
Abstract
Introduction
We describe the use of telepathology in countries with restricted resources using two diagnosis assistance systems (Isabel and Memem7) in addition to the diagnoses made by experts in pathology via the iPath-Network.
Methods
A total of 156 cases, largely from Afghanistan, were analysed; 18 cases had to be excluded because of poor image quality.
Results
Of the remaining 138 cases (100%), a responsible physician provided a tentative diagnosis for 61.6% of them. With a diagnosis from a consultant pathologist, it was then possible to make a definite diagnosis in 84.8% of cases on the basis of images taken from hematoxylin and eosin staining sections alone. The use of the diagnosis assistance systems resulted in an ordered list of differential diagnoses in 82.6% (IsabelHealth) and in 74.6% (Memem7) of cases, respectively. Adding morphological terminology reduced the list of possible diagnoses to 52.2% (72 cases, Memem7), but improved their quality.
Discussion
In summary, diagnosis assistance systems are promising approaches to provide physicians in countries with restricted resources with lists of probable differential diagnoses, thus increasing the plausibility of the diagnosis of the consultant pathologist.
Introduction
The task of pathology is to provide a morphological diagnosis for diseases, which are defined by morphological features. These morphological diagnoses are included in the final clinical diagnosis and shall support the responsible physician in making far-reaching diagnostic or therapeutic decisions. Morphological diagnoses in western countries are highly sophisticated and often go far beyond the local possibilities in underserved countries, where additional immunohistochemical and molecular biological tests are not available, so that, for instance, subtypes of lymphomas, soft tissue and cerebral tumours cannot be diagnosed accurately. 1
