
Abstract
Introduction
This study examined the effect of a telehealth intervention on the control of type 2 diabetes and subsequent potential cost-savings to the health system.
Methods
This prospective randomised controlled trial randomised adults with type 2 diabetes to the intervention (diabetes program) or control (usual care) arm. Key eligibility criteria included an HbA1c level of at least 58 mmol/mol (7.5%) without severe or unstable comorbidities. All participants continued their usual healthcare, but participants in the intervention arm received additional diabetes care from a diabetes care coordinator via a home monitor that captured clinical measures. Data collected included biomedical, quality of life measures and healthcare (GP, outpatient and inpatient) costs. The primary outcome was HbA1c collected at baseline and 6 months. Analysis was conducted on a complete case intention-to-treat basis. The healthcare system perspective was taken to calculate the incremental cost per percentage-point reduction in HbA1c.
Results
Results from 63 participants from each study arm were analysed. HbA1c in the intervention group decreased from a median 68 mmol/mol (8.4%) to 58 mmol/mol (7.5%), and remained unchanged in the control group at median 65 mmol/mol (8.1%) at the 6-month endpoint. The intervention effect on HbA1c change was statistically significant (p = .004). Total healthcare costs in the intervention group, including the intervention costs, were lower (mean $3781 vs. $4662; p < .001) compared with usual care.
Discussion
There was a clinically meaningful and statistically significant benefit from the telehealth intervention at a lower cost; thus, telehealth was cost-saving and produced greater health benefits compared with usual care.
Introduction
Worldwide, diabetes is recognised as a growing problem that may threaten global development in the future. In Australia, diabetes is the fastest growing chronic disease, and is among the top 10 leading causes of death.1,2 In 2011–2012, 5.1% of Australian adults had diabetes, with 90% having type 2 diabetes. 3 By 2031, it is projected that approximately 10% of the total Australian population may have type 2 diabetes. 3
Since 1997, diabetes has been one of Australia’s National Health Priority Areas due to its significant impact on the health of Australians. 4 Health planners are concerned that the level of chronic and preventable conditions, such as type 2 diabetes, has reached the point where the Australian health system can no longer sustain the level of burden of disease.5,6 Long-term effects of uncontrolled diabetes increase the burden on the health system, with poor glycaemic control significantly increasing the risk of complications such as neuropathy, retinopathy, nephropathy, myocardial infarction, stroke and amputations. 7
Systematic reviews of telehealth (including telemonitoring) interventions for type 2 diabetes consistently show positive effects on glycaemic control, with variation in effects on other diabetes risk factors such as blood pressure, lipids and weight/body mass index.8–14 Additionally, people’s quality of life and satisfaction with care appear to improve as a result of telemonitoring interventions.10–13
Large-scale programs have shown that the use of telehealth technologies combined with a care coordination model of care can be effective in helping people manage their chronic health condition. A US study of over 17,000 people enrolled on a home telehealth program reported after 6 months of participation a 20% reduction in hospital admissions and 25% reduction in bed days of care over 1 year compared with admissions pre-enrolment. 15 People with diabetes in a US Veterans Home Telehealth project had a reduction in the overall use of inpatient and outpatient services over the 48-month follow-up period. 16
The financial benefits from use of telehealth and e-health services are estimated to accrue from reduced use of secondary healthcare services, with Access Economics estimating the financial benefits of wide-scale telehealth implementation as being between $2 billion and $4 billion per year in Australia. 17 A recent Australian study examining telemonitoring for people with a range of chronic diseases (including diabetes) who were frequently admitted to hospital concluded that the return on investment of telemonitoring would be between 4.9 and 6.0, resulting from less utilisation of hospital and other health services. 18 An Australian telehealth randomised controlled trial (using an automated interactive telephone intervention in type 2 diabetes) showed substantially lower healthcare costs modelled over 5 years. 19 Reviews highlight the need for more evidence on the economic impact of telemonitoring for diabetes.10,13,20,21
To the knowledge of the authors, no randomised controlled trials testing the use of telemonitoring in the management of type 2 diabetes in Australia have been conducted. The present study is designed to give high-quality evidence on the use, including the economic impact, of this health service in Australian primary care, as well as contributing to international knowledge.
We hypothesised that a tailored telemonitoring intervention could result in better control of diabetes and reduced utilisation of health services. The study, named the Townsville Broadband Diabetes Telehealth (TBDT) trial, examined the effect of a telemonitoring intervention based in primary care on the control of type 2 diabetes at 12 months following the intervention, and subsequent cost-savings to the health system.
