
Abstract
Introduction
Decentralised services through outreach clinics or modern technology reduce patient travel time and cost to society. Telemedicine consultation through videoconference is one such modality. Here, we compared patient-reported health outcomes and satisfaction between video-assisted remote and standard face-to-face orthopaedic consultations.
Methods
This randomised controlled trial included two parallel groups: (1) patients receiving video-assisted remote consultation at a regional medical centre (RMC); and (2) patients receiving standard consultation at the orthopaedic outpatient clinic of the University Hospital of North Norway (UNN). This study included patients referred to or scheduled for a consultation at the orthopaedic outpatient clinic. After each consultation, patient satisfaction was determined using patient-completed questionnaires containing questions on patient-reported health (three-level European quality of life five-dimension index (EQ-5D-3L)/European quality of life visual analogue scale (EQ-VAS)) and questions from a validated OutPatient Experiences Questionnaire (OPEQ).
Results
This study included 389 patients, of which 199 received remote consultation and 190 received standard consultation (total of 559 consultations). In all, 99% RMC-randomised patients and 99% UNN-randomised patients evaluated the consultation as very satisfactory or satisfactory. Moreover, 86% RMC-randomised patients preferred video-assisted consultation as the next consultation. No difference was observed in patient-reported health after 12 months between the two groups. EQ-5D index scores were 0.77 and 0.75 for RMC- and UNN-randomised patients, respectively (p = 0.42).
Discussion
We did not observe any difference in patient-reported satisfaction and health (EQ-5D/EQ-VAS) between video-assisted and standard consultations, suggesting that video-assisted remote consultation can be safely offered to some orthopaedic patients. Moreover, a significantly high proportion of patients selected video-assisted remote consultation as their next consultation, thus strengthening the findings of this study. However, economic aspects should be assessed before widely recommending video-assisted consultation.
Keywords
Introduction
Patients require secondary-care consultation after referral from general practitioners or follow-up consultation for previous treatments or chronic diseases. Health authorities in Norway indicate that it is a public responsibility to provide necessary healthcare services to the entire population irrespective of their region of residence. Decentralised services through outreach clinics or modern technology reduce patient travel and cost to the healthcare system. 1 The University Hospital of North Norway (UNN) is a tertiary referral hospital of the Northern Norway Health Trust, covering approximately 470,000 inhabitants (2012) and a 112,975 km2 area. UNN also functions as a local hospital for Tromsø and northern Nordland County, covering 187,000 inhabitants (2012) and a 31,500 km2 area. In 2014, the authority’s expenses for patient travel, excluding expenses for ambulance transport by car, boat or air, accounted for 3.2% of the hospital’s total budget. 2 As one of the outpatient clinics with the highest number of patients, many of who require assistance by accompanying persons during travel or who cannot use public transport, it is of special interest to decentralise orthopaedic outpatient consultations.
The quality, cost and user-friendliness of telemedicine equipment are improving rapidly. These, along with the distribution of high-speed telecommunication, make it tempting to implement telemedicine without any further investigation. However, assessment of the quality and safety of given care, including patient satisfaction and economic impact of the intervention, is important in order to determine any pitfalls and to reduce unwanted events before employing this technology in routine healthcare. A previous non-randomised study showed good accuracy of telemedicine-assisted consultation for trauma management compared with that of standard consultation. 3 A randomised controlled trial (RCT) showed that telemedicine provided a satisfactory standard of care for managing minor injuries. 4 Another RCT found that telemedicine was a satisfactory technique for managing patients visiting an emergency department. 5 Other studies suggest that telemedicine can be used as an alternative to standard consultation for orthopaedic patients in an outpatient setting.6–9 One study showed that real-time videoconferencing was suitable for providing orthopaedic care in rural areas; however, further investigations, including cost–benefit analysis, were recommended. 10 Another study showed that telemedicine through a real-time videoconference effectively connected an Antarctic station to a medical centre in Japan for treating orthopaedic patients. 11 However, few RCTs have assessed the effect of telemedicine in orthopaedic patients, and none of these trials have been conducted in Norway.12–16 The quality of healthcare in general is complex and depends on many factors, including patient satisfaction. A review of studies on patient satisfaction with telemedicine found that the evidence concerning patient satisfaction with telemedicine is rather limited.17–19 An observational study regarding various paediatric surgical consultations at a children’s hospital found that both patients and clinicians reported great satisfaction with a telehealth consultation. 20 A pilot RCT conducted in 2012–2013 found that telemedicine (Skype) may be an alternative to some follow-up consultations for orthopaedic trauma patients, and patients reported similar levels of satisfaction as in-person visits. 21 There are few resent studies regarding telemedicine, patient satisfaction and out-patient clinics.
