
Abstract
Introduction
Since 2002, the Ontario Telestroke Program has provided hospitals in under-served regions of the province the opportunity to offer intravenous thrombolysis with tissue plasminogen activator (IV tPA) to eligible patients. The purpose of this study was to determine whether telestroke-assisted IV tPA patients had similar risks of 7- and 90-day mortality, symptomatic intracerebral haemorrhage (sICH), and poor functional outcome compared to patients who received IV tPA with on-site expertise.
Methods
Data from two audits of patients with acute ischaemic stroke hospitalized in Ontario, Canada in 2010 and 2012 were analysed. We modelled the risk of all-cause death within 7 and 90 days of receiving IV tPA using proportional hazards adjusting for hospital type, patient characteristics, and whether IV tPA was administered as part of a telestroke consultation. Outcomes of sICH and modified Rankin Scale ≥ 3 at discharge were modelled using generalized estimating equations adjusting for the same variables used in the mortality model.
Results
There was no difference in 7- or 90-day mortality among those who received IV tPA with telestroke (n = 214) compared to those without (n = 1885) (7-day adjusted hazard ratio (aHR) 1.29 (95% confidence interval (CI) 0.68, 2.44); 90-day aHR 1.01 (95% CI 0.67, 1.50)). Complications were similar between groups, with an adjusted odds ratio (aOR) for sICH of 0.71 (95% CI 0.29, 1.71) and an aOR of 0.75 (95% CI 0.46, 1.23) for poor functional ability at discharge.
Discussion
Patients receiving IV tPA supported by telestroke had similar outcomes to those managed with on-site expertise.
Introduction
Telemedicine is a process of leveraging information and communication technologies to improve access to health services and specialists in under-served regions. In the province of Ontario, Canada, the Ontario Stroke Network (OSN) oversees an integrated and regionalized system of stroke care that includes the Ontario Telestroke Program (OTP), a telemedicine application using videoconferencing and remote review of brain imaging to increase patient access to intravenous thrombolysis with tissue plasminogen activator (IV tPA) at hospitals where on-site neurologist availability is limited or non-existent. 1 IV tPA is a time-critical intervention with guidelines that recommend administration within 4.5 hours of symptom onset to be effective. This intervention comes with serious risks such as secondary brain haemorrhage and is performed only on patients with confirmed ischemic stroke. Access to clinicians with stroke expertise via telemedicine in hospitals without on-site neurologist support enables timely assessment, diagnosis, and treatment.
The OTP is similar to telestroke programs in the UK and Australia, where consulting stroke neurologists located at a number of regional stroke centres (RSCs) provide coverage to all referring hospitals (network model), unlike other telestroke programs that have a single Comprehensive Stroke Centre providing support to surrounding referring hospitals (hub and spoke model).2–5
The program provides emergency department (ED) physicians in hospitals located in both urban and remote regions of the province with rapid access to stroke specialists 24 hours a day, seven days a week, and supports a “drip and stay” protocol (the patient remains at the hospital where treatment is initiated and is not transferred to a stroke centre).
In a meta-analysis examining the safety of IV tPA administered as a result of a telestroke consultation, the authors concluded that this mode of delivery is safe and effective when given within three hours of symptom onset. 6 Prior studies have found no difference in mortality between patients who received thrombolysis through telemedicine compared to those who were managed with on-site stroke specialists; however, these did not account for the relative contributions of the severity of stroke, the underlying health of the patient, or process factors at the site where treatment was provided.7–9
The purpose of this study was to determine whether patients receiving telestroke-assisted IV tPA had similar outcomes to patients who received IV tPA without telestroke. Specifically, we estimated the risk of mortality within 7 and 90 days of telestroke-assisted IV tPA compared to IV tPA provided with on-site stroke expertise. We also compared the risk of symptomatic intracerebral haemorrhage (sICH) complication and poor functional outcome at discharge in these patient groups.
Methods
Study design
This was an observational retrospective cohort study using registry and health administrative data sources.
Study setting
The study took place in the province of Ontario, Canada. Ontario has a population of 13.6 million (2014) distributed unequally over a large landmass. 10 At the time of the study, 38% of telestroke hospitals were located in small towns, defined as outside the commuting zone of centres with a population of 10,000 or more. 11
Ontario’s health system is publicly funded and all residents are eligible for medically necessary services provided by physicians and hospitals.