Methods
Study design
The study was a two-arm prospective randomised controlled trial in which adults with type 2 diabetes were randomised to the intervention (diabetes program) or control (usual care) arm, and was conducted in a primary health setting in a regional city in Queensland, Australia. The study was conducted with the cooperation of 25 general practices, which were the usual practices participants attended for their diabetes care.
Participants
Inclusion and exclusion criteria.

Randomisation and masking
Arm allocation was conducted with the participant as the unit of randomisation, using computer-generated 1:1 simple randomisation. The random allocation sequence was generated by the study research coordinator (KC), held in a secure opaque envelope by the study administrator and concealed from the study Care Co-ordinators (CCs). CCs consented participants and contacted the study administrator for group assignment. Due to the nature of the intervention, participants, health professionals and researchers were not blinded to trial arm allocation.
Procedures
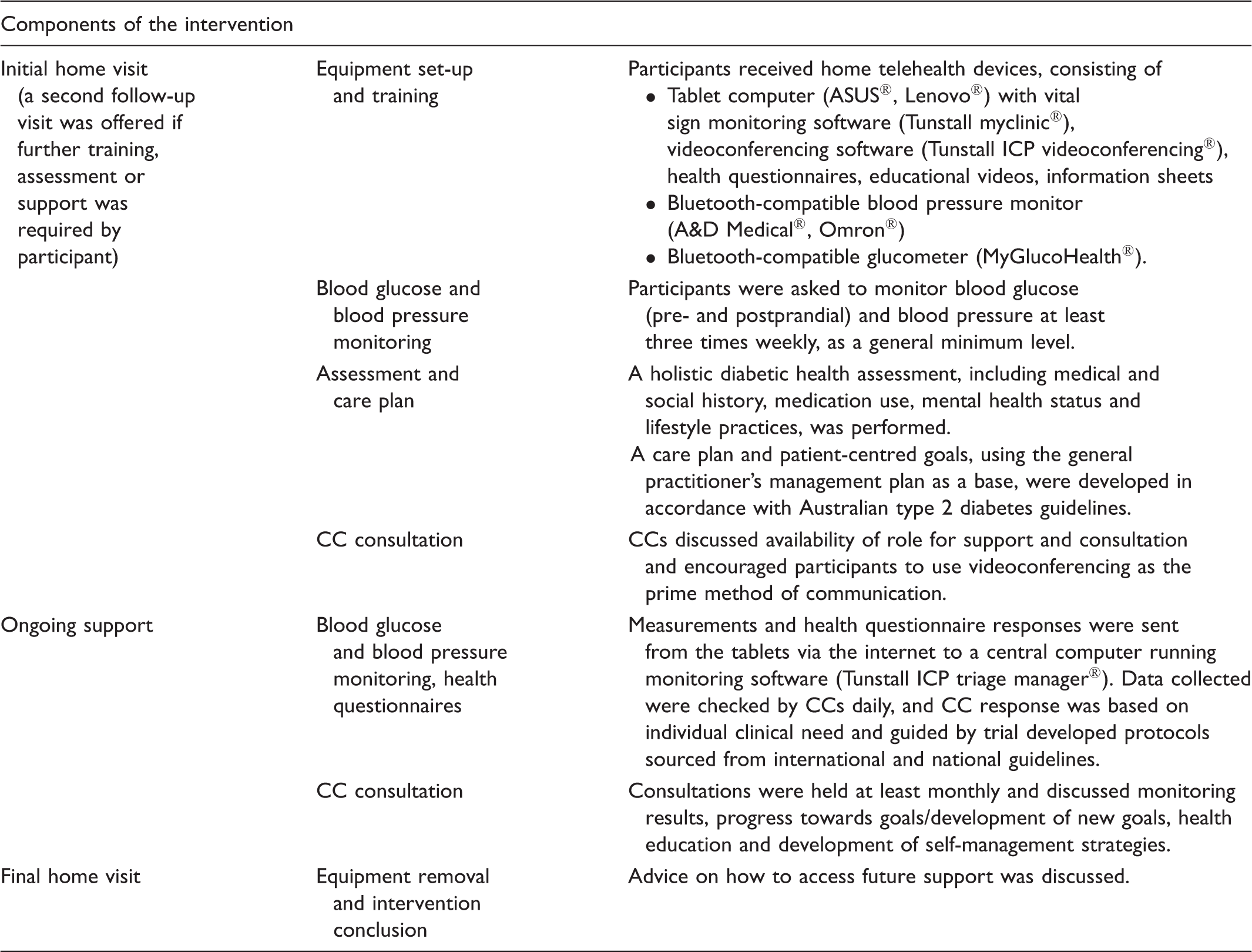
Trial intervention.
