
Abstract
As the older adult population group has been increasing in size, there has been evidence of growing social isolation and loneliness in their lives. The increased use of information communication technology and Internet-supported interventions has stimulated an interest in the benefits of e-Interventions for older people and specifically in having a role in increasing social networks and decreasing loneliness. A systematic review of e-Interventions to reduce loneliness in older people was conducted with the aim to synthesize high quality evidence on the effectiveness of e-Interventions to decrease social isolation/loneliness for older people living in community/residential care. A systematic search of 12 databases for reviews published between 2000–2017 was conducted using search term synonyms for older people, social isolation and interventions. Three independent researchers screened articles and two reviewers extracted data. The Revised-Assessment of Multiple Systematic Reviews was used to assess the quality of reviews. The final search identified 12 reviews, which included 22 unique primary research studies evaluating e-Interventions for social isolation or loneliness. The reviews were of moderate quality and the primary studies showed a lack of rigor. Loneliness was most frequently measured using the University California Los Angeles Loneliness Scale. Despite the limitations of the reviewed studies, there is inconsistent and weak evidence on using e-Interventions for loneliness in older people.
Introduction
Globally, older persons are a rapidly growing population group. 1 This growth has been accompanied by evidence of increased social isolation and loneliness, especially in older people living in residential care. 2 – 4 Social isolation and loneliness are often used interchangeably, with loneliness referring to the subjective feeling of being lonely, and social isolation referring to the objective paucity of social networks. 5
There has been an exponential growth in the use of information communication technology and Internet-supported interventions 6 in health. Research has shown evidence of improved access, delivery and management of healthcare 7 including social healthcare. 8 These interventions could offer the elderly access to increased communication pathways that can provide for social connectedness. 9 Considering age-specific requirements for adoption of technology,10,11 some evidence is emerging of behavioural intentions to use technology, 9 presenting possibilities of therapeutic use. 12 Several systematic reviews have been published on the effectiveness of information communication technology and Internet-supported interventions for social isolation and loneliness, but the quality of these reviews, and the scope and heterogeneity and rigor of the primary studies included therein, are not known. To address this gap, a review question was developed: What is the level of evidence on the effectiveness of e-Interventions to reduce social isolation and loneliness in older people living in community/residential care? In this review, e-Interventions were defined as interventions that are delivered via Internet-supported, 6 information communication technology (ICT) or other electronic technologies, with or without human support. 13
Methods
An initial search identified several systematic reviews (SRs) of interventions for social isolation/loneliness. Though some reviews were found prior to 2000, these were either non-systematic or qualitative reviews. 14 A protocol for a systematic review to address the review question was approved by the university’s Ethics Committee. Three independent reviewers, screened, selected the data and two reviewers extracted data during the review process. Kappa levels of agreement were calculated and disagreements were resolved through consensus and discussion.
The review was conducted in seven stages. See the Supplementary Material for details of search terms and criteria used.
Stage 1: A systematic comprehensive search was conducted in March 2017, using12 databases (Academic Search Complete, Centre for Reviews and Dissemination searching in the Database of Abstracts of Reviews of Effects (DARE), Health Technology and Assessment (HTA) database, Academic Search Complete, Cochrane Database of Systematic Reviews (CDSR), Cumulative Index of Nursing and Allied Health Literature (CINAHL), Joanna Briggs Institute (JBI), PubMed, Prospero, PsycINFO, Psych Articles, Sabinet, Science Direct and Scopus). The following search terms were used: (‘reviews’ and ‘2000–2017’ and synonyms for ‘cognitively intact older people’, ‘social isolation and loneliness’ and ‘interventions’). In addition, reference lists were scrutinized for additional reviews. Stage 2: Relevant reviews were selected by screening the abstracts of publications found in Stage 1 using the Participants Interventions (Comparison) Outcome Study [PI(C)OS] inclusion and exclusion criteria (Table 1). Stage 3: The selected reviews were assessed for quality using the Revised-Assessment of Multiple Systematic Reviews (R-AMSTAR) quality rating tool for systematic reviews.
15
The 11-item R-AMSTAR allows for quantifiable assessment of systematic reviews providing a measurement of the methodological quality as required for conclusions about clinical evidence with a possible score of 44.
