
Abstract
Introduction:
Physical rehabilitation for total hip replacement patients following hospital discharge is beneficial; however, accessing rehabilitation is often challenging. Telerehabilitation helps negate access issues and is efficacious in total knee and hip replacement patients. This study aims to compare the cost-effectiveness of a telerehabilitation programme delivered remotely into patients’ homes versus traditional care for total hip replacement patients following hospital discharge.
Methods:
A cost-effectiveness (cost-utility) analysis was conducted from the perspective of a health service alongside a two-arm randomised controlled trial comparing telerehabilitation (n=35) with in-person care (n=35) following hospital discharge after total hip replacement. The primary analysis used an Incremental Cost-Effectiveness Ratio to compare the cost per Quality Adjusted Life Year (QALY) accrued in the telerehabilitation group versus in-person control using costs and effects data from the randomised trial. A secondary analysis was conducted whereby the time accrued by patients attending rehabilitation sessions (including travel time) was considered the “cost” (i.e. a time burden), rather than cost from the health service perspective.
Results:
Estimated mean differences in healthcare costs and QALYs gained were detected but were not significant. The estimated mean (95%CI) difference in cost of telerehabilitation versus in-person was –$28.90 (–$96.37 to $40.45), favouring the telerehabilitation group. The estimated mean (95%CI) difference in QALYs gained from telerehabilitation versus in-person was –0.0025 (–0.0227 to 0.0217). The estimated mean (95%CI) difference in time burden favoured less time burden for the telerehabilitation group (–4.21 (–4.69 to –3.74) hours).
Discussion:
Telerehabilitation in the total hip replacement population incurred similar costs and yielded similar effects to traditional in-person care. Telerehabilitation significantly reduced the time burden for patients and carers. These findings are valuable for healthcare providers seeking to implement accessible patient-centred rehabilitation services.
Introduction
Hip replacement is the gold standard treatment for severe hip osteoarthritis. There has been an increase of approximately 55% in procedures over the last decade, with over 45,000 and 85,000 hip replacements being performed in Australia and the United Kingdom, respectively, in 2016.1,2 Physical rehabilitation for total hip replacement (THR) patients following hospital discharge is beneficial;3–7 however, transportation challenges and travel expenses 8 can impede access to centre-based rehabilitation due to driving restrictions and impaired mobility in the acute post-operative phase. 9 Telerehabilitation, or the provision of rehabilitation care through telecommunications technology, helps negate access issues by enabling the delivery of care directly into the home of the patient. Telerehabilitation following total knee and hip replacement is efficacious, with patients achieving comparable physical and functional outcomes10–12 while maintaining high levels of patient satisfaction compared with in-person programmes.13–15
The cost-effectiveness of telehealth and telemedicine is generally inconclusive. Mistry et al. 16 conducted a critical appraisal of systematic reviews assessing cost-effectiveness of telemedicine studies. They reported that methodological flaws in the economic analysis of the studies included in the review meant that conclusions could not be drawn on the cost-effectiveness of telemedicine applications. Over time, reporting of cost-effectiveness has generally improved; however, there is still room for improvement. A systematic review by de la Torre-Díez et al. supported this, concluding that while some cost-effectiveness studies demonstrate that telemedicine can reduce costs, a lack of randomised controlled trials, small sample sizes and absence of quality data remain as limitations. 17
Cost-effectiveness information is critical for informing resource-allocation decisions related to sustainable telerehabilitation models in the context of value-based healthcare systems. Cost-effectiveness studies in the orthopaedic population have yielded encouraging results. A Canadian-based cost-analysis study which compared telerehabilitation with in-person care (via home visits) in total knee replacement patients found favourable results for the telerehabilitation group. 18 Patients received 16 sessions of their respective rehabilitation model, with telerehabilitation shown to be cheaper (total cost differential –$263 (95%CI –$382 to –$143). Of note, telerehabilitation was only cheaper than in-person care if the therapist conducting home visits had to travel greater than a 30 km round trip. 18 Fusco and Turchetti explored the cost-effectiveness of a resource-intensive (20 treatment sessions) mixed telerehabilitation-standard rehabilitation programme after total knee replacement that consisted of 10 in-person rehabilitation sessions followed by 10 telerehabilitation sessions versus 20 in-person rehabilitation sessions. 19 They concluded that the mixed telerehabilitation intervention was more cost-effective from a healthcare provider perspective, yet findings were dependent on whether the healthcare provider or patient were accountable for patient travel costs.
