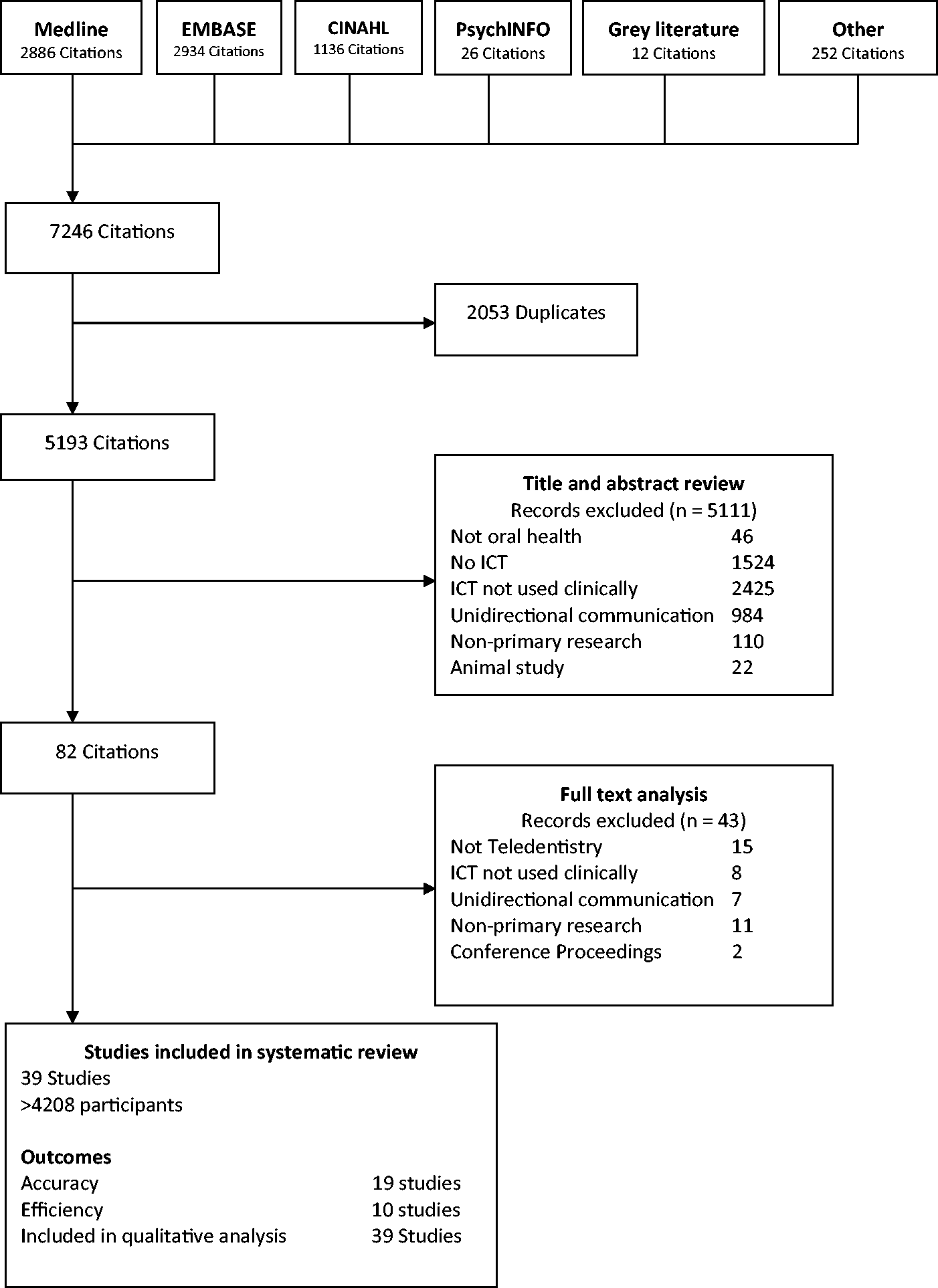
Demographics of included studies
Demographics of included studies.