Outcomes
The primary clinical outcome was HbA1c expressed as %; secondary clinical outcomes were a range of biomedical measures (blood pressure and test results, etc.) including depression, frequency of health services use (e.g. GP consultations, specialist visits, admissions to hospital) and costs. Participant satisfaction and technology acceptability measures were also collected, and results of these outcomes will be reported in a future paper. Participant data were collected by GPs and CCs at baseline and follow-up. On study completion, data were collected from GPs and public hospital records on deaths, details of hospital admissions, referrals to medical specialists, and number of visits to the GP. Participants were surveyed at baseline and follow-up using a quality of life questionnaire (12-Item Short Form Survey (SF-12)) and a depression screening questionnaire (Kessler Psychological Distress Scale (K10)).23,24 The research team collected data on trial set-up and operational and intervention costs. For the purposes of calculating adherence and intervention costs, frequency and length of participant/CC use of the telemonitoring equipment were captured automatically by the monitoring system. Participation in intervention aspects not recorded by the monitoring system (e.g. telephone calls, home visits) was registered by CCs in the system’s participant records. Copies of participant records were extracted monthly for review of accuracy by the CCs. Detailed timesheets of workflow for CCs were maintained for fortnightly periods at three time points in the study period to calculate staff costs.
Safety concerns and adverse events were monitored through a CC weekly clinical review. Any suspected concerns were reported to the participants’ GPs. Additionally, the study’s Clinical Advisory Group met regularly to confirm the clinical conduct of the intervention and respond to clinical issues and safety.
Statistical analysis
Initial power calculations showed that assuming an attrition rate of 30% over 12 months, an intervention effect of at least a 5 mmol/mol (0.4%) reduction in HbA1c would be able to be detected with 80% power and type I error of 5% (two-tailed) from complete data on 210 participants.25,26 During the course of the trial, significant delays in the roll-out of high-speed internet connections affected recruitment strategies and progress of the trial. To ensure completion of the study within timeframes required by funders, the target was adjusted to ensure 6 months’ follow-up from all participants, as previous evidence had shown that positive effects could be expected in this time. The sample size target was decreased to 120 participants, based on evidence that a larger effect could be expected. 27 Enrolment in the study closed when this sample size was achieved.
Analyses were conducted on a complete case intention to treat basis.
Missing values of HbA1c at 6 months were replaced with the 3 months’ observations (last observation carried forward). Missing cost outcomes for participants who were lost or withdrew after randomisation were not imputed. Analysis of covariance (ANCOVA) models were fitted to investigate the effect of study arm on the outcome measures. Possible confounding by baseline characteristics was also explored. Residual, DFBETA and Cook’s distance graphs were checked. Sensitivity analyses were performed with influential observations excluded from analysis. Differences in secondary clinical outcomes between groups were explored using ANCOVA models or logistic regression. Stata 13.1 was used for statistical analysis. To be considered as statistical significance, p-values at <.05 were used.
Economic analysis
Cost-effectiveness was assessed from a healthcare system perspective using participant-level data from the trial. The cost of healthcare utilisation was calculated for the trial period by summing the cost of visits to GPs, specialists and hospital admissions. Hospital events were categorised as diabetes-associated or all other-cause events. Length of stay data, where missing, was replaced with the mean length of stay for that diagnosis-related group (DRG) item. The costs of private hospital admissions were replaced with the mean cost of the DRG item considering the observed length of stays. The average daily cost of the intervention per participant was calculated; this included recruitment, set-up, health assessments, CC consultations, monitoring and triage, software maintenance, internet connection, reports and communication with other health professionals, and equipment removal. An alternative daily cost value was calculated assuming a fully implemented service and used for sensitivity analyses. All costs were converted to 2013 dollars using the Australian Consumer Price Index. Costs were compared between groups using the non-parametric median test. The incremental cost-effectiveness ratio (ICER) was calculated as the difference in costs divided by the difference in mean HbA1c results for the two strategies. The 95% credible interval for the ICER was estimated by bootstrapping the results with 1000 simulations. Sensitivity analyses were undertaken for key parameters with uncertainty and/or variability.
Ethical approval for the trial was received from the Royal Australian College of General Practitioners National Research and Evaluation Ethics Committee (11-006) and the Griffith University Human Research Ethics Committee (MED/07/12/HREC). The trial protocol was published in 2012. 25 The trial was registered with the Australian New Zealand Clinical Trials Registry (ACTRN12612000086864).