To date there have been no cost-effectiveness studies comparing telerehabilitation with traditional care in the THR population. This study aims to compare the cost-effectiveness of a post-acute telerehabilitation programme delivered remotely into patients’ homes versus traditional care for THR patients following hospital discharge.
Methods
Design
A cost-effectiveness (cost-utility) analysis was conducted from the perspective of a health service alongside a two-arm randomised controlled trial comparing telerehabilitation with traditional care following hospital discharge after THR. 15 A 6-month time horizon was selected because it captures the timeframe in which most costs and benefits related to telerehabilitation versus in-person rehabilitation for this clinical population are likely to be accrued, and was consistent with the final follow-up assessment of the clinical trial. No discounting of costs or effects was warranted, as the timeframe was less than 1 year. The decision tree for this study is presented in Figure 1.

Decision tree for this trial-based economic evaluation.
Participants and setting
This study was conducted in a metropolitan hospital in Brisbane, Australia. This hospital has the infrastructure to provide a physiotherapy rehabilitation service in-person in a traditional clinic setting within the hospital, or via telerehabilitation with clinical staff using tablets or notebook computers. Participants included the trial participants who had received a THR and been randomised to the telerehabilitation (n = 35) or traditional care group (n = 35). The mean (SD) age of participants was 64 (10) years, and 44 (63%) were female. 15
Trial intervention and intervention-related procedures
The trial methodology is published in a detailed protocol manuscript. 20 In summary, participants were randomised to a traditional in-person (control) or telerehabilitation (intervention) group and undertook a 6-week rehabilitation programme. Interventions 20 for both groups were performed by physiotherapists trained in the delivery of a standardised exercise programme. The programme was progressed based on physiotherapists’ assessment during the 6-week intervention period.
On discharge from hospital the control group received traditional care, 21 defined as a standardised paper-based home exercise programme targeting hip-strengthening exercises. Participants were instructed to perform the home exercise programme three times daily and self-monitor compliance using an exercise diary. At 2, 4, and 6 weeks post-operatively, participants attended an outpatient clinic for a 30-min in-person physiotherapy session focussing on gait and reviewing and progressing their home exercise programme.
The intervention programme was identical in content to the control programme, with the mode of delivery being directly into patients’ homes via telerehabilitation technology using applications on an Apple iPad™. Home exercise programmes were facilitated using the Wellpepper clinic (Wellpepper Inc, Seattle, WA) application and physiotherapy sessions conducted via the eHAB telerehabilitation application (NeoRehab, Brisbane, Australia). Wellpepper enables healthcare professionals to create exercise programmes for patients to follow on a tablet device. The application provides videos and instructions to guide patients through the home exercise programme and monitors compliance by the patient indicating which exercises they have completed. eHAB is a clinically validated telerehabilitation system that enables real-time videoconferencing into the home. One to two days prior to discharge, the intervention group were loaned an iPad with Wellpepper and eHAB installed to use for the duration of the 6-week intervention period. All iPads were connected via a prepaid mobile internet plan for use during the intervention.
The intervention group received three automated reminders per day via Wellpepper to perform their home exercise programme. Two weeks after discharge, the intervention group received a physiotherapy session via real-time videoconferencing using eHAB, where analysis and advice regarding gait and their home exercise programme were undertaken. If abnormalities were observed in mobility (gait pattern and reliance on walking aid) or the ability to perform their home exercise programme correctly, an additional eHAB appointment at 4 weeks post-operatively was scheduled. Participants continued to use Wellpepper to facilitate their rehabilitation until 6 weeks post-operatively. At the conclusion of the intervention period, all participants were provided with a paper-based home exercise programme to continue independently.