Quality appraisal
Quality rating, based on the modified Downs and Black criteria, were scored on a criteria out of a possible 33. Scores ranged from 17 (51%) to 28 (85%) with an average of 23 (70%) for studies assessing accuracy of teledentistry and ranged from 16 (48%) to 28 (85%) with an average of 22 (66%) for studies assessing effectiveness of teledentistry. The overall average, for all studies was 23 (69%). In general, quality ratings were lowered because studies did not: (1) describe principle confounders; (2) have good follow-up; (3) describe characteristics of patients lost to follow-up; (4) describe those who were ineligible or refused to participate; (5) report a power calculation; (6) ensure the measurers were blinded; or (7) report 95% confidence intervals or actual probability values for main outcomes. The majority of studies were descriptive and this created difficulties in assessing the quality of these papers against rigorous methodological checklists.
Summary of study results
Results for teledentistry studies with the outcome assessment of accuracy.

Outcomes of included studies on effectiveness of teledentistry.

Qualitative synthesis of findings
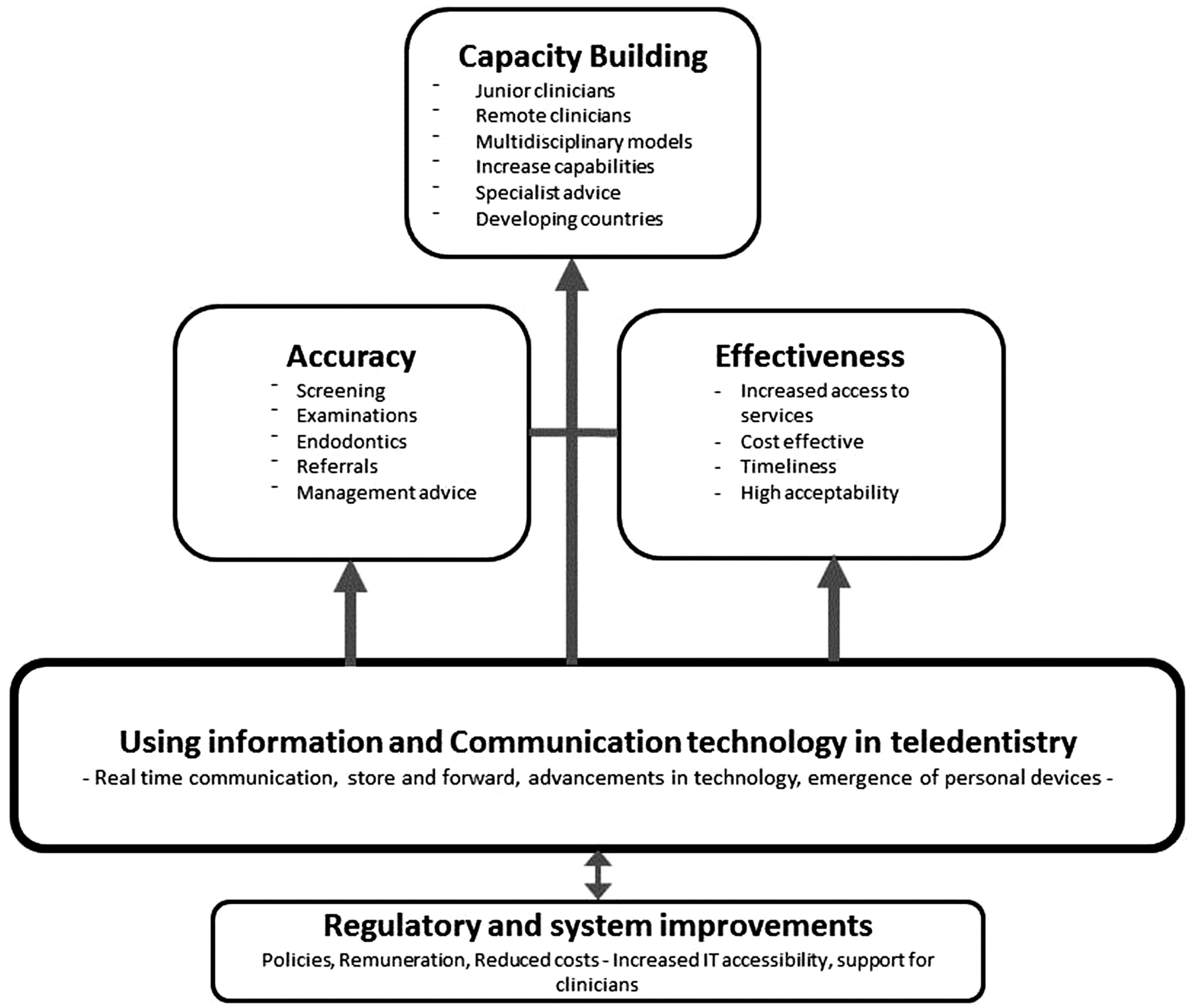
Five main themes were identified in the qualitative analysis on the application of teledentistry in dental practice. The themes were:
using information and communication technology in teledentistry; regulatory and system improvements in teledentistry; accuracy of teledentistry; efficiency of teledentistry, including increasing access to clinical services, efficiencies and acceptability; building and increasing capacity of the dental workforce (Figure 2). Thematic schema – information and communication technology is the backbone of teledentistry which is continually improved over time, leading to accuracy and efficiencies of teledentistry which enables capacity building in dentistry.
Theme one: using information and communication technology in teledentistry
All studies noted that information and communication technologies world-wide have developed over time and become less expensive, and as a consequence clinicians find it cheaper and simpler to use these technologies to undertake teledentistry.