Data sources
The study cohort was derived from two cross-sectional Ontario Stroke Registry audits of patients with acute stroke and transient ischaemic attack (TIA) who received care in acute care hospitals in Ontario in two fiscal years 2010/2011 and 2012/2013 (April 1 to March 31). Patient records selected for audit were identified from the Discharge Abstract Database (DAD), an administrative data source that includes demographic and clinical information on all patients discharged from acute hospitals in Ontario. Details of the audit methodology have been reported previously but, in brief, trained abstractors performed chart abstraction to collect information about the patient’s presenting symptoms, medical history, diagnostic tests, and treatment.12,13 In the audits, all patients who received care at hospitals offering telestroke were audited with the exception of one telestroke site in the 2012/2013 audit where the annual stroke/TIA caseload was below the audit inclusion threshold.
We restricted the study cohort to cases where the final diagnosis was ischaemic stroke and IV tPA was administered. Patients who had a telestroke consultation at a hospital participating in the telestroke program were included in the telestroke group, while all other patients were included in the non-telestroke group (see Figure 1). Cases where telestroke-assisted IV tPA occurred at a non-telestroke registered site were excluded (n = 4).
Flowchart of study population.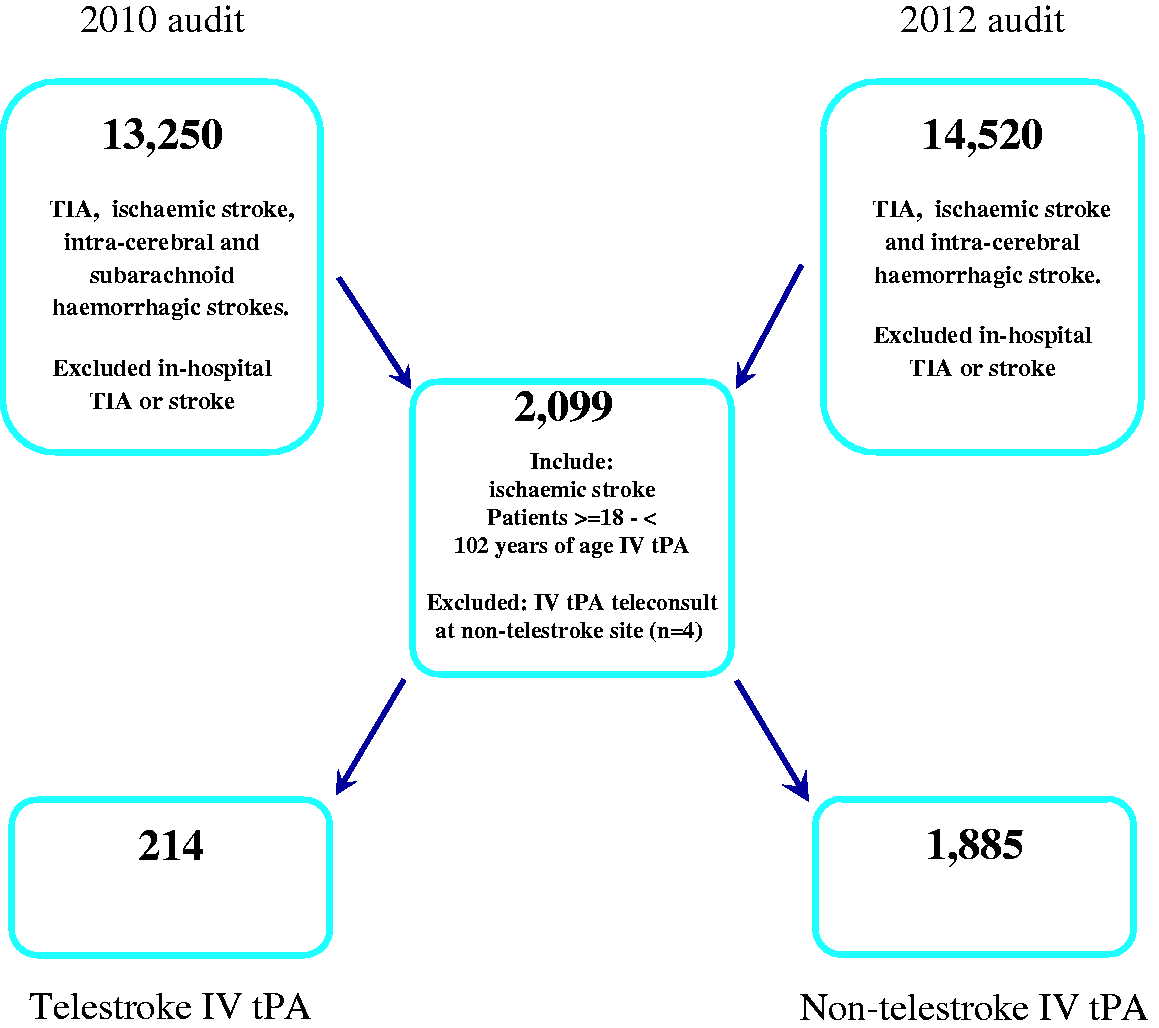
Using the patient’s encrypted health card number, we linked to Ontario’s Registered Persons Database to obtain demographic information and death date. Patient postal code was linked to the Postal Code Conversion File Plus (PCCF+, Statistics Canada) for information on place of residence (rural or urban).