For patients who walked unaided prior to surgery, but were unable to complete a Timed Up and Go test 22 unaided 6 weeks after their surgery, additional in-person physiotherapy sessions were provided. The determination of whether a person was able to complete the Timed Up and Go test unaided was made by the physiotherapist (blinded to group allocation) who conducted the 6-week assessment. All sessions beyond the 6-week intervention period were centre-based in-person appointments, regardless of allocation to the control or intervention group, and were considered within scope of rehabilitation healthcare resource use for both groups.
Health outcome measures
The measure of effect for this cost-utility analysis was Quality Adjusted Life Years (QALYs) derived from EuroQol-5D-5L (EQ-5D-5L) assessments collected during the trial. The EQ-5D-5L was completed by patients at baseline, 6 and 26 weeks post-operatively. Published Australian population preference weights were applied to EQ-5D-5L responses provided at each assessment to generate multi-attribute utility scores and calculation of QALYs using an area under the curve approach. Mean and 95%CI multi-attribute utility estimates were calculated for each group at each assessment, as well as for total QALYs accrued within the 6-month time horizon. To overcome the risk of biased uncertainty estimates due to the potential for non-normal distributions in these data, uncertainty estimates were produced using bootstrap resampling (2000 replications, bias-corrected confidence intervals). Furthermore, to protect against the potential influence of any imbalance in baseline EQ-5D-5L on subsequent QALY-incremental cost-effectiveness ratio estimates, baseline EQ-5D-5L was pre-specified for inclusion as a covariate in all QALY-related incremental cost-effectiveness analyses. Sensitivity analyses were conducted to examine whether the inclusion of baseline EQ-5D-5L was influential on effect estimates in comparison to unadjusted analyses; however, adjusted and unadjusted QALY effect estimates were entirely consistent (therefore, only pre-specified EQ-5D-5L adjusted estimates are presented).
Resource use and valuation of costs
Resource use was collected from the perspective of the rehabilitation healthcare provider. This was inclusive of clinician labour associated with physiotherapists delivering the rehabilitation interventions (via telerehabilitation or in person). Clinical staff at the participating facility typically use comparable computer workstation/notebook or tablet hardware whether or not their patients receive rehabilitation in the clinic or via telerehabilitation; however, provision of telerehabilitation required additional software subscriptions (Wellpepper and eHAB) which were recorded and costed on a per-patient basis for patients receiving telerehabilitation. In addition, patient time and out-of-pocket costs for travel to attend clinic appointments were reported by patients for each session (not included in healthcare provider perspective analyses). Hospital administrative records were also used to verify and corroborate appointment-related resource use recorded for patients during the trial.
For the purpose of the trial, participants in the telerehabilitation group borrowed a tablet (with data SIM card for internet access) from the research team to ensure intervention fidelity was consistent across the telerehabilitation group. However, as the investigators did not consider this (lending a mobile device with internet access) to be a cost that would usually be borne by a healthcare organisation offering a telerehabilitation service, this has been costed and reported for the readership and included in a sensitivity analysis, but not the primary analysis from the perspective of the health service provider. This is important to note, as it means the primary analysis from the perspective of the health service assumes that patients choosing to access a telerehabilitation service would be able access a suitable internet connection with an appropriate device. Following completion of the planned 6-week intervention period, monthly phone calls were made to any participant continuing to receive rehabilitation interventions related to their hip replacement to ensure any other ongoing healthcare resource use data from the perspective of the health service (e.g. further in-person appointments for those who were not yet independently mobile) could continue to be recorded (all participants had completed rehabilitation therapies within the study time horizon).