The present study compared the patient-reported quality of remote telemedicine consultation in an outpatient clinic with that of standard consultation during a prospective RCT that took place from 2007 to 2012. In this study, telemedicine refers to the use of real-time videoconferencing and digitalised radiography. Our hypothesis was that the introduction of telemedicine through a real-time videoconference in selected orthopaedic patients did not decrease the perceived quality of treatment administered by doctors involved in the consultation. The second hypothesis was that telemedicine increased patient satisfaction. A previous study from our group reported the professional quality of telemedicine in the same setting. 22 In the present study, we compared patient satisfaction and patient-reported outcome measures (European quality of life five-dimension index (EQ-5D) and European quality of life visual analogue scale (EQ-VAS)) between video-assisted remote orthopaedic consultation and standard consultation.
Methods
This RCT included two parallel patient groups that were randomised to receive remote consultation at a regional medical centre (RMC; intervention) and standard consultation at the orthopaedic outpatient clinic of the UNN (control). The study method, technical equipment, randomisation, sample size calculation and performance have been described in detail elsewhere. 22 Study patients were recruited from the four northernmost municipalities in Troms County in Northern Norway. Eligible patients were referred to or scheduled for a follow-up visit at the orthopaedic outpatient clinic at UNN, Tromsø. All the study patients provided informed consent and had orthopaedic conditions meeting the inclusion/exclusion criteria defined by the orthopaedists running the study (e.g. new referred, follow-up after surgery, trauma or chronic disorders). 22
Remote consultation was performed through real-time videoconference, with a trained nurse and patient at the remote location and an orthopaedic surgeon at UNN. No physician was present with the patient at the remote site. Standard consultation was performed at the orthopaedic outpatient clinic.
Patient satisfaction was assessed by administering questionnaires to the patients and orthopaedic surgeons after each consultation; in addition, a questionnaire was mailed to the patients at three and 12 months after the final consultation. The questionnaires that were answered immediately by the patients after the consultation included many questions from the Norwegian OutPatient Experiences Questionnaire (OPEQ), which was evaluated by Garratt et al. and is recommended for measuring patient experience in outpatient clinics. 23 We did not include all the items and questions of the validated OPEQ questionnaire, not including the core scale clinic access (both the questions) and questions on ‘unanswered questions’ (core scale communication), ‘background information available’ and ‘organisation of work’ (core scale organisation). As recommended, we only used relevant questions for scale information and pre-visit communication to keep the number of questions to a minimum. Besides, we used five-level questions (1 indicating very good and 5 indicating very bad) instead of a 10-point scale for maintaining uniformity in the final questionnaires. Hence, the motivation behind this scale compression was to ease the cognitive burden on respondents. We have not seen any evidence to suggest that such a simplification will impact on the validity of the OPEQ. In addition, the questionnaires included questions for determining overall patient satisfaction with the received consultation, previous experience with video-assisted consultation, preference of location for the next consultation, extent of agreement among different reasons for the preferred location (shortest travel time, give support to local offer, direct face-to-face meeting with orthopaedic surgeons or combination with other activity), travel distance and who completed the questionnaire. The patients randomised to receive video-assisted consultation were asked supplementary questions before and after the consultation to compare between telemedicine and standard consultations and were asked questions on technical performance. Both the questionnaires – that is, those given to the patients immediately after the consultation and those mailed to the patients at 12 months – included questions for assessing patient-reported outcomes (EQ-5D-3L and EQ-VAS). The EQ-5D was chosen because it is by far the most widely used generic preference-based instrument used in the literature. 24 Furthermore, it has demonstrated good responsiveness in patients with orthopaedic disorder. 25 As for the choice of value set, we applied the most widely used value set elicited from a British population, because no Norwegian value set was available. 26 English translations of the patients’ questionnaires used in the study can be viewed in the Supplementary materials in a previous publication. 22
Baseline data were collected using the questionnaire that was completed immediately after the first consultation. These included demographic variables (age, gender, occupation and education), indicators for measuring patient-reported outcomes and experience with different specialist outpatient clinics.