Each patient’s Charlson-Deyo comorbidity score was calculated by linking the audit data to the DAD.14,15 We used a two-year lookback and ICD-10 diagnostic code equivalents to determine whether comorbid conditions were present. 16 Data linkages and analyses were conducted at the Institute for Clinical Evaluative Sciences (ICES).
The audit provided information on patient characteristics including: stroke severity, 17 sICH defined as intracerebral haemorrhage following IV tPA administration with documentation that the patient’s neurological status significantly deteriorated within 36 hours of IV tPA; modified Rankin Scale (mRS) score at discharge summarizing the patient’s functional status, 18 and care on a stroke unit. 13
Ontario Telestroke Program (OTP)
Telestroke represents a partnership between the Ontario Telemedicine Network (OTN), the OSN, and CritiCall. CritiCall manages the emergency telephone referral service while OTN oversees the entire program including the telemedicine infrastructure and the Telestroke Steering Committee. The Steering Committee is co-chaired by a medical director who represents the stroke neurologist consultants and organizes regular telephone conference calls with consultants, as well as dealing with any complaints. CritiCall is the central call centre for paging telestroke consultants while OTN provides the connectivity, manages the consultant call schedule, and does the accounting for the physician stipends. The provincial health ministry funds all aspects of the program including remuneration of the consultants.
All of the telestroke consultants are “stroke neurologists”, implying they have fellowship training in stroke care and have the same qualifications as those within hospitals providing on-site IV tPA consultation. As of 2017, 20 consultants are on the roster, many having participated for more than a decade. Consultants receive an on-call stipend for each 24-hour shift plus fee-for-service for each consultation completed. Following a consultation, a telestroke consultation report template (fillable pdf) is completed by the telestroke neurologist and faxed to the referring hospital where the report is added to the patient’s medical record.
The OTN supports a secure virtual private network (VPN) with connectivity to all Ontario hospitals. Each user requires a name and password to connect to the telestroke VPN. Teleconferencing is managed using VidyoDesktop (www.vidyo.com/video-conference-systems/vidyodesktop), available for desktop and mobile platforms. The application allows for camera control (pan and zoom) at the patient’s bedside. Images are transferred between referring sites and consultant using the Emergency Neuroimaging Transfer System (ENITS) (www.health.gov.on.ca/en/pro/programs/ecfa/action/acute/hsp_enits.aspx). All computed tomography (CT) and magnetic resonance imaging (MRI) scanners in Ontario are connected to the ENITS server and all acute head CTs are automatically pushed to the ENITS server. The digital imaging and communications in medicine (DICOM) browser used to review images is eUnity (www.clientoutlook.com/eunity-platform/diagnostic/) and is available for PC, Mac, iPad, iPhone, and android devices. ENITS requires two-step identification for successful login. All images stay on the ENITS server for two weeks.
Referring sites are asked to page Telestroke (CritiCall) before the CT is completed to allow time for the consultant to logon to their computers and to discuss the patient history. Telestroke consultants are asked to respond within 10 minutes of being paged, otherwise CritiCall will contact the standby consultant.