All participants had healthcare resource use data collected during the trial (none missing) which were costed at market rates in 2018 Australian dollars. The primary source for healthcare market rates was the Australian Independent Hospital Pricing Authority 23 (inclusive of appointment-related costs). Costs for software/telecommunication for telerehabilitation were market rates from the providers (including Wellpepper Inc and eHAB). Patient costs of travel to and from appointments were estimated using distance travelled from the patient’s residence and cost per kilometre travelled values provided by the Australian Taxation Office for private vehicle use, or patient-reported public transport and taxi fares when these modalities were used. For the purpose of the sensitivity analysis, the cost of providing each participant in the telerehabilitation group with a tablet, protective case and data SIM card was calculated by dividing the total cost of procuring these devices from a local metropolitan supplier (which was also consistent with the device manufacturer recommended retail price) by the number of participants receiving telerehabilitation. This may be considered a high estimate of these costs, as future patients could have continued to use these devices and thereby reduced the per-person hardware cost estimate.
Incremental cost-effectiveness (cost-utility) analysis
The primary analysis used an Incremental Cost-Effectiveness Ratio (ICER) to compare the cost per QALY accrued in the telerehabilitation group versus in-person using costs and effects data from the randomised trial.
The ICER equation was:

The difference in cost was estimated using the regression coefficient for group allocation (with cost as the outcome variable). Similarly, difference in QALYs was estimated using the regression coefficient for group allocation (with QALYs as the outcome variable). To quantify uncertainty in these estimates, bootstrap resampling (2000 replications) was used to calculate 95% confidence intervals (for between-group differences in costs and QALYs), as well as a 95% confidence ellipse for ICER (cost per QALY). A sensitivity analysis was also conducted whereby the cost perspective was not limited to the health service provider, but also inclusive of patient costs associated with travel to the hospital for in-person sessions as well as per-person cost for the tablet, protective case with data SIM card for internet access for telerehabilitation sessions. The same regression analysis approach as the primary analysis, including bootstrap resampling was used to examine whether cost-effectiveness findings were robust against the decision not to include this broader perspective of costs in the primary analysis.
Incremental cost-effectiveness (patient rehabilitation time per QALY gained)
A novel secondary analysis was conducted whereby the time accrued by patients attending rehabilitation sessions (including travel time) was considered the ‘cost’ (i.e. a time burden), rather than cost from the health service perspective. For this secondary analysis, the ICER was:
Estimates were generated in the same way as the primary analysis (including regression analyses with bootstrap resampling), with patient time cost (measured in minutes, expressed in hours) was used in this secondary analysis. Because there was also third-party burden, associated with carer time spent supporting patients to participate in the rehabilitation interventions, a sensitivity analysis for this secondary analysis was undertaken that repeated the aforementioned secondary analysis, but included carer time in addition to patient time in the time cost components of the equation.
Results
Resource use and costs
For participants in the telerehabilitation group, the per-person cost of eHAB and Wellpepper subscriptions for the entire 6-week intervention were $30 and $36.67, respectively. The mean number of appointments attended, healthcare costs, patient time, carer time and patient travel costs are presented in Table 1, with 95% bias-corrected confidence intervals for each group. Despite the aforementioned subscription costs for the telerehabilitation group, a slightly higher point estimate for the mean total healthcare cost was observed for the in-person group ($516.12) versus the telerehabilitation group ($487.22); however, the 95% confidence intervals for these values were overlapping. The driver for the slightly higher point estimate of mean cost for the in-person group originated from the small difference (0.4 sessions) in the mean physiotherapy appointments attended for each respective group. The cost for the tablet (iPad), protective case, and data SIM card purchase for each person was recorded at $89.43 within the trial. Patients in the in-person group spent a significantly greater amount of time attending physiotherapy appointments (including travel) and also accrued significantly greater out-of-pocket costs associated with this travel (Table 1).