Results are presented as mean (standard deviation) or number (percentages). Differences between the groups were analysed using two-sample t-tests, chi-square tests or generalised estimating equations (GEEs). GEEs were used with an exchangeable covariance structure to control for dependence between two or more repeated consultations for some patients. McNemar’s test was used to assess changes in patient evaluation of video-assisted consultation. A p-value of less than 0.05 was considered significant. All statistical analyses were performed using STATA version 14.0 (StataCorp LP, TX, USA).
Results
Between November 2007 and August 2012, the trial randomised 402 patients, of whom 190 patients allocated to UNN (95%) and 199 allocated to RMC (98%) received consultations. A total of 559 consultations (257 at the UNN and 302 at the RMC) were conducted. At UNN the mean number of consultations was 1.35 (range 1–6) per patient, and at RMC the mean number was 1.52 (range 1–6). Across both arms, 547 questionnaires (249 UNN and 298 RMC) were completed immediately post-consultation (98% of the total consultations). In all, 143 (75%) UNN-randomised patients and 144 (73%) RMC-randomised patients returned the 12-month follow-up questionnaire. Missing data for single questions ranged from 0% to 12%, except for EQ-VAS at baseline, which was 25% for both UNN- and RMC-randomised patients. Flow chart and baseline characteristics, which were not significantly different between the groups, have been published previously. 22