Like teleradiology, telepathology is a well-accepted form of information technology. Static telepathology allows diagnoses to be made on still images.2,3 Telepathology on frozen sections is applied to overcome the distance between institutions at intraoperative examinations during surgery.4,5 Dynamic telepathology enables pathologists to examine whole histological sections or cytological smears over any distance.6–8 The promising application of these approaches in countries with restricted resources is well documented.9,10 “Hybrid telepathology” combines video consultations and store-and-forward communication.10,11 On the whole, telepathology, including teleteaching,7–13 is a promising method to connect the knowledge of consultant pathologists with the requirements of a physician in an underserved country.
In this study, we report our experience in making telepathological diagnoses in combination with two Internet-available diagnosis assistance systems.
Methods
Patients
The study is based on data from 138 patients (after excluding 18 cases with poor image quality) generated by two kinds of Internet platforms: the first approach to the cases was the tele-communication system iPath-Network, 14 a Web-designed platform for discussing medical cases with special concern to pathology and radiology. It houses multiple discussion groups and forums according to participating institutions. The data used for the present study belong to the groups of Afghanistan 15 and Tanzania as well as the forum of Histopathology, 16 Cytopathology 17 and Dermapathology 18 (Table 1). Eighteen of the 156 cases were excluded from the study because the image quality was considered unacceptable (Table 2). The second approach to the cases was the use of two diagnosis assistance systems (see the following section).
Study patients.
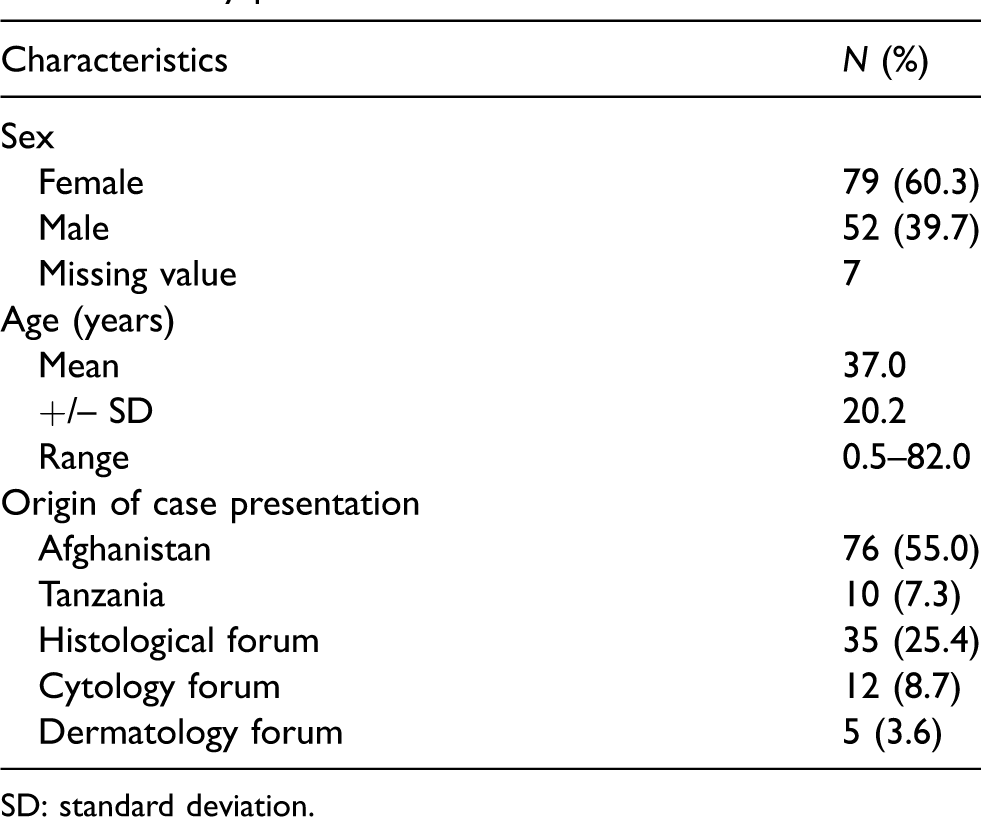
SD: standard deviation.
The physicians responsible for the primary morphological diagnosis (RM, FH, KH, SK, MD, DM, OM) comprised five pathologists, one surgeon and one specialist in head and neck diseases.
Study design