Summary of mean (95% confidence intervals – bootstrapped bias corrected) per-person healthcare resource use and costs as well as travel time and travel costs.
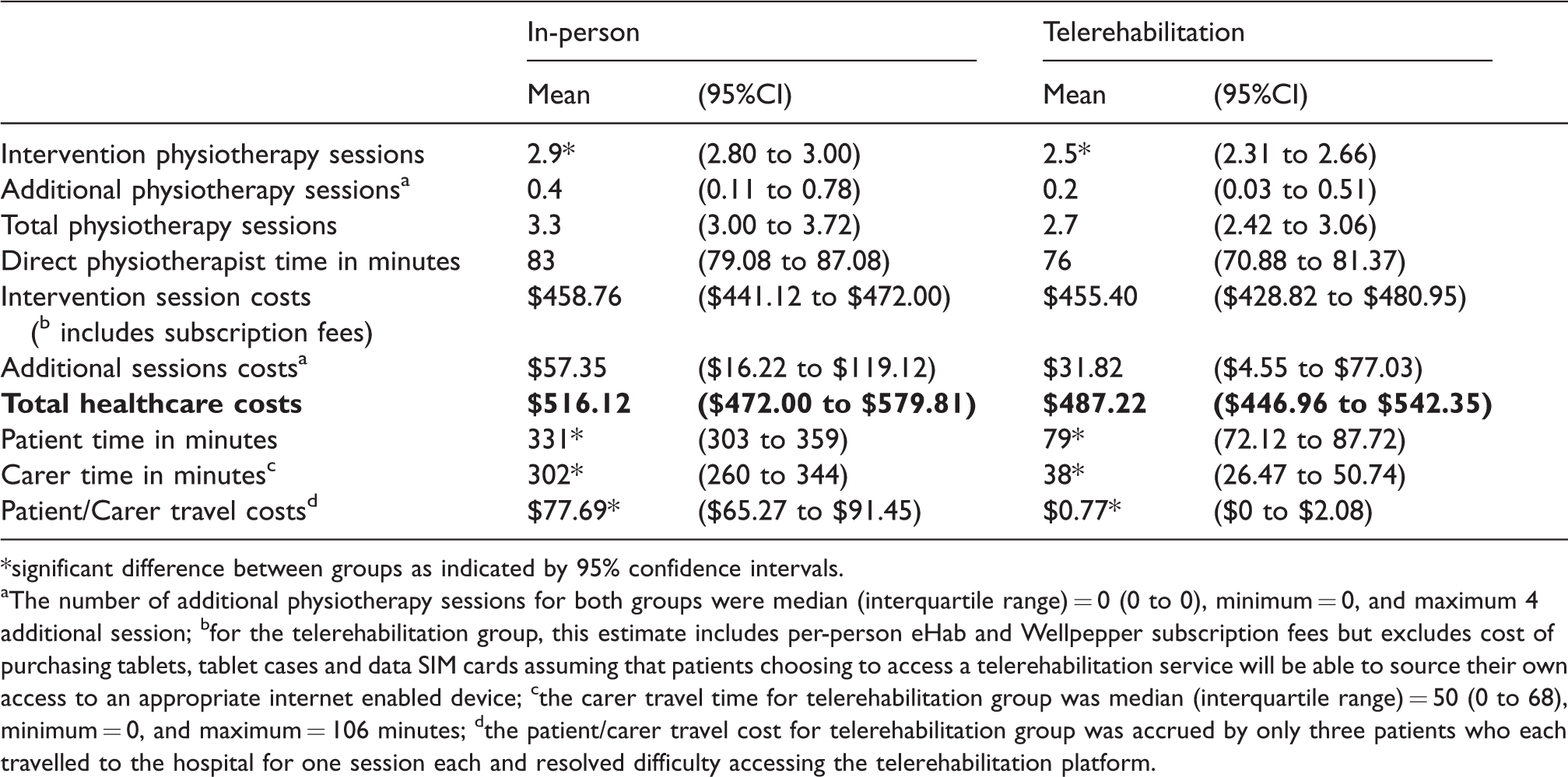
*significant difference between groups as indicated by 95% confidence intervals.