Whilst there are some examples of large trials of teledentistry involving complex information technology systems in the studies included in this review,19,25,28,38,39,54 many teledentistry programs, especially recently, utilise the emergence of personal internet connections, smart phones and personal computers to gather, store and forward the required data. Many studies used the simplicity of an email system with photographic and/or radiological attachments between remote sites to great effect.
The studies used a wide variety of clinical cameras to convey intra-oral and extra-oral information to the involved communication partners. Many studies suggested that the use of high tech intra-oral camera required extensive training for the user, with some studies suggesting the use of smart phones could overcome this training barrier and also reduce paediatric aversion to unfamiliar equipment, although, it is important to ensure patient privacy is maintained under this model.
There was a distinction made between teledentistry programs that used real-time communication between relevant parties and store and forward methods, where written, radiological and/or photographic information was stored and then forwarded between parties as the method of communication. Some studies used either or a combination of both. Both have their relevance in a teledentistry program, with the method chosen based on the type of dental service provided and expected outcomes. Primary care services in dentistry could benefit from using email and store-and-forward image system. Such a system could provide a screening approach to organizing a referral system for patients requiring specialty services in the field of oral medicine.
49
Telemedicine by smartphones has also been used by the authors to view postoperative images the night of the (oral) surgery, thus making the morning rounds more efficient.
17
Theme two: regulatory and system improvements in teledentistry
All studies discuss the suggested regulatory and system improvements, to progress teledentistry programs and applications in the future. Many authors discussed how teledentistry had been shaped and modified during the project’s course as the team learnt about the process and overcame barriers that project developers faced over time. These studies suggested that if long-term sustainability of teledentistry is to be realised then regulatory barriers such as remuneration for the clinical team, would need to be overcome – often there is limited finance for teledentistry advisors to be acknowledged and reimbursed for their time.