Patients’ evaluation of the consultation per allocation.
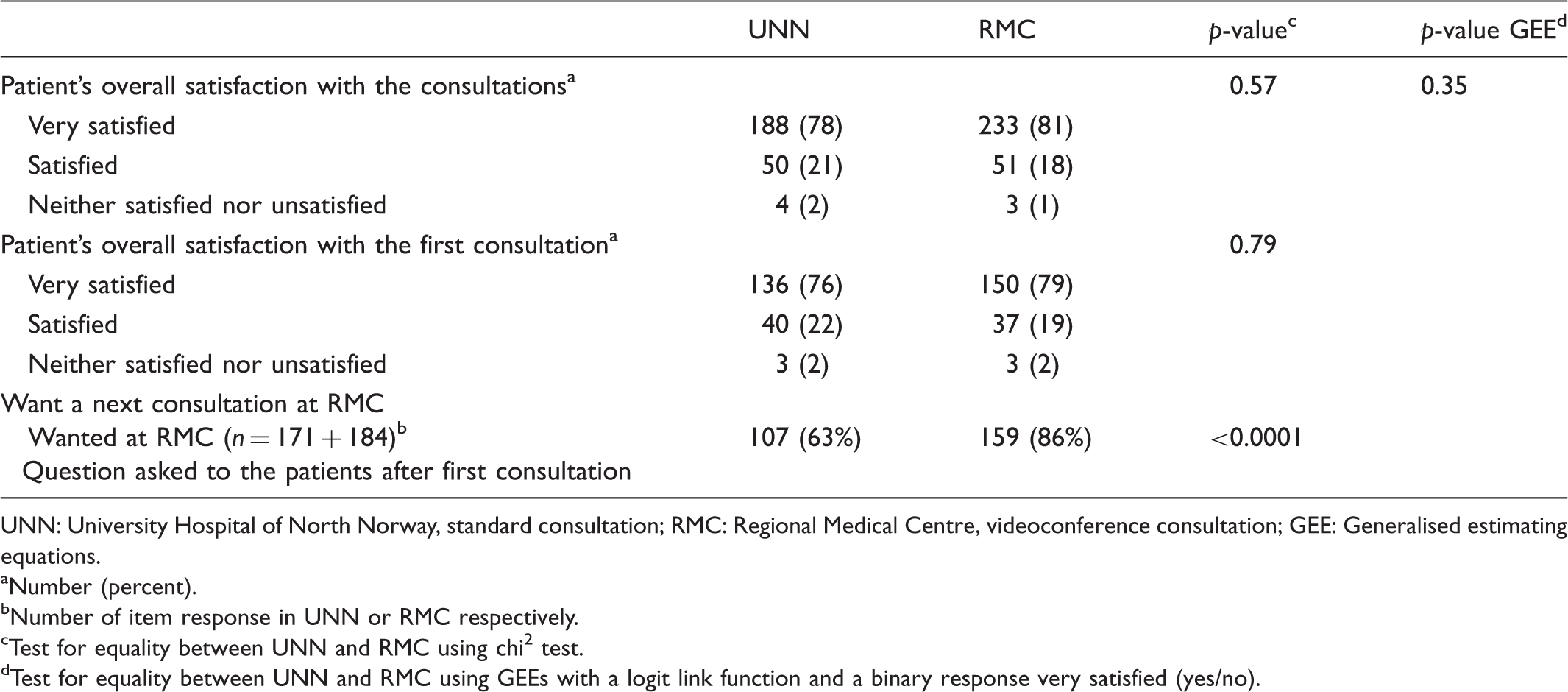
UNN: University Hospital of North Norway, standard consultation; RMC: Regional Medical Centre, videoconference consultation; GEE: Generalised estimating equations.
Number (percent).
Number of item response in UNN or RMC respectively.
Test for equality between UNN and RMC using chi2 test.
Test for equality between UNN and RMC using GEEs with a logit link function and a binary response very satisfied (yes/no).
Patients’ response to questions from OPEQ regarding the consultation per allocation.a

OPEQ: OutPatient Experiences Questionnaire; UNN: University Hospital of North Norway, standard consultation; RMC: Regional Medical Centre, videoconference consultation.
Values are number (percent) or mean ± standard deviation.
Number of item responses in UNN and RMC respectively. The number of responses to each item/question varies with a range of 217–243 at UNN and 273–292 at RMC.
Test for equality between UNN and RMC using t-test or chi2 test as appropriate.
Test for equality between UNN and RMC using generalised estimating equations (GEEs). A logit link function was used for binary responses (yes/no; no = No or Partial) and an identity link function for ordinal responses. For the question ‘Consulted about examination/treatment’, the answers ‘Did not want’ and ‘Does not apply’ were not included.
Five-level question (1 best, 5 worst).
New referred patient only (n = 55 UNN, n = 69 RMC) first consultation.
