
Abstract
The American College of Emergency Physicians Emergency Telehealth Section was charged with development of a working definition of emergency telehealth that aligns with the College’s definition of emergency medicine. A modified Delphi method was used by the section membership who represented telehealth providers in both private and public health-care delivery systems, academia and industry, rural and urban settings. Presented in this manuscript is the final definition of emergency telehealth developed with an additional six clarifying statements to address the context of the definition. Emergency telehealth is a core domain of emergency medicine and is inclusive of remotely providing all types of care for acute conditions of any kind requiring expeditious care irrespective of any prior relationship. The development of this definition is important to the global community of emergency physicians and all patients seeking acute care to ensure that appropriately trained clinicians are providing the highest quality of emergency services via the telehealth modality. We recommend implementing emergency telehealth in a manner that ensures appropriate qualifications of providers, appropriate/parity reimbursement for telehealth services and, most importantly, the delivery of quality care to patients in a safe, efficient, timely and cost-effective manner.
Introduction
In 2016, the American College of Emergency Physicians (ACEP) Emergency Telehealth Section was awarded an ACEP Section Grant to develop a telehealth-focused practice guideline document with a number of specific goals. Our primary goal is to develop a working definition of emergency telehealth that appropriately aligns with the ACEP definition of emergency medicine.
ACEP promotes high-quality emergency care and advocates for emergency physicians and their roles in patient care and public health. 1 , 2 In a statement of values, ACEP encourages emergency physicians to take responsibility and leadership in improving the quality of emergency care. 1 , 2 Emerging technologies, and specifically telehealth, are rapidly impacting emergency physicians and their patients, providing access, empowering health literacy and improving convenience.
Telehealth – the use of telecommunications technologies to communicate and facilitate health-related services between two remote parties – is typically used in health care between provider and patient or between two health-care providers. 3 This modality can serve as a vehicle to enable the delivery of high-quality, cost-effective, convenient and efficient health care to patients while providing access to health services from nearly any location. 4 Telehealth can improve the quality of care delivered by supplementing available services or providing care that may otherwise be unavailable due to time, distance or resource limitations.
The words ‘telemedicine’ and ‘telehealth’ are traditionally used interchangeably and are linked to terms such as tele-emergency medicine, tele-psychiatry, tele-dermatology, telestroke and so on to refer to specific telehealth services. 5 While these terms indicate a clinical specialty or discipline, they all fall under the umbrella of telemedicine or telehealth. The term ‘telemedicine’ implies remotely providing a health-care service when there is a sick or injured patient. 6 The term ‘telehealth’ is broader and more inclusive, encompassing screening, prevention, maintenance, follow-up services, health-related education, public health and health administration. 3 , 5 We use telehealth broadly to describe all specialties and services related to health care delivered via telecommunications technologies.
Caring for patients remotely is valuable in a variety of settings, including acute unscheduled and emergency care, inpatient settings and disaster response. Telehealth has been used for decades, facilitating care for millions of patient encounters. Common examples include teleradiology, telestroke, tele-psychiatry and teletrauma. The advent of low-cost, high-bandwidth data transmission has introduced a host of new applications and democratised access to care. New applications such as direct to consumer services show promise but lack rigorous studies of outcome and cost-effectiveness. Although telehealth offers many opportunities and much potential, patients, providers and payers demand evidence to facilitate further development of the field.
ACEP defines emergency medicine as a medical specialty with a focus on the diagnosis and treatment of acute, undifferentiated illness or injury and all components required to provide that care. The ACEP definition clearly states ‘Emergency medicine is not defined by location but may be practiced in a variety of clinical settings … [including] telemedicine’. 7
According to a survey conducted by the Telehealth Section in 2012, emergency physicians work in telehealth providing direct clinical services, remote supervision, remote monitoring, remote diagnostic testing, care coordination and teaching and education. Given this broad adoption of telehealth among emergency physicians, the ACEP Emergency Telehealth Section determined that there was importance and urgency to define emergency telehealth better.
Developing a definition for emergency telehealth
We conducted a modified Delphi process in six rounds consistent with the method described by Hsu and Sandford. 8 Participants were asked to volunteer from the membership of the ACEP Emergency Telehealth Section. All contributors are board-certified emergency physicians and fellows of ACEP. The group also includes members of the American Telemedicine Association and medical directors, executives and founders of telemedicine services. The participants (N=10) represented both private and public health-care delivery systems, academia and industry, rural and urban settings and practiced various types of telemedicine, including direct to consumer, provider to provider and remote consultation services.
In the initial round, participants were asked to ‘define emergency telemedicine’ in an open-ended fashion. Following the initial round of voting, answers were consolidated and summarised. With each subsequent round, alternatives were eliminated or consolidated. Only one definition remained for the final rounds and efforts focused on generating inclusivity and consensus. Once consensus on content was reached, the group continued edits for clarity. The final definition is presented below.