15
A criterion cut-off point, reviews with scores<22 (an average of two marks per criteria which indicates that, on average, only two criteria for each of the domains were satisfied) was used to exclude reviews viewed a low quality.15,16 Stage 4: Data from the selected reviews were extracted and the list of underlying primary studies was entered into Microsoft Excel. Stage 5: The abstracts of the primary studies were reviewed using the PI(C)OS inclusion and exclusion criteria and assessment of study design criteria based on the Centre for Evidence-Based Medicine (CEBM) levels of evidence (LoEs) and grades or recommendations.
17
The CEBM guidelines for study quality are: I: SR, II: randomized controlled trial (RCT), III-1: quasi-experimental studies (QE), III-2: cross sectional studies, and III-3: two group comparative surveys. All studies rated <III (case series, post-test or pre-test/post-test or surveys only) were excluded as comparison designs are inadequate to establish causation due to design problems, bias and confounders which can lead to erroneous conclusions.18,19 Stage 6: A final list of included primary studies was selected and a table of studies per review was compiled to identify the individual unique studies across the reviews. The list of primary unique studies was then classified using an adapted Internet-supported interventions classification,
6
comprised of three categories of e-Interventions, namely: (a) online activities (e.g. social media, computer/Internet use and training); (b) interpersonal communication (e.g. videoconferencing (VC) and Internet-based communication); (c) Internet-operated therapeutic software (e.g. robotics and gaming). Stage 7: Data were extracted and synthesised from the review to address the review objectives. Inclusion and exclusion criteria Participants Interventions (Comparison) Outcome Study [PI(C)OS].