Patients’ self-reported health at baseline and 12 months per allocation.a
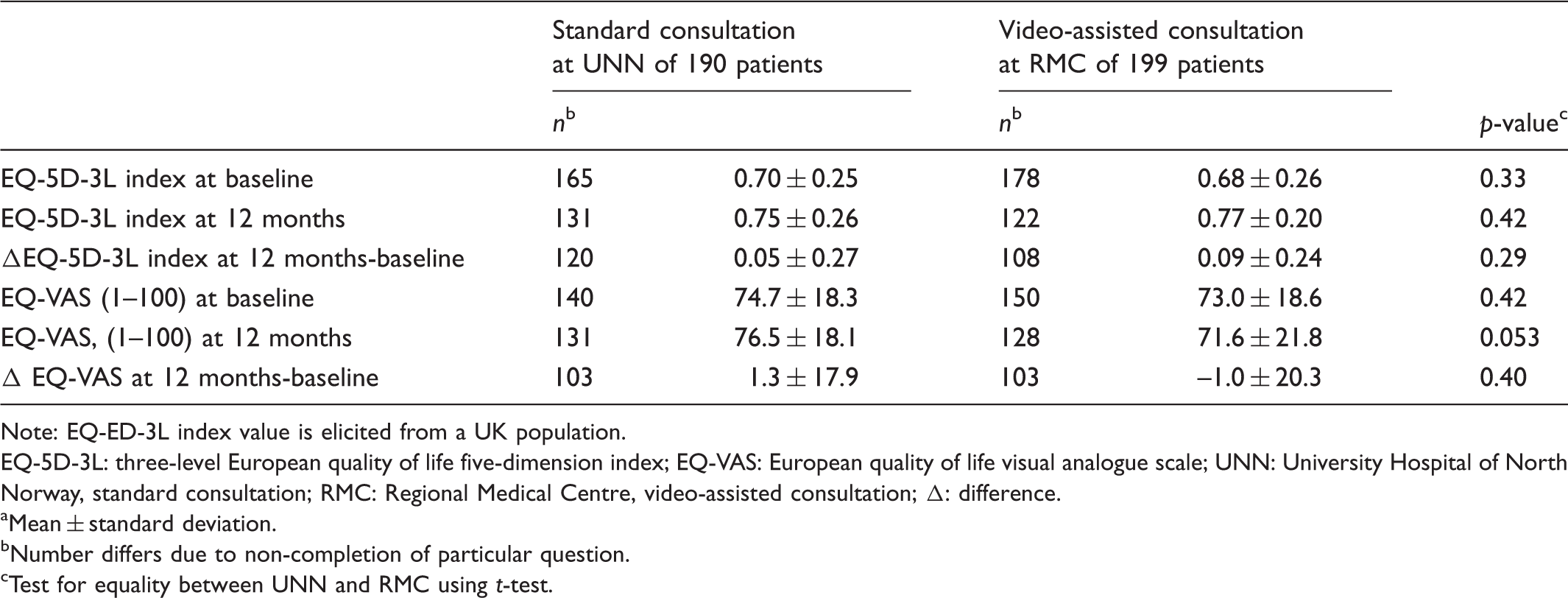
Note: EQ-ED-3L index value is elicited from a UK population.
EQ-5D-3L: three-level European quality of life five-dimension index; EQ-VAS: European quality of life visual analogue scale; UNN: University Hospital of North Norway, standard consultation; RMC: Regional Medical Centre, video-assisted consultation; Δ: difference.
Mean ± standard deviation.
Number differs due to non-completion of particular question.
Test for equality between UNN and RMC using t-test.