Results
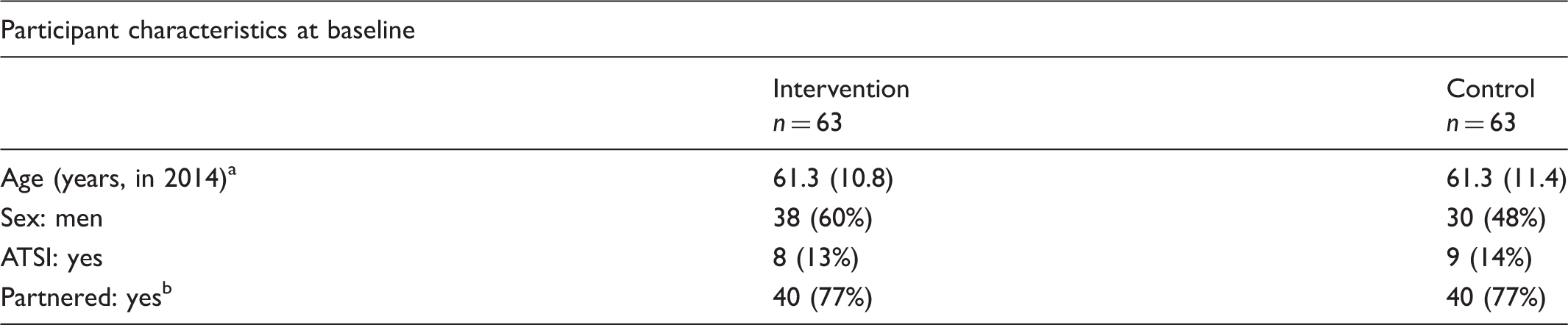
Recruitment was conducted from 1 February 2012 to 20 June 2014. A total of 157 individuals were randomised. Of these, 31 participants were lost to follow-up, of whom 19 were unable to participate in the study (Figure 1). This was primarily due to a long time interval between consent and intervention commencement forced by the availability of internet connections, and resultant changes in participant circumstances (e.g. medical status, residential address) for 17 participants allocated to the intervention. Follow-up data were collected and analysed from 126 participants (Figure 1). Participant characteristics at baseline are presented in Table 3. Participants in the two arms were similar in age distribution and indigenous and marital status, but there were slightly more men in the intervention group compared with the control group (38/63 vs. 30/63, respectively).
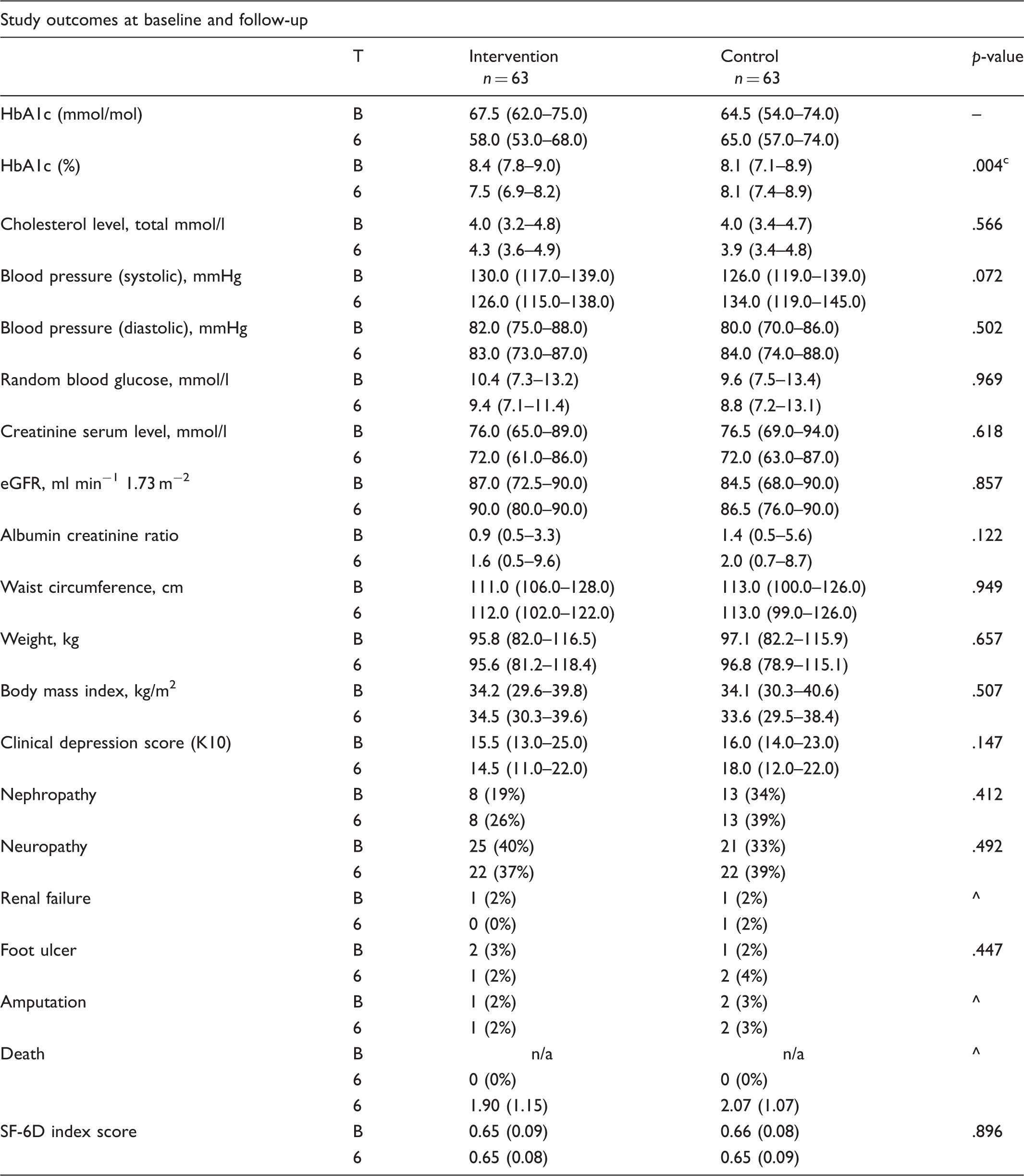
Participant flow. Participant characteristics and study outcomes. Frequencies and column percentages shown unless otherwise noted. Mean (standard deviation) shown. Responses to this question were received from 104 participants. ATSI: Aboriginal or Torres Strait Islander. Frequencies and column percentages shown unless otherwise noted. Mean (standard deviation) shown. Responses to this question were received from 104 participants. ATSI: Aboriginal or Torres Strait Islander. n (%) or median and inter-quartile range presented unless otherwise noted; frequencies may not add up to group size due to missing data; % proportions calculated with number of non-missing values in denominator. p-values (null hypothesis: no difference in observed changes between groups) calculated with analysis of covariance or logistic regression. adjusted for body-mass index at baseline. 6: 6 months’ follow-up; B: baseline; eGFR: estimated glomerular filtration rate; HbA1c: glycated haemoglobin; K10: Kessler psychological distress scale; Nephropathy: albumin/creatinine ratio ≥ 2.5 males, ≥ 3.5 females; Neuropathy: any loss of foot sensation on 10-point microfilament test; Renal failure: presence of chronic kidney disease Stage 4 or 5, as indicated by eGFR<30 ml/min/1.73 m2; T: timepoint; ^: cannot be calculated; n/a: not applicable; –: not calculated.