Results
Search and selection
The initial search identified 719 publications. After exclusion of duplicates and irrelevant publications, 160 publications remained. The 160 publications were screened by three reviewers using the PI(C)OS criteria (Table 1). Twenty-six full text reviews were assessed for eligibility, resulting in 12 reviews which included primary studies with e-Interventions. An additional review
20
was identified at this stage and added, resulting in 13 reviews for quality assessment. One review
21
was subsequently excluded (R-AMSTAR = 19) due to a lack of a priori systematic review processes (Figure 1). The levels of agreement between reviewers were good (Kappa = 0.93) and disagreements was resolved through consensus discussion.
PRISMA flow diagram search process. R-AMSTAR: Revised-Assessment of Multiple Systematic Reviews. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.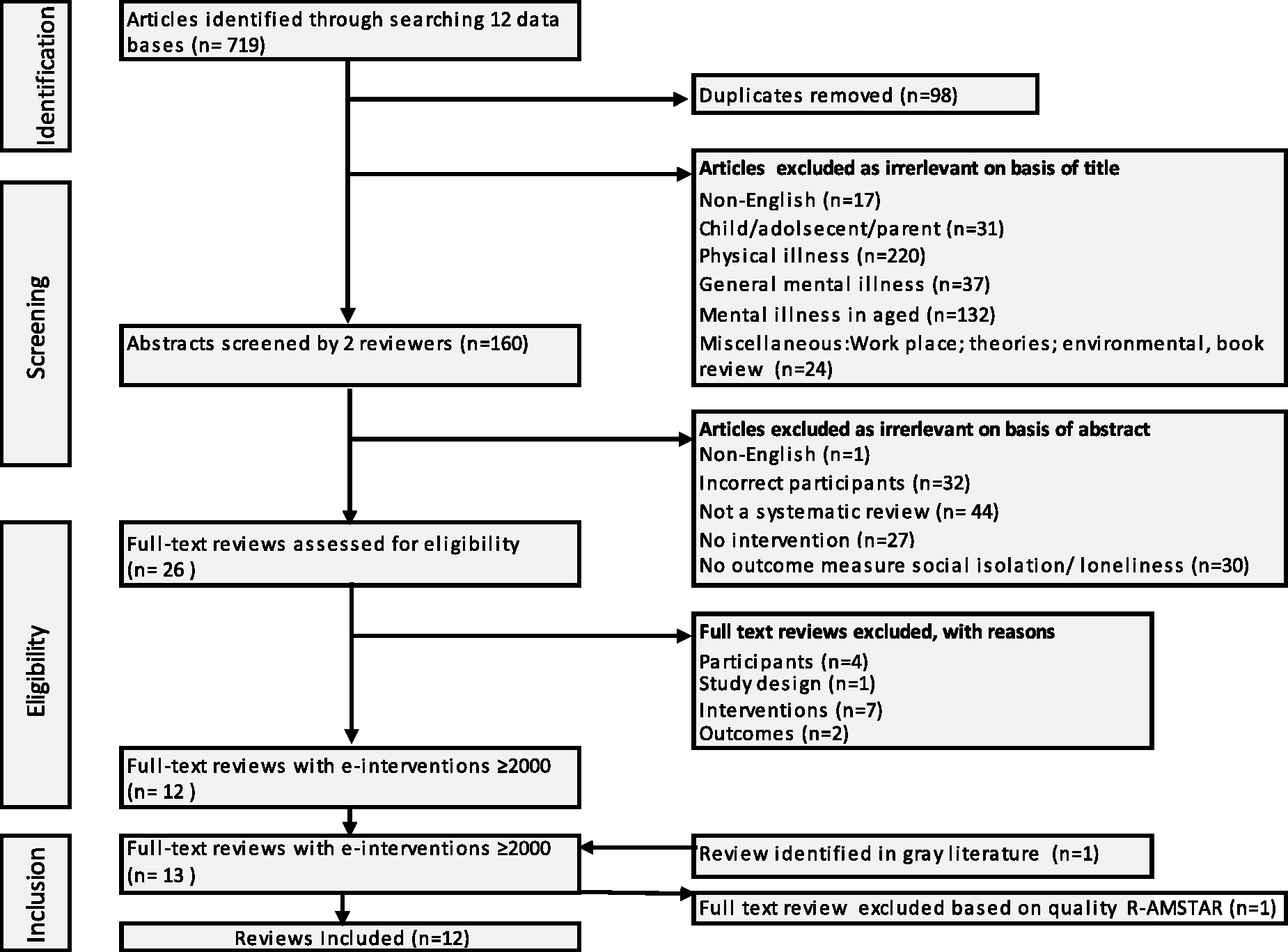
Characteristics of 12 selected reviews
Eight systematic reviews without meta-analysis, 22 – 29 three meta-analyses14,20,30 and one integrative review 31 were included. Five reviews were published in 2016.23,26–28,31 Four reviews focused on e-Interventions targeting social isolation/loneliness in older people,20,23,28,30 two27,29 on e-Interventions for older people (i.e. not limited to social isolation/loneliness), and six on interventions for social isolation/loneliness in older people (i.e. not limited to ICTs).14,22,24–26,31
Quality of 12 selected reviews