Ontario’s regionalized stroke care system has three types of hospitals: RSCs are acute hospitals with stroke protocols, clinicians with stroke expertise, access to neurosurgery and interventional neuroradiology, and linkages to rehabilitation and secondary prevention service providers. 13 District Stroke Centres (DSCs) meet the requirements of RSCs but do not have neurosurgery or interventional radiology. Over the period of this study, two RSCs and several of the DSCs used telestroke on an as-needed basis, for example, to cover staff neurologist scheduling gaps. A non-designated centre is an acute hospital that does not meet the definition of either a RSC or DSC.
When a patient arrives at the ED of a telestroke-referring hospital within 4.5 hours of stroke-symptom onset, the ED physician conducts a rapid assessment, the patient is transferred to the CT scanner, and the CritiCall relay process activated. Over telephone, the ED physician and on-call telestroke consultant review the history and findings while the CT scan images are automatically uploaded to a provincial server for the consultant to review. The consultant then connects to the referring hospital’s ED via two-way video-conferencing and performs a virtual physical examination of the patient and makes treatment recommendations including whether IV tPA should be administered. In eligible cases, the consultant may suggest that the patient be transferred to a Regional Stroke Hospital for endovascular or neurosurgical treatment.
Analysis
In the analysis, we excluded patients younger than 18 years or older than 102 years. We calculated standardized differences (SDs) to compare characteristics of patients who received IV tPA with and without telestroke assistance. 19 A difference of less than 0.1 is considered non-significant.
We analysed four outcomes: all-cause death within 7 and 90 days of ED arrival, sICH, and mRS score at discharge. Survival time was calculated as the difference between the date of ED arrival and the date of death. The mRS score was dichotomized as 0–2 (no or minimal disability) versus 3–5 (moderate to severe disability).
We modelled the risk of death within 7 and 90 days using Cox proportional hazards adjusting for year and variables with a p-value of <0.05 in bivariate analysis or known to be associated with poor outcome. Variables included whether IV tPA was telestroke assisted, hospital type, sex, age group (18–64 years, 65–79, ≥80), stroke severity (mild, moderate, severe), stroke unit admission, rural residency, history of atrial fibrillation, and comorbidity score (<2 or ≥2). In a secondary analysis exploring the relationship between telestroke and a hospital’s capacity to provide comprehensive stroke care, we re-ran the model, creating an interaction term of telestroke by hospital type. RSC and DSC hospitals were categorized as “stroke centres” and non-designated hospitals as “non-stroke centres”. We corrected for hospital clustering using the variance sandwich estimator.
We used logistic regression with generalized estimating equations adjusting for hospital clustering and used the same variables as in the mortality model to examine the association between telestroke-assisted IV tPA and sICH and functional outcomes. We used SAS Enterprise Guide, version 6.1, for all analyses (SAS Institute, Cary, NC). The full data set creation plan is available from the authors upon request.
This study was approved by the Research Ethics Board of Sunnybrook Health Sciences Centre, Toronto, Ontario, Canada.
Results
Characteristics of patients who received telestroke-assisted intravenous thrombolysis with tissue plasminogen activator (IV tPA) compared to patients who received IV tPA with on-site expertise, Ontario Stroke Audit 2010/2011 and 2012/2013.