Patients’ data (see also Table 2 and 3) are sent to the appropriate group or forum in order to get a second opinion diagnosis by an experienced consultant pathologist. For this purpose, the local responsible physician sets images taken from histological sections or cytological smears on the iPath-Network 14 with or without his tentative diagnosis, combined with the most important clinical information regarding patient’s gender, age, location of the lesion, macroscopic findings and clinical symptoms. Each patient is characterized by a iPath code consisting of a six- to seven-decimal-place number. No personal data are reported on the iPath platform. Identification of the patient is only possible for the responsible physician. On the basis of these data the consultant pathologists (PF, KDK, GS, PD, GJ, NH, KA) make a diagnosis or a differential diagnosis available to the responsible physician. Images for which a diagnosis was possible, despite low-standard image quality, were regarded as acceptable (see, for example, Figure 1). The diagnoses were made without asking for additional examinations. If more than one consultant pathologist evaluated the images and discrepant diagnoses emerged, the opinion of the most experienced person, who has the position of the moderator of the group or forum, was considered as correct. The speciality of the consultation is given in Table 3.
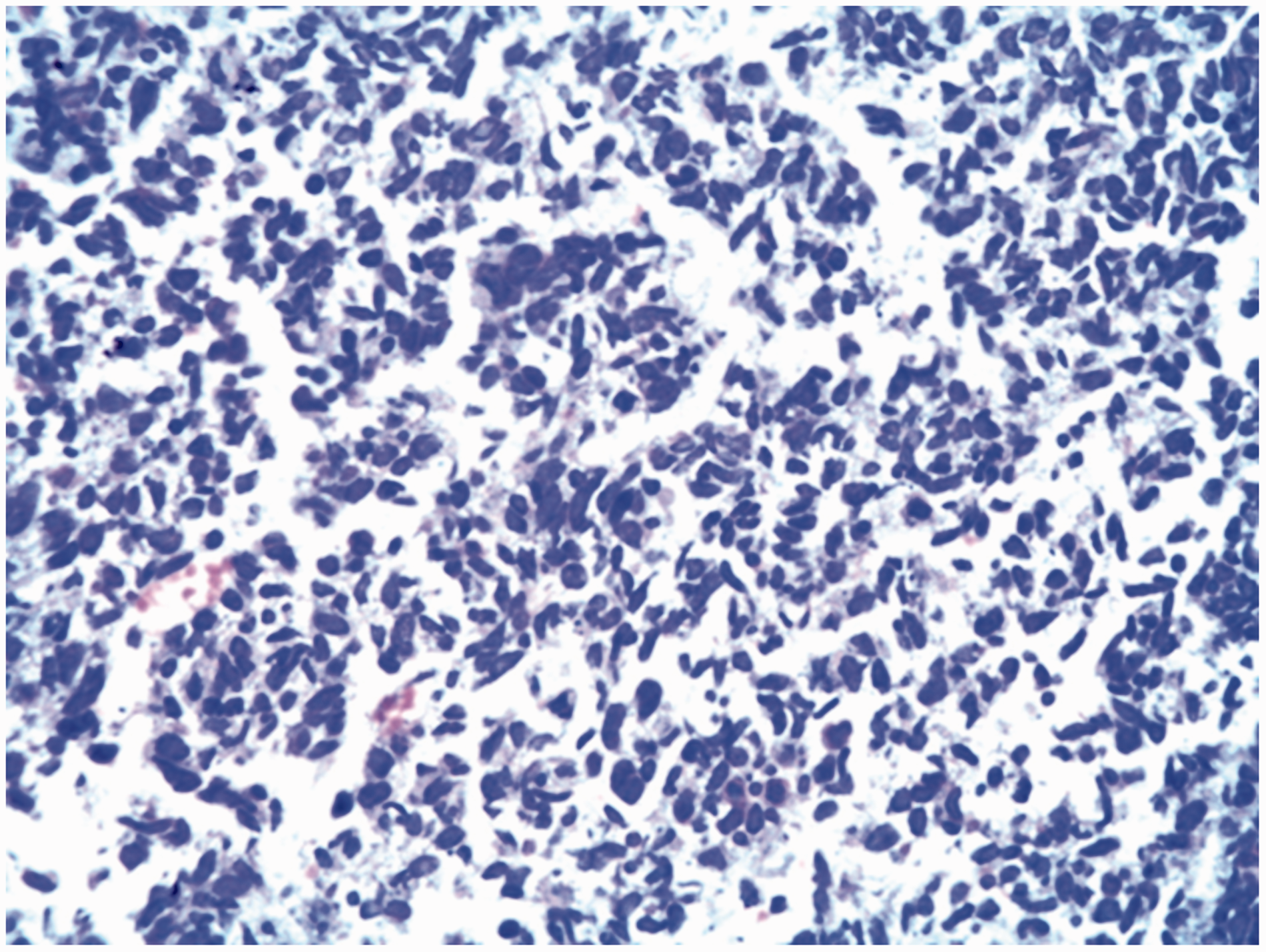
Breast tumour (demonstration case) in a young female.
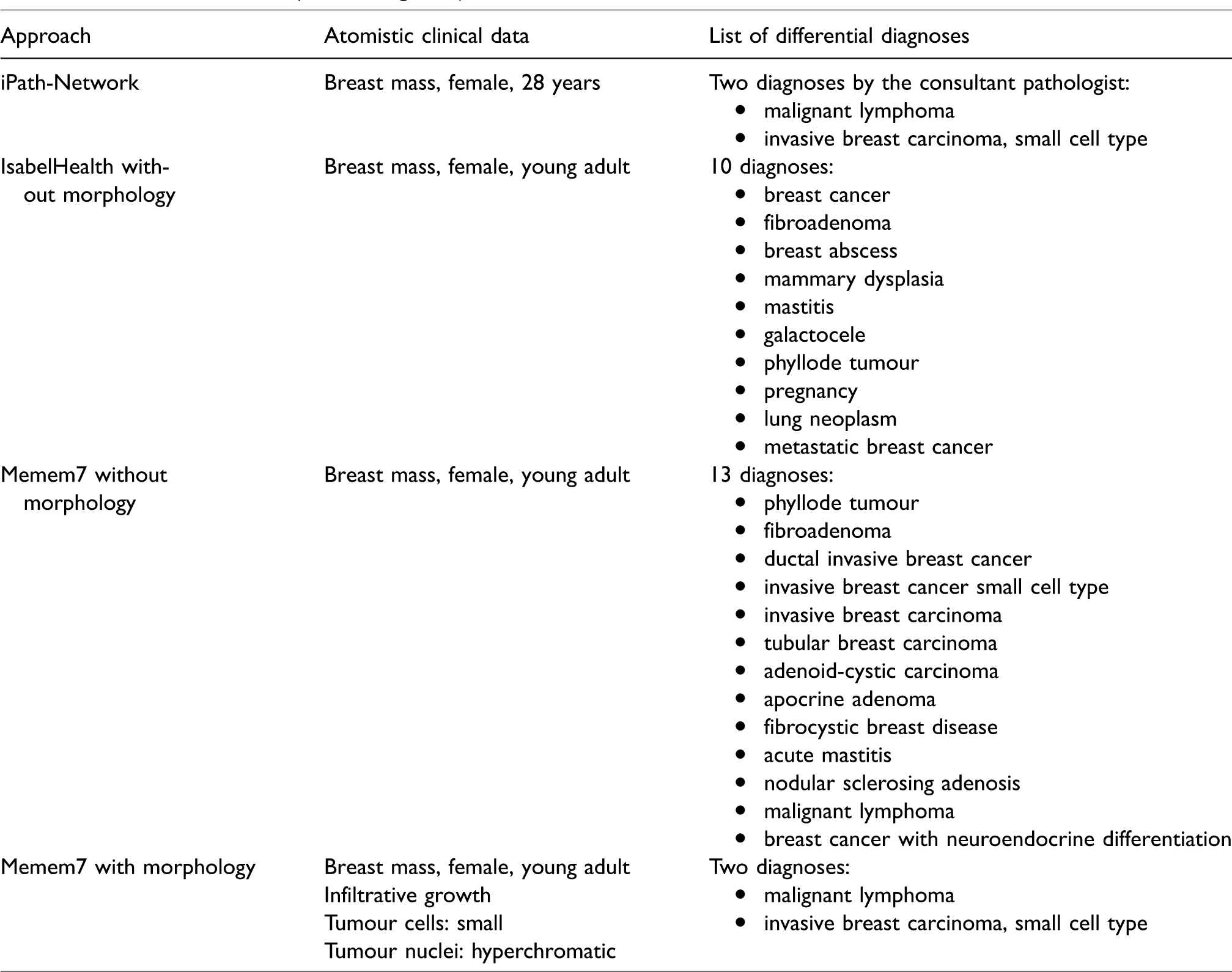
In a second step, data from the 138 evaluable patients gained by the iPath were used to check the utility of two diagnostic assistance systems accessible via the Internet. One is the commercial Isabel platform (version 9/2018), 19 the other is the non-profit Memem7 platform (version 10/2018). 20 After the input of the most reliable “atomistic” clinical terms like gender, age, involved organ and other findings, the systems automatically produced a list of possible diagnoses – in the case of Isabel, in a descending order of probability. The executing search function and algorithms are not evident for the user in both systems. Different from the Isabel system, the Memem7 system also enables the use of atomistic morphological terms like glandular growth pattern, cell polymorphism and/or similar terms. This is demonstrated in Table 4 and Figure 1, using the example of a 28-year-old female patient with a unilateral breast mass. For the cases that