Characteristics of the 12 reviews with 22 e-Intervention studies.
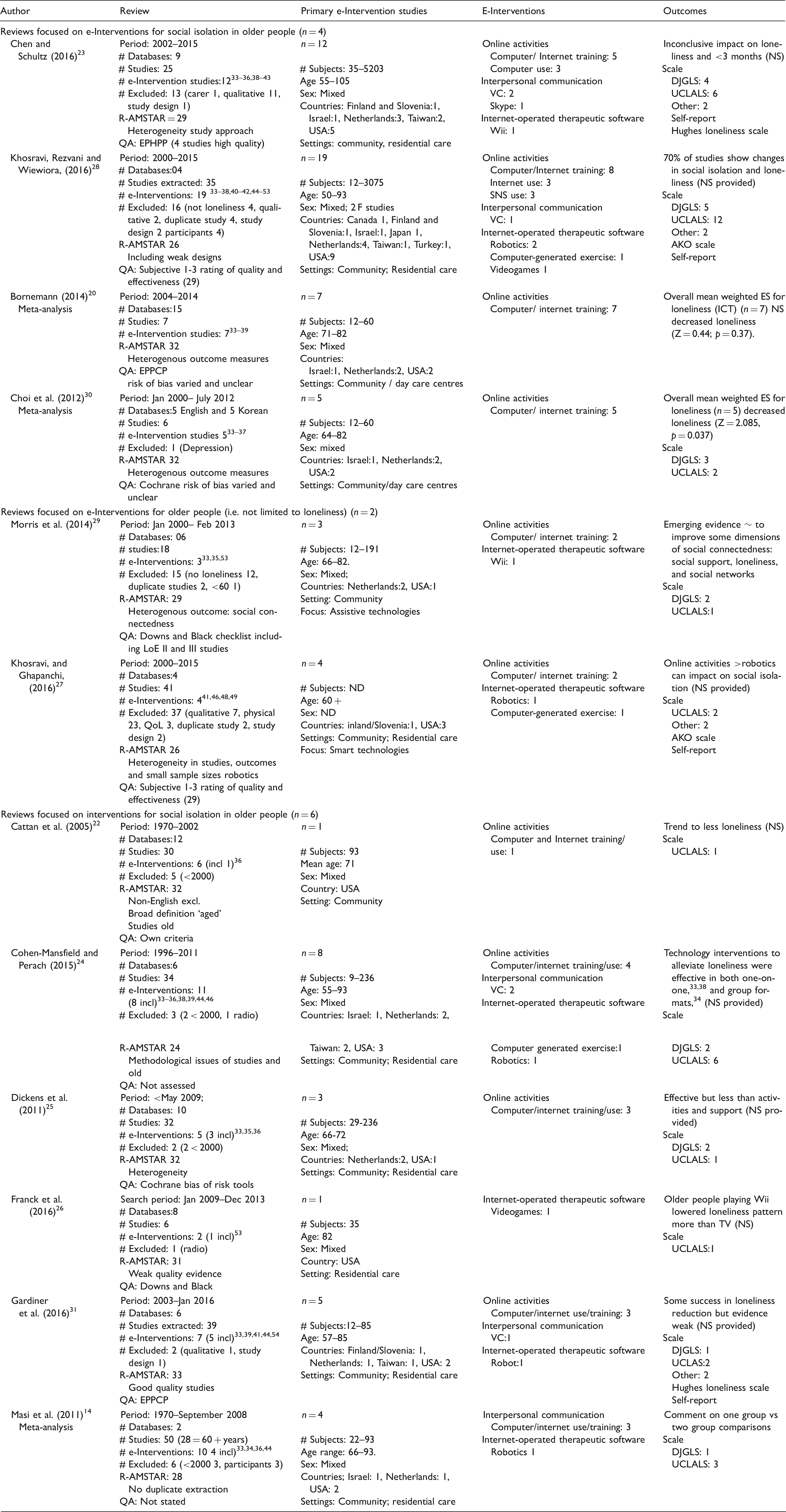
DJGLS: de Jong Gierveld Loneliness Scale; EPHPP: Effective Public Health Practice Project tool; ND: not documented; NS: not significant; QA: quality assessment; UCLALS: University California Los Angeles loneliness scale; VC: videoconferencing.
Primary studies in reviews
The 12 reviews included 323 primary studies of interventions for social isolation/loneliness of which 174 were e-Intervention studies. Using the CEBM criteria of quality (I–III), 72 studies in the 12 reviews were selected for inclusion in this review, resulting in 22 unique e-Interventions primary studies.
More than half (12) of the 22 e-Interventions were conducted in the USA, followed by four in the Netherlands. The studies included cognitively intact older adults living in the community residential settings, though 12 studies were conducted in nursing homes. The most common e-Intervention reported was ‘online activities’ such as computer/Internet training and usage (n = 15). In terms of study design, six of the primary studies were RCTs, eight were QE studies and eight were cross-sectional studies. Outcomes for loneliness were measured using different versions of the University California Los Angeles Loneliness Scale (UCLALS) with the European studies tending to select versions of the de Jong Gierveld Loneliness Scale (DJGLS). Even though critiques have been levelled at the UCLALS for yielding greater effect sizes 14 and being insensitive to change, 21 it was the most frequently used measure for loneliness.
Impact of studies on social isolation
Social isolation/loneliness outcomes for e-Intervention studies (n = 22).