aThe number of additional physiotherapy sessions for both groups were median (interquartile range) = 0 (0 to 0), minimum = 0, and maximum 4 additional session; bfor the telerehabilitation group, this estimate includes per-person eHab and Wellpepper subscription fees but excludes cost of purchasing tablets, tablet cases and data SIM cards assuming that patients choosing to access a telerehabilitation service will be able to source their own access to an appropriate internet enabled device; cthe carer travel time for telerehabilitation group was median (interquartile range) = 50 (0 to 68), minimum = 0, and maximum = 106 minutes; dthe patient/carer travel cost for telerehabilitation group was accrued by only three patients who each travelled to the hospital for one session each and resolved difficulty accessing the telerehabilitation platform.
Multi-attribute utility and QALYs
The mean estimate of the in-person rehabilitation group multi-attribute utility score profile at baseline was slightly higher than the telerehabilitation group, but confidence intervals overlapped (in-person mean (95%CI) = 0.46, (0.39 to 0.53); telerehabilitation mean (95%CI) = 0.39 (0.30 to 0.48)). Both groups experienced substantial improvement by the 6-week assessment (in-person mean (95%CI) = 0.85, (0.81 to 0.88); telerehabilitation mean (95%CI) = 0.83 (0.78 to 0.87)) and 26-week assessment (in-person mean (95%CI) = 0.89, (0.84 to 0.92); telerehabilitation mean (95%CI) = 0.88 (0.85 to 0.92)), with no indication of meaningful between-group differences at these re-assessments. Consequently, the mean accrued 6-month QALY estimates were similar for each group (in-person mean (95%CI) = 0.41, (0.39 to 0.42); telerehabilitation mean (95%CI) = 0.40 (0.38 to 0.42)).
Primary and primary sensitivity (cost-utility) ICER estimates
There was no significant between-group differences in rehabilitation healthcare costs or QALYs gained. The small estimated mean (95%CI) difference in cost of telerehabilitation versus in-person was –$28.90 (–$96.37 to $40.45), favouring the telerehabilitation group. The small estimated mean (95%CI) difference in QALYs gained from telerehabilitation versus in-person was –0.0025 (–0.0227 to 0.0217). Consequently, although the ICER point estimate may be equated to indicate that in-person rehabilitation cost an additional $11560 per QALY gained versus telerehabilitation, this should be interpreted with extreme caution owing to the negligible mean differences (particularly in QALY) from which this ICER was derived. The cost-effectiveness of telerehabilitation versus in-person rehabilitation is better illustrated by the cost per QALY estimates and 95% confidence ellipse derived from the bootstrap resampling presented in Figure 2(a). In summary, the estimates were close to the origin ($0, 0 QALY) with the 95% confidence ellipse overlapping into all four quadrants on the cost-effectiveness plane. This indicates that neither intervention is clearly favoured when it comes to incremental cost-effectiveness (cost-utility) analysis with costs derived from the perspective of the health service. Findings from the sensitivity analysis with the broader perspective of costs were consistent with the primary analysis (Figure 2(b)). The estimates were also close to the origin ($0, 0 QALY) and with the 95% confidence ellipse overlapping into all four quadrants on the cost-effectiveness plane, again indicating that neither intervention is clearly favoured when it comes to incremental cost-effectiveness even with the broader perspective of costs in this sensitivity analysis.

Cost-effectiveness (cost-utility) estimates with 95% confidence ellipse for the (a) primary cost-utility analysis and (b) sensitivity analysis with a broader cost perspective including patient technology and travel costs.