Participants were engaged in the study over the period from March 2012 to November 2014, and followed for a median duration of 6.9 months (range: 4.4 to 14.4). Intervention participants nominated 51 GPs from 19 general practices as their usual GP, while control participants identified 41 GPs from 20 practices. Three-quarters (75%; n = 47) of participants in the intervention arm engaged in the monitoring aspect of the intervention at levels recommended by the CCs or above, while 62% (n = 39) engaged in the CC consultation aspect of the program at or over the minimum recommended level.
Baseline and follow-up levels of the clinical and quality of life outcomes are presented in Table 3. Baseline values were at similar levels in the study groups, except that the median values of albumin creatinine ratio and nephropathy were approximately 35% lower in the intervention group at baseline. The change in clinical and quality of life outcomes over time was mostly similar across the study groups, except that the change (reduction) in HbA1c values in the intervention group over time was significantly greater than in the control group (p < .01): median difference 9.5 mmol/mol (Table 3), mean difference 8.0 mmol/mol (calculated). For the cost-effectiveness calculation, the difference in HbA1c (%) values between study groups was expressed as the difference in mean values at follow-up: −0.305 (calculated). Post-hoc assessment of the results for the intervention group (two samples of n = 63, repeated measures, ANCOVA analysis) estimated the power at 82%.
The changes in secondary outcome measures (biomedical, depression and quality of life) were neither clinically nor statistically significant (Table 3). There were no adverse events or deaths during the study period.
Cost and effectiveness outcomes.