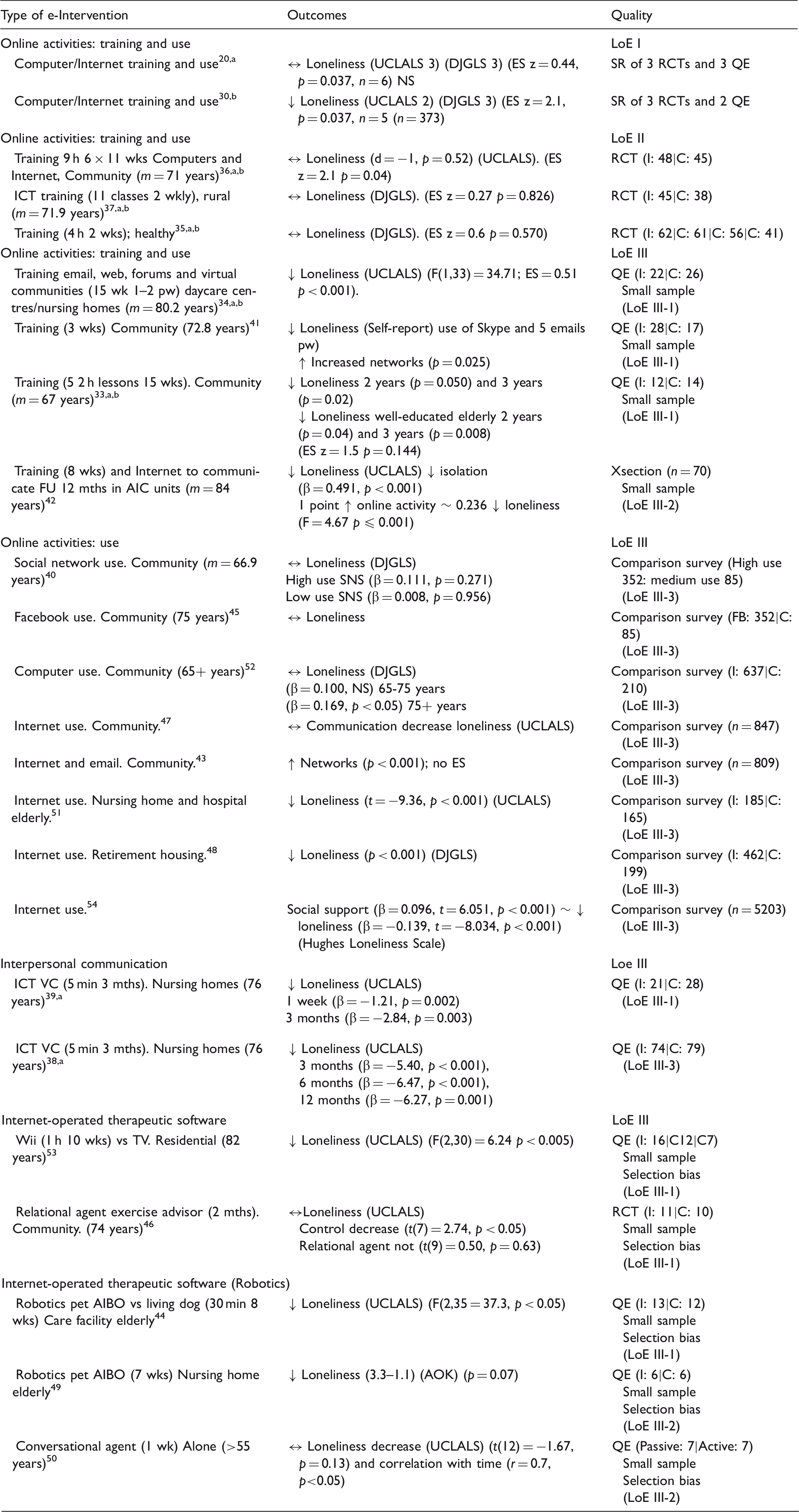
: significant decreased; ↑: significant increased; ↔: no significance; C: control; DJGLS: de Jong Gierveld Loneliness Scale; ES: effect size; I: intervention; LoE: level of evidence; mth: month; QE: quasi-experimental; pw: per week; RCT: randomized controlled trial; SR: systematic review; UCLALS: University California Los Angeles Loneliness Scale; wk: week.
Borneman SR; bChoi SR.