The majority of studies suggested that support systems are crucial for integrating teledentistry into the clinical environment. This included both supporting policies and procedures, dedicated personnel to assist, and secure integrated and compatible electronic health records. Some studies indicated that on occasions policy updates struggle to keep up with technology updates and this created some tension when providing services via teledentistry. Personnel available to the clinicians, on the ground, to provide information technology support for the new systems and familiarity with the technology being used in the teledentistry program prior to being used clinically were found to be extremely beneficial. … All United Kingdom NHS dentists are busy and work on a highly structured time of service payment system. …. There was no financial compensation for the time spent by dentists capturing the images of their patient records and putting together the whiteboard and transmitting the information.
46
Recent legislation in California, AB415 recognizes that technology has evolved to be a useful tool in several fields for expanding access to healthcare. However regulatory barriers and reimbursement issues still need to be addressed in dentistry as in other fields as the movement towards telehealth advances.
42
The results from this project indicate that the ISDN-based systems provide invaluable support for clinical decision making in time critical contexts, its major drawback is expense, both in initial purchase and equipment maintenance.
44
In this research, data obtained on dental caries through remote diagnosis were similar to those obtained by traditional visual inspection. This finding can be especially useful in telehealth activities through the use of relatively low cost tools such as digital cameras and personal computers with internet-based connections.
41
Theme three: ‘accuracy’ of teledentistry
Of the studies that evaluated the ‘accuracy’ of the teledentistry, the majority reported it was as reliable as face to face clinical observations in a range of settings, including; screening, orthognathic examination, orthodontic treatment, remote detection of root canals, indications for oral surgery, diagnosis of orofacial diseases, and management of dentogenous infections. One study reported that it was difficult to diagnose the extent of demineralisation accurately through teledentistry;
51
and another reported low kappa agreement between face to face and teleconsultation for soft tissue changes.
54
Most considered on-site examinations as the gold standard comparison and the studies reported sensitivity, specificity/positive/negative predictive values (Table 2). Our data strongly suggest that oral screenings of preschool children conducted by means of teledentistry are comparable to traditional, visual oral examinations conducted in-person by a dentist.
33
Information technology could increase the accuracy of consultations because it allowed specialists to view and review digital imaging outside a medical centre quickly and easily.
49
Since the results showed an almost complete agreement between teleconsultants regarding the therapy (K ≥ 0/892), there is the possibility to help remote clinicians with decision-making.
39
The results of this study make it clear that a dentist can make a valid judgment … based solely on a virtual exam from complete records provided by allied dental personnel in the field.
42
Theme four: effectiveness of teledentistry
The majority of the studies reported to some degree on the effectiveness of teledentistry services. These included; increased access to clinical services, cost savings, timeliness and a reported high acceptability among clinicians, patients and caregivers. Some studies reported teledentistry resulted in increased efficiency after a familiarisation period with the technology.
Teledentistry increases access to clinical services for patients
Overwhelmingly, studies reported an increased access to clinical services for patients through the use of teledentistry. This was particularly relevant for remote communities and vulnerable patients. Teledentistry was found to enhance the continuity of care in many situations and in some circumstances was found to be able to increase preventive oral health behaviours when used in an oral health promotion. Its use improved access to specialist care as well as access to general dentists. Teledentistry assists community health professionals, or in some cases child care workers to provide images to be reviewed and screened for the needs assessment and prioritisation for dental services. Similarly general dentists can use teledentistry to request advice from and referral to specialist dentists. The major outcome from the teledentistry field trial was the successful delivery of alternative models for paediatric oral health services provision for regional Victoria. This demonstrates that teledentistry can be a highly effective mechanism for enhancing early diagnosis and referral for patients who might otherwise not receive care.
24
…videoconferencing thus seems suitable for long distance consultation in dentistry. It has the potential to increase the total number of dental specialist services in sparsely populated areas in Finland.