include the morphological findings, we discriminated four subgroups: (1) Memem7 confirmed the expert diagnosis without a further differential diagnosis; (2) Memem7 confirmed the expert diagnosis with one further differential diagnosis; (3) Memem7 confirmed the expert diagnosis with more than one differential diagnosis; and (4) the expert diagnosis was not found by Memem7, but at least one alternative diagnosis was delivered.
One of the authors (PF) classified the results as helpful or not helpful. A diagnosis was considered as helpful if a diagnosis or a list of differential diagnoses was provided by the diagnosis assistance systems. Results were considered not helpful if no list of differential diagnoses could be provided by the diagnosis systems. Since these additional tests were only applied belatedly in the frame of this study, the results were not made available to the responsible physician.
Evaluation of data
The following parameters were evaluated: 1) accordance between the diagnoses of the consultant pathologists and the diagnosis of the responsible physician; 2) the cases in which the responsible physician did not make a tentative diagnosis; 3) the number of cases in which no definite diagnosis was possible for the consultant pathologist; 4) the results of the diagnosis assistance systems including the number of atomistic terms needed for the case description; 5) the number of cases with no reliable results in the diagnosis assistance systems; and 6) the number of cases in which no diagnosis could be made available because of poor image quality.
Statistical analysis
For the statistical analysis, we used the R software package (version 3.4.2) 21 ; p < 0.05 was considered to be significant.
Results
Telepathological diagnoses without diagnosis assistance systems
Eighteen cases (of 156 patients) were not accepted for a morphological diagnosis because of poor image quality (Table 1). Adding the eight cases where no morphological diagnosis was possible for medical reasons, 26 cases of 156 (corresponding to 16.7%) could not be evaluated by telepathology (Table 2). Most study patients were from Afghanistan (Table 1).