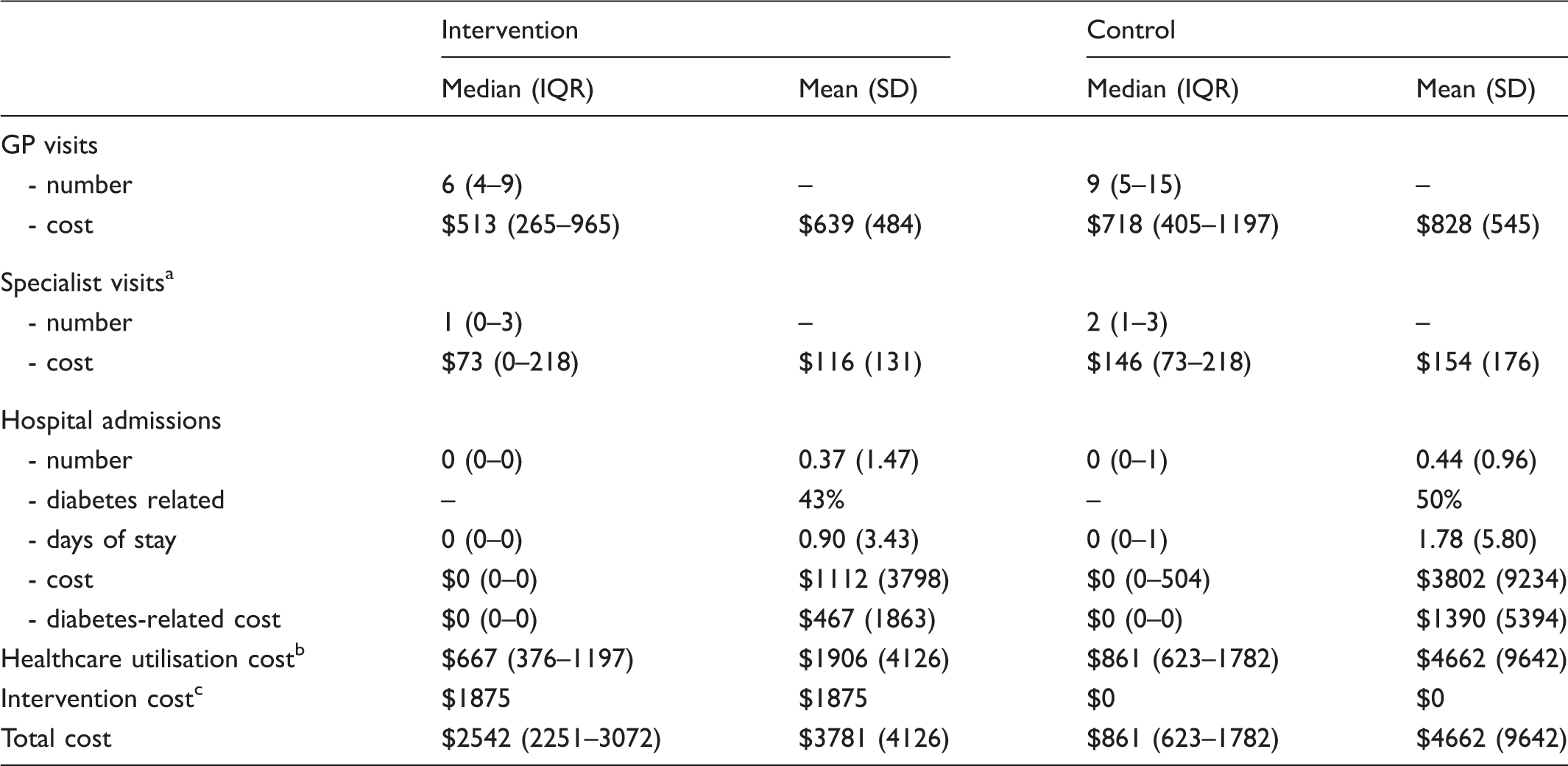
Costs reported in 2013 Australian dollars.
Based on referrals during trial.
Excluding intervention costs.
Same for every participant, therefore spread of values (IQR or SD) is not shown.
GP: general practice; IQR: inter-quartile range as 25th–75th percentiles; SD: standard deviation.