Secondary and secondary sensitivity (time burden-utility) ICER estimates
The estimated mean (95%CI) difference in time burden for patients to participate in rehabilitation sessions via telerehabilitation versus in-person was –4.21 (–4.69 to –3.74) hours, favouring less time burden for the telerehabilitation group. The incremental (lower) patient time burden per QALY estimate and 95% confidence ellipse derived from the bootstrap resampling is presented in Figure 3(a). The 95% confidence ellipse was positioned almost equally across the two bottom quadrants on the cost-effectiveness plane. This indicates a high degree of certainty that there is a lower patient time burden associated with telerehabilitation (and no indication of significant between-group difference in QALYs). The 95% confident ellipse from the sensitivity analysis was positioned even lower across the bottom two quadrants on the cost-effectiveness plane than the primary analysis. This indicates that when carer time burden is considered in addition to patient time burden, then the extent to which telerehabilitation was associated with lower time burden was extenuated (Figure 3(b)). The estimated mean (95%CI) difference in combined patient and carer time burden associated with telerehabilitation versus in-person rehabilitation was –8.6 (–9.69 to –7.54) hours.
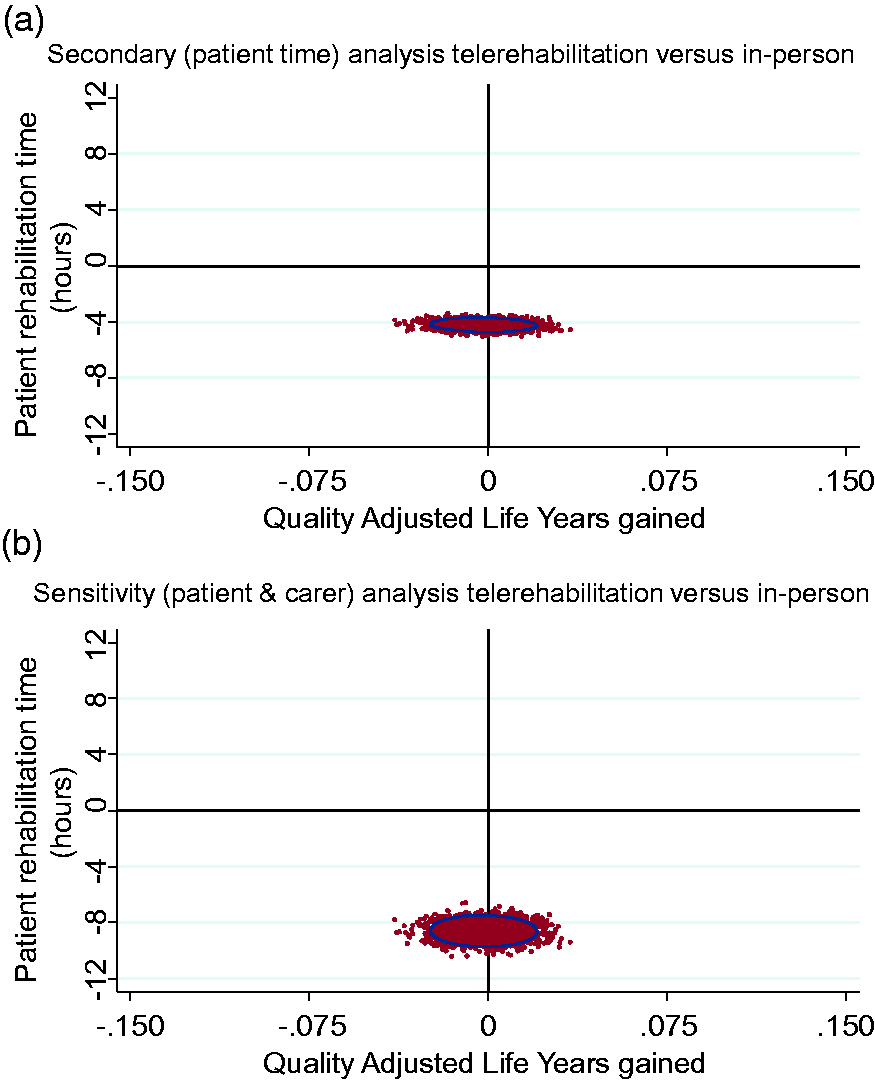
Secondary analyses of rehabilitation session-related time burden and effect (QALY) estimates with 95% confidence ellipse for the (a) secondary analysis of patient time burden and (b) a sensitivity analysis that included both patient and carer time burden.