Distribution of EQ-5D-3L dimensions at baseline, 12 months, and difference between 12 months and baseline.a
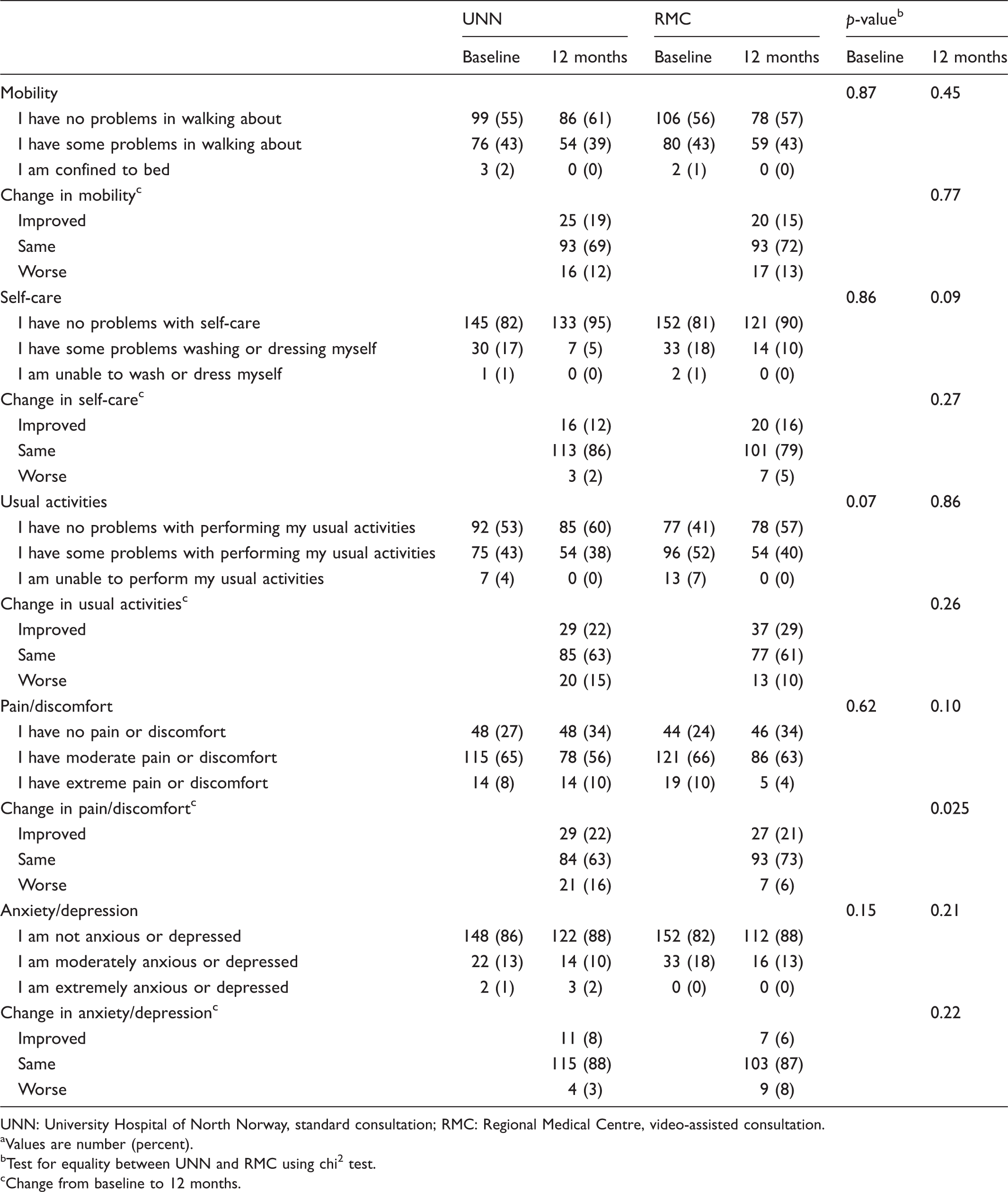
UNN: University Hospital of North Norway, standard consultation; RMC: Regional Medical Centre, video-assisted consultation.
Values are number (percent).
Test for equality between UNN and RMC using chi2 test.
Change from baseline to 12 months.
No significant difference was observed with regard to questionnaire completion between RMC- and UNN-randomised patients; completion by patients (77% and 76%, respectively) and by guardians (11% and 15%, respectively) (p = 0.60).