Morphological diagnosis of responsible physician.
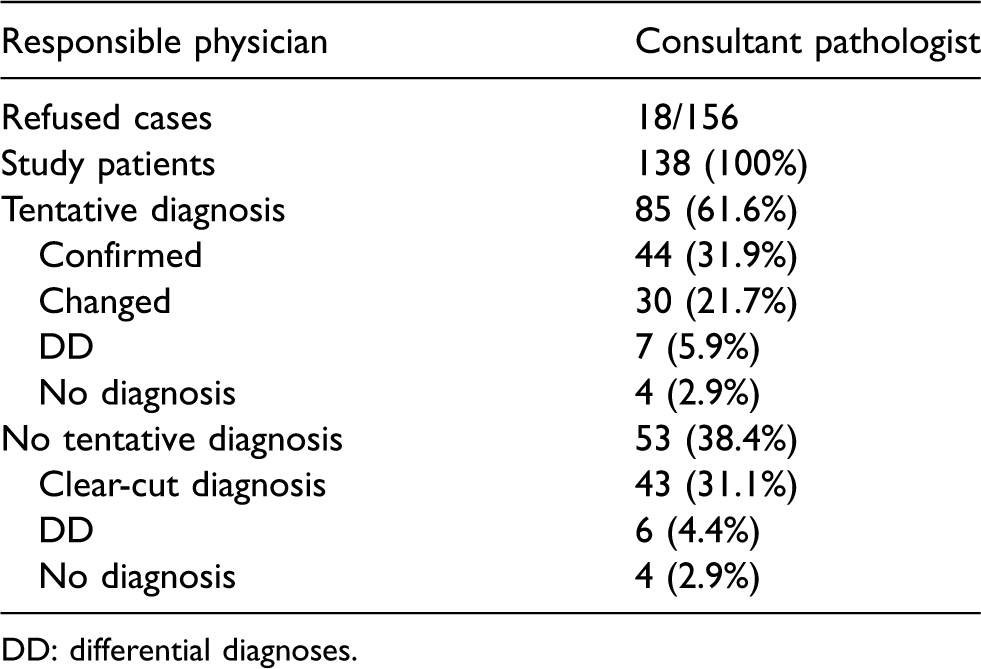
DD: differential diagnoses.
Within the study group of 138 patients with evaluable pictures on the iPath, the ratio of female/male was 1.5:1; the mean age was 37 ± 20 years. In 85 cases (61.6%) the responsible physician proposed a diagnosis, which was confirmed in 44 and changed in 30 cases; in seven cases only a differential diagnosis was made available and in four cases no diagnosis was possible (Table 2). In 53 of 138 cases (38.4%) no tentative diagnosis was provided by the responsible physician. In 43 of them (311.%) the consultant pathologist could make a diagnosis, in six (4.4%) a list of differential diagnoses was made available and in four cases (2.9%) there was no diagnosis made available.
Of the 138 cases, the consultant pathologist made a definite diagnosis in 117 cases (44 + 30 + 43 cases, corresponding to 84.8%), compared to 61.6% in the case of the primary physician. In 13 cases he offered a list of differential diagnoses and in eight cases he offered no diagnosis. The number of cases in which no definitive diagnosis was made available by the consultant pathologist was not dependant of the specialist discipline (p = 0.29; Table 3).
Evaluation of diagnosis depending of medical discipline.

The evaluation of diagnosis assistance systems without added morphologic aspects
The expert considered the Isabel and Memem7 differential diagnoses list as helpful in 114/138 (82.6%) and 103/138 (74.6%) cases, respectively. This difference between both systems is not significant. The reason for giving a positive assessment was a short overview about possible diagnoses and prevention of forgetting an unusual diagnosis or syndrome. Isabel provided an average of 37.8 (standard deviation (SD) ± 19) diagnoses as compared to 29.7 (SD ± 41.5.9) for Memem7. This difference was not significant (p = 0.43). For describing a case we used an average of 3.5 terms (+/−0.7) in Isabel and 4.0 (±1.4) in Memem7. This difference was significant (p = 0.0007).