Discussion
This study was the first to explore the cost-effectiveness of in-person care compared with telerehabilitation following THR. No significant between-group differences were detected in total healthcare cost or QALYs gained. These findings are consistent with economic evaluations in the total knee replacement population that have indicated telerehabilitation is an economically viable alternative to traditional in-person care for post-joint-arthroplasty rehabilitation.18,19 Nonetheless, some key differences should be noted.
This was the first study to report cost-effectiveness for post-joint replacement telerehabilitation intervention, with prior studies either focussing solely on costs 18 without consideration of effect, or investigating a mixed intervention with an equal split of in-person and telerehabilitation intervention sessions. 19 Furthermore, participants in the present study received a total of approximately three physiotherapy sessions (mean sessions: telerehabilitation 2.7; in-person 3.3). This reflects current practice in Australia wherein patients receive three to four outpatient physiotherapy sessions following discharge from hospital. 21 This differs considerably from the 16 sessions provided by Tousignant et al. 18 and the 20 sessions provided by Fusco and Turchetti. 19 A greater number of sessions per person reduces the per-session cost of technology-related expenses, and is therefore more likely to yield a cost-result in favour of telerehabilitation. In addition, in the present study, patients assigned to the in-person group were responsible for their own travel to the hospital, which is common practice in many regions internationally. This is in contrast to domiciliary rehabilitation delivery 18 or ambulance transportation 19 in the aforementioned studies.
The present study also had some novelty in considering patient and carer time as a natural unit of cost in a secondary (time-utility) analysis that revealed significantly lower patient and carer time burden with telerehabilitation (with no significant difference in patient outcome). This is an important finding in the context of modern healthcare systems adopting patient-centred models. The significant reduction in time burden associated with telerehabilitation could arguably enhance patient satisfaction and compliance rates with rehabilitation programmes. This is perhaps supported by significantly higher levels of patient satisfaction being reported in the telerehabilitation group (p = 0.017) for the item “my therapy session was easy to attend” during the randomised trial from which this economic evaluation was derived. 15 In addition, the telerehabilitation group participants were more compliant with their home exercise programme, with an overall compliance of 86% (SD 20%) compared with 74% (SD 26%) for the in-person group (mean difference 12% (95% CI 0.5%–23%)) in the trial. However, it is noteworthy that a causal relationship between reduced time burden and increased compliance cannot be assumed without further investigation.
There are at least three important factors which support the generalisability of our results. First, our rehabilitation model was based on current practice as defined by Nelson et al. 21 Second, patients were responsible for their own travel arrangements to attend hospital-based appointments (consistent with usual practice in Australian and many other healthcare settings internationally). Third, the technology used is widely available (iPads and accessible software subscriptions), making it feasible to deploy similar models of care without large up-front costs to healthcare providers.
The limitations of this study need acknowledgement. All telerehabilitation sessions were conducted by the same physiotherapist who was familiar with the technology. Physiotherapists new to telerehabilitation may not have produced comparable findings. For the sensitivity analysis, the cost of providing telerehabilitation participants with the required technology was calculated by dividing the total technology cost by the number of telerehabilitation participants. This may be considered a high estimate of these costs, as future patients could have continued to use these devices and thereby reduced the per-person hardware cost estimate.
In conclusion, telerehabilitation in the THR population incurred similar costs and yielded similar effects to traditional in-person care. Telerehabilitation significantly reduced the time burden for patients and carers participating in rehabilitation. These findings are valuable for healthcare providers seeking to implement accessible patient-centred rehabilitation services.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.