Telemedicine consultation
RMC-randomised patients were asked to express their thoughts about telemedicine and standard consultations before and after the consultation. Before the consultation, 23 (12%), 27 (14%), 82 (43%) and 14 (8%) patients graded video-assisted consultation to be much better, better, as good as the standard consultation and worse, respectively. After the first telemedicine consultation, these numbers changed to 28 (15%), 34 (18%), 120 (63%) and 8 (4%), respectively. In all, 44 (23%) patients did not have any opinion regarding the consultation type before the consultation. No significant change (p < 0.86) was observed in patient evaluation before and after the first consultation. Furthermore, six patients had previously received telemedicine consultation.
In all, 67%, 32% and 1% patients evaluated the technical performance to be very good, good and neither good nor bad, respectively. No video-assisted consultations were cancelled. Seventeen consultations were delayed (two consultations delayed for 75 and 60 minutes and the remaining consultations delayed for 17 minutes (mean)) because of technical problems.
Discussion
We did not observe any difference in patient satisfaction after video-assisted and standard consultations. However, we did not completely investigate the reasons underlying patient satisfaction or dissatisfaction with the consultations. We used the available validated Norwegian OPEQ because of the lack of a validated patient satisfaction questionnaire for video-assisted consultation in the outpatient setting in the initial phase of the study. We did not observe any significant difference in the core items, except for questions on ‘staff collaboration’ and ‘information-self-care’. Video-assisted consultation relies on a collaboration between the present persons. A nurse at a remote location retrieves a patient in the waiting area and plays an active part during the consultation. In contrast, a nurse was present in only 32% of the standard consultations. In addition, questions on support personal staff did not have the option ‘not relevant’, thus making it difficult to evaluate patient response on staff cooperation. In the question on ‘information-self-care’, patients were asked whether they were informed about their own contribution after the consultation. This was perceived better by RMC-randomised patients, which may be a coincidence. No significant difference was observed with respect to other questions on information or ease of understanding orthopaedic surgeons.
Patient satisfaction may be associated with short waiting time at the clinic. 27 In the outpatient clinic, delay may be caused by the need for the consultant to assist junior doctors asking for help. When having consultations with patients at remote locations by video-assistance, we do not leave the room to get the next patient and we are therefore less likely to be interrupted. Our experience is that the junior doctors also do not interrupt during a video-assisted consultation. Short waiting time at the clinic for remote consultation may be explained by this, in addition to a general desire of punctuality because of the new consultation form. This may stabilise with an increase in the use of video-assisted consultation. However, it is difficult to predict how this might influence patient satisfaction.
Quintana et al. showed that receiving assistance to complete the questionnaire may influence patient satisfaction. 28 In the present study, no significant difference was observed in questionnaire completion between RMC- and UNN-randomised patients.
Patients reported high overall satisfaction with the consultations, which was consistent with that reported in other studies on the satisfaction of orthopaedic patients.5,8,21 Nielsen et al. concluded that ‘effective communication is the key to patient satisfaction’. 29 We observed high positive values for all the questions concerning communication and information, and these values were high independent of the consultation type (Table 2). Wallace et al. observed higher treatment satisfaction among virtually treated patients than among conventionally treated patients. 30 However, their study included a different setting and specialities. A survey study on paediatric surgery telehealth conducted by Shivji et al. reported a high satisfaction rate among both patients and clinicians. 20 High patient satisfaction with telemedicine consultation is consistent with that observed in the present study which showed that a high proportion of patients receiving video-assisted remote consultation prefer this consultation in the future.