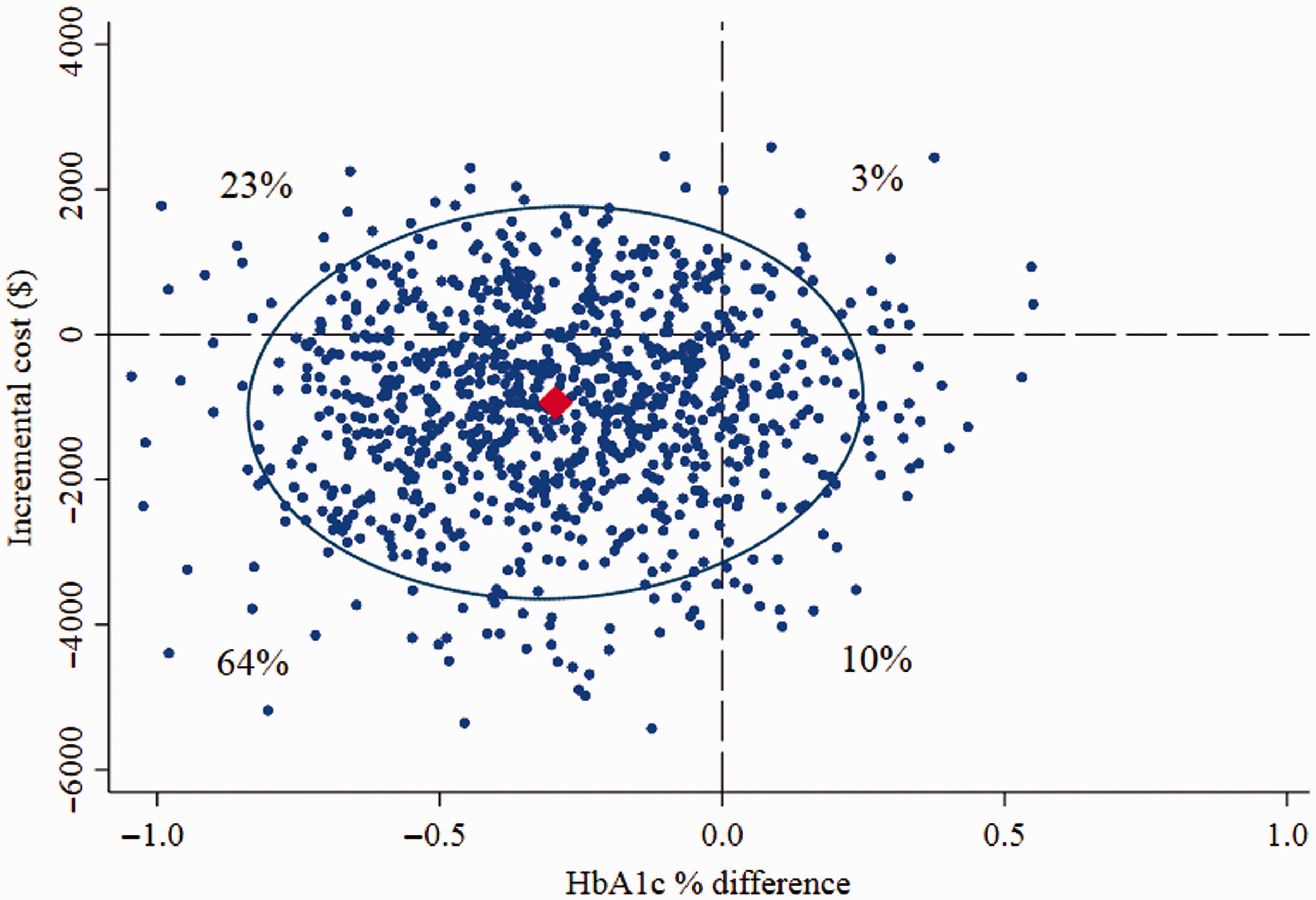
Cost-effectiveness scatterplot.
Cost-effectiveness sensitivity analyses.

ICER: incremental cost-effectiveness ratio, calculated as cost-difference (over 6 months, intervention minus control) between groups divided by the effectiveness-difference (HbA1c % at 6 months, intervention minus control).
Discussion
The TBDT trial showed that a positive effect on glycaemic control resulted from participation in a telemonitoring intervention when compared with usual care. Additionally, this was accompanied by a decrease in the healthcare costs from GP visits, specialist referrals and hospital admissions. There was no significant association found between changes in secondary outcomes and study group.