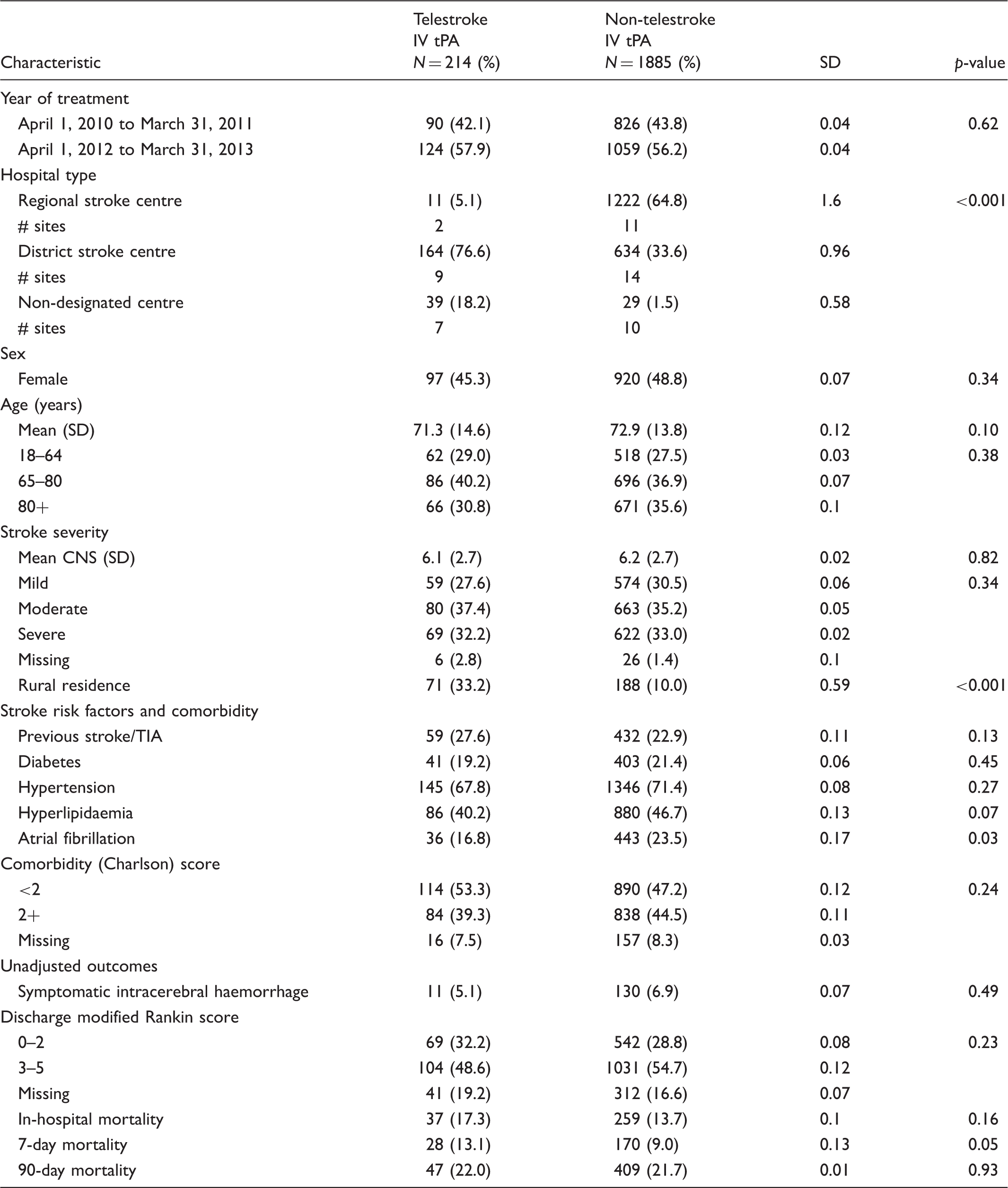
CNS: Canadian Neurological Scale (mild ≥8, moderate 5–7, severe <5); TIA: transient ischaemic attack; SD: standardized difference.
Differences <0.1 considered non-significant.
Process measures between patients receiving intravenous thrombolysis with tissue plasminogen activator (IV tPA) with and without telestroke assistance.