We reported earlier that the orthopaedic surgeons evaluated the consultation at UNN as very good (22%), good (78%) and neither good nor bad (0%) compared to at RMC 15%, 83% and 2%, respectively. 22 In our study, the patients were more satisfied with the consultation than the orthopaedic surgeons, which was consistent with that reported in another study. 31 In this other study, this is partly explained by an assumption that the fact that patients evaluated their own physician, on whom they are dependent for receiving care, made their evaluating more positive. 31 However, in our study, this situation was independent of the consultations form. We did not investigate the orthopaedic surgeons’ willingness to use video-assisted consultations in our study. This could be subject to further research since the actual physician’s viewpoint or attitude forms an essential part of when a wider implementation of telemedicine is planned. 32
The appropriate implementation of an RCT decreases unknown factors that may influence patient satisfaction. Randomisation is suggested to create a control group that maintains a balance between known and unknown confounding factors without selection bias. 33 We did not observe any significant difference between the groups, except for travel distance, which resulted because of allocation. The RMC is located 148 km from UNN and is the hub site for the region. Only 3.6% of UNN-randomised patients travelled < 150 km compared with 100% of RMC-randomised patients. One study reported that orthopaedic patients travelling < 50 miles (∼80 km) reported decreased satisfaction; 34 however, this was not observed in the present study.
Our study suggested increased pain reduction after 12 months in RMC-randomised patients (Table 4). Our study included patients showing different levels of acute deterioration of quality of life and patients with different degrees of chronic diseases. This might explain the small difference in reported pain reduction. However, our study showed reduced EQ-VAS score at 12 months in RMC-randomised patients (Table 3). This might explain the lack of improvement in patient-reported health at 12 months, although this question had a low response rate.
One limitation of our study is that we did not include all the recommended core scale/item questions to determine the most important aspects of patient experience with outpatient consultation. 23 We did not include questions on clinic access. At both the RMC and UNN, the waiting area was on the same floor and was not far from the main entrance. In addition, the patients were not asked directly whether they had any unanswered questions after the consultation.
Some studies indicate that questions on patient expectation of the consultation affect patient satisfaction. We did not include these questions in the present study; however, we believe that our study might have been strengthened by the inclusion of these questions.29,35,36 Another possible limitation is that our study did not include questions on transmission condition (picture, sound and privacy). When establishing the study design, we assumed that the video technology used would be satisfactory. This was true because 99% of patients and 92% of specialists reported very good or good technical performance. None the less, we recommend that problems concerning transmission should be considered in similar future studies because these problems represent three out of 10 items in the evaluated telehealth satisfaction scale. 37
In conclusion, we did not observe any difference in patient satisfaction and patient-reported health (EQ-5D) between video-assisted and standard consultations. This suggests that video-assisted remote consultation can be offered safely to selected orthopaedic patients. This conclusion was strengthened by the finding that a significantly high proportion of patients selected video-assisted remote consultation for their next consultation. However, various economic aspects should be assessed before recommending wide application of this consultation type.
Footnotes
Acknowledgements
We thank Solveig Nørgaard and Anne-Sofie Høgbakk for assisting in remote consultation; Jan Abel Olsen for providing professional assistance in planning the study and questionnaires; Ann Kristin Hansen and Vegard Fossum for collecting data; Kerstin Aune for assisting with the patient questionnaires; physicians and staff of the orthopaedic outpatient clinic and department at the UNN for recruiting patients; regional general practitioners for recruiting patients and Clinical Research Centre (UNN), Inger Sperstad, Samline Grimsgaard, Inger Sandstad, Norwegian Centre for Integrated Care and Telemedicine (UNN), Lars Rye, Jan Hugo Olsen and all the study patients.
Authors’ contributions
AB contributed to the study design, data collection, data analysis, interpretation and writing of the manuscript. EB contributed to the study design, interpretation and writing of the manuscript. GK contributed to data collection, interpretation and writing of the manuscript. AS contributed to the study design, data collection, interpretation and writing of the manuscript. TW contributed to the study design, data analysis, interpretation and writing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study was approved by the Regional Committee Research Ethics, Northern Norway, in 2007 (P REK NORD 134/2006).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a research grant from the Northern Norway Regional Health Authority (HST 950-10, ID 3543).
Trial registration
ClinicalTrials.gov identifier: NCT00616837. Because of organisational delays, this trial was registered on 22 January 2008. The specified study start date in ClinicalTrials.gov is November 2007.