The reduction of mean HbA1c in the intervention group over 6 months by 8 mmol/mol is comparable to other therapeutic interventions. It is also considered clinically significant, as research from the United Kingdom Prospective Diabetes Study showed that there is a direct relationship between glycaemic level and risk of complications; for example, a 1% lower mean HbA1c was associated with a 21% reduction in deaths related to diabetes, a 14% reduction in myocardial infarction and a 37% reduction in microvascular complications. 7
Healthcare costs were significantly lower in the intervention group (mean difference: $4662–$1906 = $2756; Table 4) compared with the control group. This result excluded the cost of intervention ($1875) applicable in the intervention group; after accounting for this cost, the intervention is clearly cost-saving (net mean cost-savings of $881 (4662–3781; Table 4) per participant in a 6-month period). Efficiency gains (expected after implementation as standard practice) are likely to further decrease the cost of intervention. It is of note that a small number of control group participants incurred relatively high costs (n = 8 had costs >$10,000, max $47,500), but many had zero or low costs, whereas in the intervention group, all incurred the minimum cost of the intervention ($1875) but n = 5 incurred costs >$10,000 (max $23,000). These distributions of costs explain the differences between mean and median costs in the groups. The set-up costs of a telemonitoring system, which are additional to the costs used in the analysis, would impact on the feasibility of providing the intervention initially. However, by providing the intervention at scale and on an ongoing basis, the cost of provision would be offset by the reduction in healthcare resource utilisation costs.
The trial’s results are consistent with previous published telehealth interventions. A recent review of interventions most similar to the present study 13 (telemonitoring for adults with type 2 diabetes) concluded that 15 out of 19 studies reviewed showed positive impacts on HbA1c. The lack of effect on secondary clinical outcomes is similarly consistent, with trials reporting mixed effects on these indicators.10,13 Quality of life did not show significant change in our study, with trials overall showing no change or positive effects on this indicator. 11
The results, in respect to health system use and cost, add to the current evidence in Australia of benefit from the implementation of home telemonitoring. A national multi-site trial in older people with chronic disease also found reductions in hospital and primary care costs. 18 This trial involved participants who were at higher risk of hospital readmission (assessed on their rate of previous admission). Of interest comparatively, our trial was able to demonstrate cost-effectiveness in a group of people of younger average age, selected on the basis of disease (glycaemic) control rather than risk of hospitalisation. Internationally, the reduction of inpatient and outpatient costs has previously been reported as a result of a large-scale home telehealth study.15,16
Limitations of the present study included the reliance on data from 6 months of participant follow-up, compared with the planned 12-month study period, and the failure to reach initial target participant numbers. Nevertheless, post-hoc power analyses showed that the study sample size was adequately powered for the variance around the effect size with a power of 82%. Additionally, data were sourced from general practices, which may have compromised the quality of information relating to healthcare outside of the general practice setting, particularly in outpatient and private hospital admissions; however, this is typical of the population living with diabetes, as patients are generally managed on a day-to-day basis by their GP in primary care. Potential selection bias may have been present in this trial due to factors including the likelihood that people willing to enrol and participate were possibly more likely to show behaviours that increased their wellbeing; additionally, general practices were involved in presentation of the study to potential participants and may have selected patients for their perceived suitability. However, these participants are likely to have been randomly and equally assigned across both groups.
Overall, the study collected comprehensive healthcare utilisation information and cost data from the primary and secondary care sectors to undertake a comparative effectiveness analysis. The intervention was effective in reducing HbA1c levels, shifting patients with diabetes from being poorly controlled to having good control, and significantly reducing the costs of inpatient and outpatient resources.
These results provide evidence of the applicability of telemonitoring to Australian settings, which may be expanded to primary care settings in other jurisdictions. Ideally, the intervention would be suitable to be tested with a larger sample and assessed for its impact across the spectrum of diabetes severity. Additionally, the durability of the intervention’s effect should be studied to predict the possible long-term impact, as well as investigating the most efficient methods for implementation, in terms of cost, effectiveness and integration into current health systems.
Footnotes
Acknowledgements
This work was undertaken by Northern Australia Primary Health Ltd. (formerly trading as Townsville-Mackay Medicare Local), as the organisation responsible for trial implementation, delivery, data collection and reporting.
The authors would like to acknowledge the contributions of the trial team in study development, delivery and data collection: Julie Randall, Julie Twomey, Kathleen Shaw-Farrell, Grant Stephens and Kristen Granata.
Contributors
RW and PS contributed to the study design. RW was responsible for study oversight and delivery. KC and RW collected the data, with KC responsible for management of the trial dataset. PS and GM undertook the statistical and economic analysis. All authors contributed to interpretation, draft and final versions of the report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Townsville Broadband-Enabled Diabetes Telehealth Trial was supported by funding from the Australian Government under the Digital Regions Initiative Partnership Agreement, and the Queensland Government. The Trial Extension was funded by the Australian Government as represented by the Department of Communications.