Emergency telehealth definition
Emergency telehealth is remotely caring for acute illness, injury and exacerbations of chronic diseases, including the initial evaluation, diagnosis, treatment, prevention, coordination of care, disposition and public-health impact of any patient requiring expeditious care, irrespective of any prior relationship. Emergency physicians are uniquely qualified to leverage emergency telehealth, unscheduled or scheduled, to provide medical care across the spectrum of conditions and severity.
The ACEP Emergency Telehealth Section believes the context for the definition of emergency telehealth currently includes the following (1 August 2018):
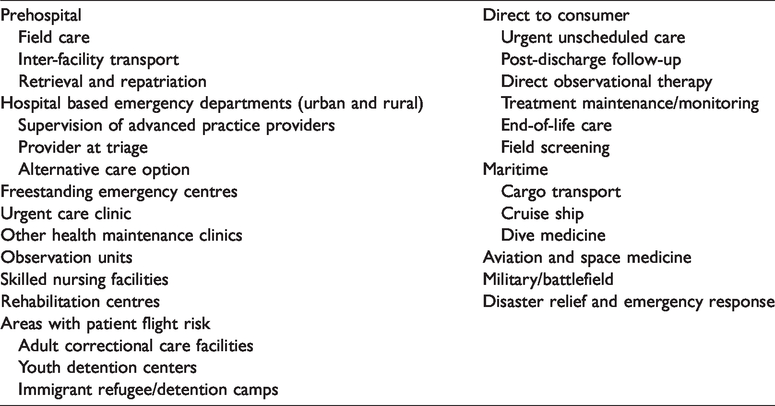
A provider’s training, expertise, capabilities, capacity, certification and credentialing dictate the quality and range of services offered through telehealth. Emergency telehealth may be utilised by or in consultation with a board-certified/eligible emergency physician. Emergency physicians use a variety of technologies safely, effectively and within existing regulatory, quality and confidentiality frameworks to deliver emergency medical care and address access to care, care efficiency, diagnostic interpretations, clinical interventions, monitoring and transitions of care. Emergency telehealth may be conducted in a variety of settings that include, but are not limited to, urban and rural hospital and freestanding emergency departments, urgent care clinics, observation medicine units, correctional care facilities, out-of-hospital settings, including the home, skilled nursing facilities, rehabilitation centres, during medical transport, emergency medical services at the scene of illness or injury or in the community, at disaster sites, as well as austere environments such as maritime, aviation, space and military uses in and out of theatre. Emergency physicians should use evidence-based medicine and guidelines to deliver emergency telehealth effectively. Emergency telehealth providers should participate in building the base of evidence regarding emergency telehealth. The ACEP Emergency Telehealth Section believes that the prudent layperson standard, defined in the Balanced Budget Act (BBA) of 1997, applies to EMTALA mandated care, regardless of whether care is delivered in person or through emergency telehealth, and that both in-person and emergency telehealth may be used to satisfy EMTALA screening obligations as dictated by local hospital/medical staff policies.
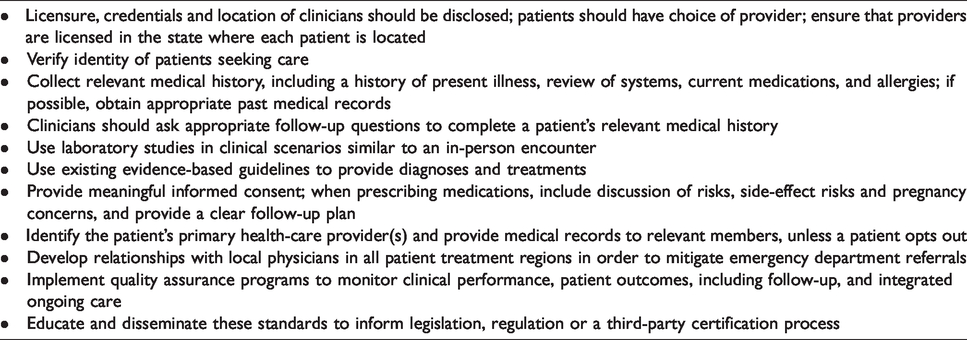
We recommend implementing emergency telehealth in a manner that ensures appropriate qualifications of providers, appropriate/parity reimbursement for telehealth services and, most importantly, the delivery of quality care to patients in a safe, efficient, timely and cost-effective manner. We outline the application of emergency telehealth in Table 1 and minimum standards for telehealth practice in Table 2. The future application and expansion of telehealth into emergency medicine has the potential to help emergency providers care for anyone, with any concern, at any time.
Emergency telehealth applications.
Recommended minimum standards for telehealth practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by a Section Grant from the American College of Emergency Physicians.
ORCID iDs
Neal Sikka https://orcid.org/0000-0002-4696-6922
Aditi U Joshi ![]()