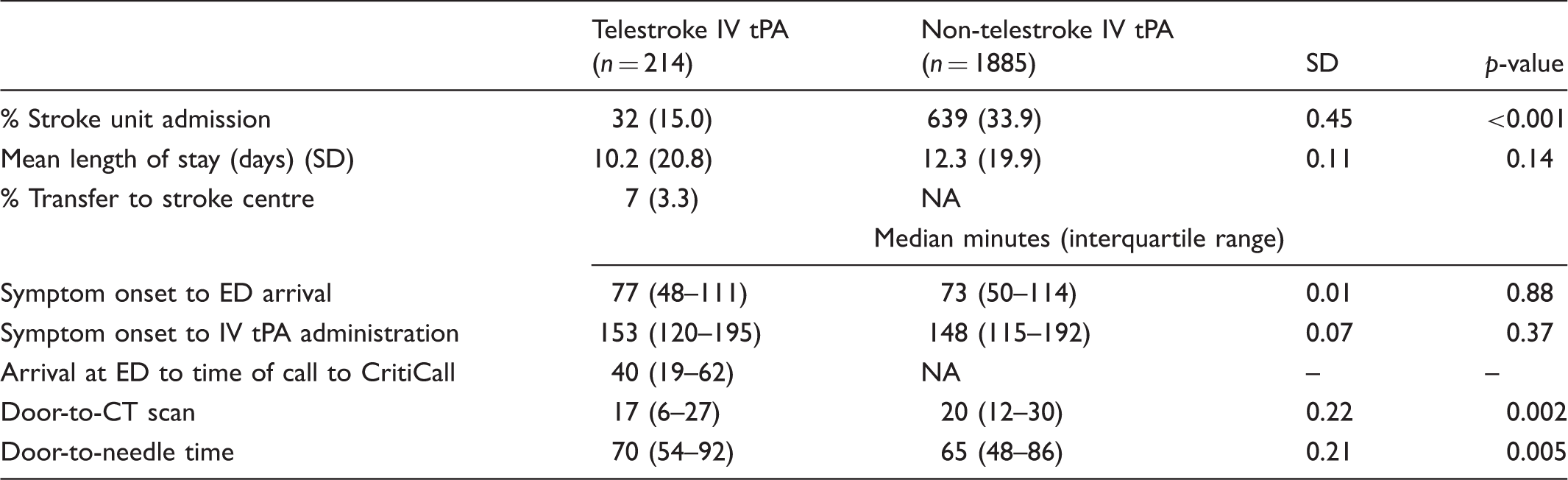
SD: standardized difference; NA: not applicable; ED: emergency department; CT: computed tomography.
Differences <0.1 considered non-significant.
Adjusted hazard ratios (aHR) and odds ratios (aOR) for outcomes following intravenous thrombolysis with tissue plasminogen activator (IV tPA).
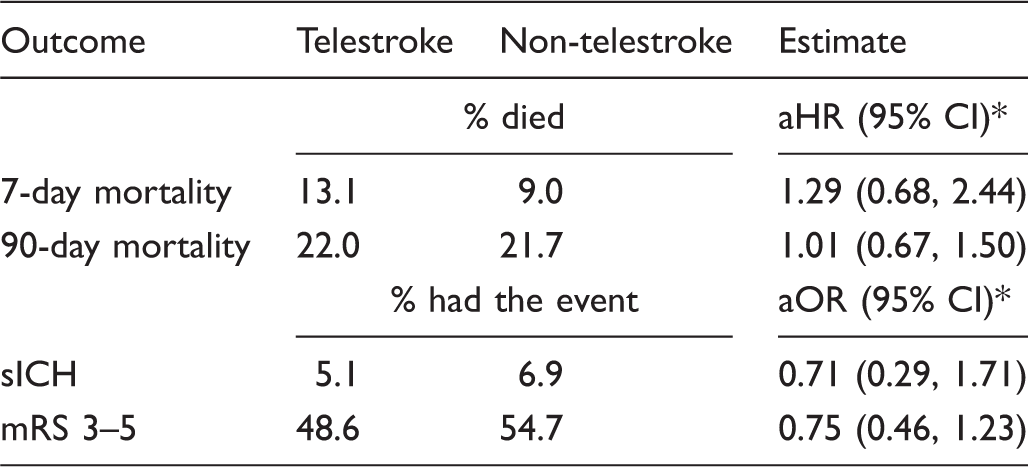
CI: confidence interval; sICH: symptomatic intracerebral haemorrhage; mRS: modified Rankin Scale, where a score of 3–5 indicates moderate to severe disability.
Reference category: telestroke = no.
Adjusted for age group, sex, atrial fibrillation, comorbidity score, stroke severity, hospital type, stroke unit, year, telestroke, rural residence.
Adjusted hazard ratios (aHR) for interaction between telestroke and hospital type, by outcome.
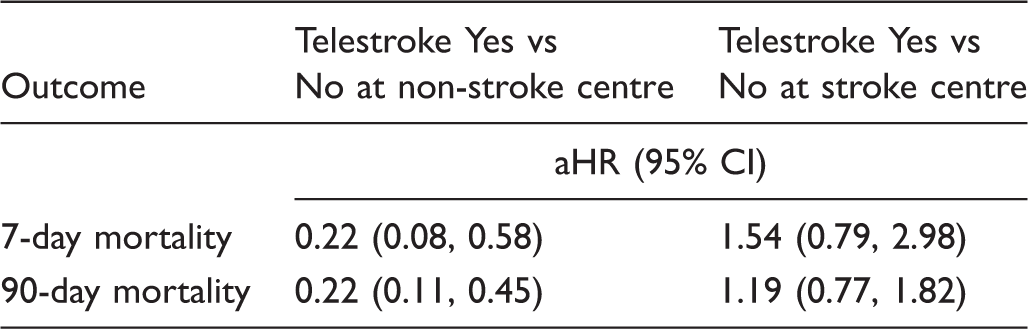
CI: confidence interval.