Evaluation of diagnosis assistance systems with added morphological aspects
Contrary to Isabel, Memem7 has morphological terms included in its term thesaurus and, therefore, a list of morphological differential diagnoses can be provided. The average number of differential diagnoses was 3.9+/–9. When we added the morphological details the number of tuples needed to describe the case to be investigated raised to 5.7 ± 1.1. The 72 cases that included morphological findings were divided into four subgroups: (1) 19 cases corresponding to 26.4% with a confirmed expert diagnosis, but without a further differential diagnosis; (2) 11 cases corresponding to 15.3% of the cases with a confirmed expert diagnosis and one additional differential diagnosis; (3) 35 cases (48.6%) with a confirmed expert diagnosis and more than one differential diagnoses; and (4) seven cases (9.7%) with no confirmed expert diagnosis, but at least one proposal of a diagnosis.
Discussion
Classifying diseases by morphological methods is one undisputed basis for reaching a final clinical diagnosis, allowing curative or palliative treatment. In countries with restricted resources, there are some serious problems that conflict with using this approach: (1) the non-availability of a pathology service; (2) technical problems such as tissue embedding and staining methods; (3) a lack of additional methods for reaching a final morphological classification; and (4) a lack of experienced pathologists. Problems (2), (3) and (4) can be addressed by telemedicine, and one frequently used system is the iPath-Network.2,3 The expectance of the responsible physician is either the confirmation of his diagnosis, an expert diagnosis or a list of possible differential diagnoses. Even if the responsible physician proposed a diagnosis, a confirmation of this tentative diagnosis by the consultant pathologist is considered as very helpful by all responsible physicians.
In 84.8% (117/138) of cases the consultant pathologists were able to give a probable diagnosis or a list of differential diagnoses using a Web-designed platform for morphological images. Our results of a positive appraisal of telepathology in countries with restricted resources is in line with several publications.22–26
We analysed two diagnosis assistance systems with and without morphological descriptors. Both systems were interchangeable, with no statistical significant differences in the number of broadened differential diagnoses. The results of the diagnosis assistance systems were considered helpful in 82.6% (IsabelHealth) and 74.6% (Memem7) of cases. If morphological terms were added (only possible in Memem7), in 52.2% of cases a list of one or more morphological diagnoses were made available by the diagnosis assistance system, exemplified by the demonstration case (Table 4 and Figure 1). In this case both diagnosis assistance systems offered a list of possible differential diagnoses, thus making available a plausibility control for the expert diagnosis. When using Memem7, which allowed the inclusion of morphological findings, the same two differential diagnoses are reported as proposed by the expert.
Demonstration case (see also Figure 1).
Diagnosis assistance systems are helpful in (1) broadening the lists of differential diagnoses, (2) the confirmation of a diagnosis in case of uncertainty and (3) considering rare and largely unknown syndromes and orphan diseases. When a new diagnosis is proposed by the consultant pathologist, he can provide the information included either in Memem7 or especially in IsabelHealth about this disease entity to the local physician and participate this information with the responsible physician. The written report of the iPath-Network may be completed by the Internet source recoded in the diagnosis assistance systems.
There are continuous improvements by the Memem7 system by optimizing both the medical semantic net and the disease coding by numerous feedback and supervised learning algorithms.
In summary, we report a promising approach in combining expert diagnoses in telepathology with diagnosis assistance systems. Both investigated systems were helpful on the level of clinical data, and one system also proved to be helpful in supporting a probable morphological diagnosis or in finding further morphological diagnoses.
Telecytology, telepathology or whole-slide imaging is now considered to be an inherent part of pathology.8,27 Beyond these positive statements, our approach combining telepathology with diagnosis assistance systems has some promising aspects: (1) the probabilistic ranking of diagnoses lists, taking into consideration age, disease duration and sex; (2) Web-assisted insights into the proposed diagnosis; (3) adding machine learning systems to the diagnosis assistance systems; and (4) adding technological advancements like android smartphones to telepathological methods.28,29
Ethical aspects
All cases were anonymous. Names and birth data of the presented patients were unknown to the consultant pathologist. Sex, age, localization and disease duration were known and, in rare cases, a macroscopic image was available; if diagnosis concerned the visage, the eyes were blinded. The authors have written approval that the images provided can be used for scientific analysis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the Robert Bosch Foundation, Stuttgart, and Sabine-Dörges-Stiftung, Ludwigsburg.