Internet/computer training
Seven studies evaluated computer/Internet training, three RCTs and four QE studies. The three RCTs 35 – 37 reported no significant decrease in loneliness measured by both the UCLALS and DJGLS (II). Some evidence of decreased loneliness was reported by the QE studies, including a sustained effect for up to three years. However, these studies were generally small and prone to bias (III-2). Use of computer/Internet was primarily assessed through cross-sectional studies (III-3), and evidence for associations for reduced loneliness was found and correlated to frequency of use (III-2).
Interpersonal communication
The two QE videoconferencing studies,38,39 reported evidence of effectiveness in reducing loneliness (III-2).
Internet-operated therapeutics
Modern technologies such as robotic pets and video games showed mixed evidence of decreasing loneliness, but the QE studies were small and prone to selection bias (III-3) (Table 3). No mHealth studies were found.
Discussion
In the context of reported increases of loneliness in the growing older population, 2 – 4 the scope and rigor of studies conducted in this field is not clear. This systematic review of reviews confirms the heterogeneity of the publications in this field 20 evidenced by varying definitions of older people, social isolation/loneliness and e-Interventions/ICTs/Internet-supported interventions. Some consistency existed in the measurements of loneliness, with most of the studies using either the DJGLS or the UCLALS. The review supported the findings from Bornemann, 20 showing consistency of sensitivity to loneliness across instruments. However, only four reviews were found with a specific focus on e-Interventions for loneliness in older people.20,23,28,30 The reviews were of moderate quality, with no reviews meeting all the R-AMSTAR criteria. The reviews also varied in scope, either with a specific focus on the effectiveness of a targeted e-Intervention such as computer training,20,30 or overviews of the published studies in the field.27,28 The criteria for inclusion of primary studies and quality assessment of these studies varied greatly with different tools used for rating rigor and bias. These variations would impact on the confidence in the conclusions of these reviews.
To assess the evidence of effectiveness of e-Interventions in this varied field, the interventions were classified into online activities, interpersonal, Internet-supported communications and Internet-supported therapeutics such as robotics, games and relational agents. The following conclusions emerged from the review.
Training and use of Internet/computer e-Interventions were not supported with conclusive evidence on the impact on loneliness. In examining the underlying studies, there appeared to be no definitive evidence of the effectiveness and sustainability of effectiveness. Level III-2 (cross-sectional studies) showed evidence of a correlation between use and loneliness, but the nature of the studies and the lack of an active intervention design, suggests further examination. Level III-2 studies, (QE two group evaluation studies), provided evidence of decreasing loneliness, but the low quality small-study designs suggest caution for future implementation. The level II (RCTs) studies showed no significant effect on decreasing loneliness and the two meta-analyses conducted in 2012 and 2014, including the same five core studies, with divergent pooled findings related to possible inclusion of different primary data in the meta-analyses. 20
The evidence for Internet-supported communication showed a significant reduction in loneliness, though this was mediated by self-efficacy 24 and frequency of use. 40 As e-Interventions may alleviate older people’s social isolation through different mechanisms, such as connecting to the outside world, gaining social support, and boosting self-confidence, 23 it would be important for studies to capture information on all these processes.
The emergence of the field of robotics showed some evidence of potential for decreasing loneliness, though the studies were small and biased. It would be important to explore the commonality between videogames, relational agents and robotics that allow for a decrease in social isolation/loneliness, as opposed to computer/Internet training and use, though no evidence of this was found.
This review confirmed the lack of high quality evidence in the field. In addition, despite the existence of guidelines to encourage the standardisation of systematic review reporting, the failure of researchers to adhere to such guidelines weakened the strength of the systematic reviews. The underlying studies lacked rigor in study design to address causation, and the heterogeneity led to challenges in generalizability of the primary research studies. Lastly, there is a need for research in mHealth interventions for social isolation as the grassroots uptake of mobile phones 55 may provide opportunities for increased uptake of e-Interventions to address loneliness in the older person.
Conclusion
In conclusion, due to the limitations of the reviewed primary studies and the reviews, insufficient quality evidence for the reduction of loneliness seems to exist to allow recommendations for e-Interventions for older people (Grade B).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.