31
Efficiencies and acceptability of teledentistry
With the increasing widespread availability of cost effective information technology, many studies reported that the technology required for teledentistry is effectively a low cost exercise and the costs associated are quickly counterbalanced by the savings in both time and travel for clinicians and patients who would otherwise have to travel long distances for consultations. Studies reported that delays for clinicians were minimised with reduced numbers who failed to attend appointments and greater numbers of patients being able to be seen in a clinical session. The immediacy of ‘live’ teledentistry was seen as a real advantage for clinician and patient alike in decision making and resulting access to care.
Some studies reported greater efficiencies in referrals for specialist care. These studies reported an increase in referrals for patients who might otherwise not have received specialist care, and some studies reported a decrease in the number of inappropriate referrals, due to education and assistance to referring practitioners.
Overall, there was a high level of acceptability of teledentistry reported in many studies; with patients, children, parents and clinicians indicating efficiencies in the delivery of healthcare. There was willingness to interact with the technology used in teledentistry, especially among young children. Surveys consistently reported high overall acceptability from patients and clinicians. Though, where teledentistry replaced an already functioning referral system there was some reluctance to utilise a new process.25,46 SFMTS [Store and Forward telemedicine System] resulted in 50% less lost working time. We reduced the first visit to the hospital for this pathology in 29.1% of patients and the mean time elapsed until treatment onset by 76 days.
35
The 10 cases discussed represented uncomplicated clinical entities that might be considered problematic for a non-specialist. Normally all 10 of these patients would have been referred to a consultant, but as a result of the telemedicine rounds, it was only necessary to refer two of them.
20
Additional results reported by school administrators were that students and families faced fewer transportation issues, had lower cost for care, appreciated flexible appointment scheduling, faced reduced language barriers, and had an easier time getting dental care for young children and individuals with behaviour challenges or complex medical problems.
55
In addition, the process of obtaining images in non-invasive and less stressful for small children than the usual oral examination. We have noticed that all children like seeing their teeth on the computer screen. Dental imaging appears to be seen as play for them.
33
Theme five: capacity building
Many studies reported that teledentistry was an excellent tool to build the clinical capacity of clinicians through a variety of supportive environments and learning experiences. This was especially true for junior and/or remote clinicians. This could include; education sessions, professional development forums, multidisciplinary health models, shared patient responsibility and peer support. New graduates or junior staff particularly reported that support from senior clinicians via technology was advantageous. Teledentistry was reported to be able to increase the ability of the remote dental team to provide treatment beyond their initial capacity and were able to increase specialist dentistry services. Some studies reported the use of teledentistry to support dentistry in developing countries, to educate and support these dental health workers who have varying levels of oral health care training. The teledentistry assisted, affiliated practice dental hygienists benefit by being allowed to perform preventive services they are licenced to provide in a mid-level practitioner model that promotes additional employment choices and professional opportunities.
47
The value of SOMNet [teledentistry program] for the majority of participants is access to external expertise and, in the end, better care for patients, in addition to a means for continuing education.
29
The teledentistry pilot model suggests that a centrally located dental school can provide dental care to patients in remote areas and educate remote interns, much as if they were at the school.
23
Telemedicine consultation is a vital patient-management tool of key importance to any field clinicians or those in geographically remote regions, but also to clinicians who are not specialised enough…
39
Discussion
In using qualitative research methodology in this systematic review of teledentistry, we have bought a new insight into the positive and negative aspects of bringing a teledentistry program to fruition. The themes in this study provide a rich source of information and advice for policy makers, health service managers and clinicians. We have found that modern teledentistry programs are cost effective and use readily available already daily-integrated technologies. Teledentistry has the ability to increase access to dental care and specialist advice for patients. Teledentistry is reported as having a high acceptability by clinicians and patients due to the efficiencies it provides including; time, travel and cost effectiveness for all parties, reduced appointment waiting times and reduced wasted clinical time for practitioners. Teledentistry also provides extensive opportunities for capacity building of clinicians, especially new or recent graduates.