Adjusted for age group, sex, atrial fibrillation, comorbidity score, stroke severity, hospital type, stroke unit, year, telestroke, rural residence, hospital type.
Discussion
We found that patients with acute ischaemic stroke who received telestroke-assisted IV tPA were not at greater risk of death within 7 or 90 days, nor at greater odds of experiencing sICH or poor functional ability at discharge compared to non-telestroke patients.
The median DTN time among telestroke patients was 70 minutes and is lower than the 90–97 minutes reported in other jurisdictions.9,20,21 Studies have shown that pre-hospital processes are associated with reduced DTN times and, consequently, complications and mortality.22–24 In Ontario’s stroke system, pre-hospital protocols include a paramedic screening tool and ED pre-notification. The time to CT scan, however, was shorter at telestroke sites, suggesting that parsing of both the telestroke program and referring site processes is needed to better understand and improve DTN times.
The rate of sICH (5.1%) among telestroke-assisted IV tPA patients was similar to non-telestroke IV tPA patients (6.9%), and falls within the 0.9% to 10% range reported in previous studies.8,9,20,21,25–28 Two earlier Ontario studies reported sICH rates following IV tPA of 2.0% and 10%.23,29
In this study, 17.3% of telestroke-assisted IV tPA patients died in hospital, while 22% died within 90 days – the latter similar to the rate found in an earlier Canadian study (22.5%). 27 Other studies have reported un-adjusted in-hospital mortality rates following telestroke-assisted IV tPA ranging from 5.4% to 10.9%, and at 90 days, from 8.3% to 14%.8,9,20,25,28,30 In a randomized controlled trial examining the effect of extending the thrombolysis treatment window from 3 to 4.5 hours, 7.7% of Alteplase-treated patients (n = 32) died within 90 days of treatment compared to 8.3% of those who received a placebo. 31 However, our cohort was older and had, on average, a higher degree of comorbidity compared to patients participating in the Alteplase trial.
This study has several limitations. First, our results depend on the accuracy and completeness of medical record abstraction. Abstractors were required to achieve 85% agreement with clinical experts on key data elements in training charts and had access to a stroke specialist throughout the data collection. Although we adjusted for admission to a stroke unit and stroke centre, other processes of care that may influence outcomes including those related to telemedicine technology were not available for analysis. The overall number of cases treated at non-stroke centres was small (n = 68) and while the protective effect of telestroke service appears to be large, the CIs are wide, suggesting further examination with a larger sample is needed. We do not have the measurements of patients’ pre-event functional status to determine the extent or direction of change, limiting comparisons with other studies. Finally, our results are from a mature stroke system within a publicly funded healthcare system and may not be generalizable to other regions and countries.
In this large cohort of IV tPA patients, those who received telestroke-assisted IV tPA had similar outcomes to those managed with on-site expertise. For non–designated stroke centres, telestroke appears to result in better outcomes. These findings support the ongoing use of telestroke services for thrombolysis administration.
Footnotes
Acknowledgements
The opinions, results, and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred.
We acknowledge the help of the OSN in particular, Chris O'Callaghan and Linda Kelloway and the OSN Telestroke Steering committee in creating this document. The OSN provides provincial leadership and planning for the Ontario Stroke System by measuring performance, partnering to achieve best practices, and creating innovations for stroke prevention, care, recovery, and reintegration. As of April 1, 2016, the OSN and Cardiac Care Network of Ontario (CCN) have come together as a single entity to ensure a comprehensive and integrated approach to cardiac, vascular, and stroke care in Ontario.
Parts of this material are based on data and/or information compiled and provided by CIHI. However, the analyses, conclusions, opinions, and statements expressed in the material are those of the authors, and not necessarily those of CIHI.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). Moira Kapral is supported by a Career Investigator Award from the Heart and Stroke Foundation, Ontario Provincial Office.