Information technology is expanding and improving at a fast rate and the integration of technological innovations in our daily lives provide opportunities for integrating these into a wide range of teledentistry activities potentially lowering the costs for training and support as well as for acquisition if privacy concerns can be overcome for personal device usage. The ability of smartphones to take high quality photographs for remote diagnosis and provide a method of communication through video or teleconference applications has reduced costs and availability of tele-health programs dramatically, although care should be taken to ensure transmission and storage of any patient information is secure. What is of concern is that many teledentistry programs are aimed at supporting rural and remote patients and clinicians, yet this population has the poorest access to a reliable internet connection in many countries. Government agencies must help remote communities join the communication revolution in an effort, not only to support the community members, but it is essential to provide support to the rural healthcare workforce.
The ability for teledentistry to build capacity, for the increased provision of quality dental care in rural and remote clinical practice is by far one of its greatest strengths and harnessing this technology for this purpose is achievable. However, access to costly and hard-to schedule specialists in rural areas can also benefit from the implementation of teledentistry, especially for screening purposes. Providing professional and personal mentoring by giving expert advice to clinicians to build their capacity to provide a wide range of dental treatment has been found to be a useful strategy in the retention of healthcare workers in rural/remote locations.5,6 The option to provide this support through a teledentistry program should be explored. The capacity for similar programs to support a new graduate program regardless of location should also be explored as programs can be delivered relatively cheaply.
Suggestions for program coordinators
The qualitative analysis in this study has generated some pertinent information that could be of value to health service administrators charged with the task of supporting and/or developing a teledentistry program for use in improving quality and access to dental care for their community. The key points were as follows:
Technology has developed so rapidly that smart phones and mobile devises are the easiest and cheapest way to set up teledentistry schemes. Synchronous consultations are difficult to organise for busy specialists, so it is essential to build in a system whereby clinical questions can be answered in a convenient time. The store and forward option is the most straight forward option to trial teledentistry programs. Teledentistry programs will not be sustainable unless organisations build in remuneration for both the specialists and the referring practitioners. Indeed funded designated advice sessions could be used for teaching as well as diagnosis. There is evidence that teledentistry reduces costs for the referring dental team, patients and carers, further reinforcing the necessity to ensure that clinical staff providing advice are given adequate financial incentive to maintain the service. Clinical capacity building for clinicians and allied staff is possible and post-graduate trainees can increase their utilisation of teledentistry to help them improve their knowledge and skills without having to travel to a central location. Indeed online learning coupled with real-time teledentistry certainly needs to be explored by health service and educational researchers.
Limitations
There are limitations in this study, mainly stemming from the fact that the majority of included studies were only rated as being of fair quality. The majority of the studies expressed optimism about the teledentistry programs, but there is a high chance that there is some publication bias as all studies reported at least one positive result for accuracy or effectiveness. Programs involving teledentistry that are not successful are more likely to be abandoned well before they have the opportunity to be published. Adding to this, the majority of the studies were reported on by the developers of the programs, creating a possible opportunity for a bias in reporting of the results included from the studies. Very few studies used the same outcome measure, making meta-analysis of the data impossible. This is the advantage of a qualitative review as it has the potential to explore multiple contexts of the programs through qualitative synthesis, creating a more meaningful understanding of the development of a teledentistry program in the future.
Conclusions
Teledentistry provides a viable option for remote screening, diagnosis, consultation, treatment planning and mentoring in the field of dentistry. Rapidly developing information and communication technologies have increasingly shown improving cost effectiveness, accuracy and efficient remote assistance for clinicians. There is high acceptability for teledentistry amongst clinicians and patients alike, through efficiencies in time, travel and costs, which offers reduced appointment waiting times for patients and less wasted clinical time for practitioners. One of the most promising aspects of teledentistry is the ability to provide mentoring for recent graduates which can be provided at a relatively low cost. Teledentistry programs need to ensure that systems are in place for remuneration of advising clinicians, and there is sufficient program, structural and personnel support for the staff implementing new schemes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.