
Abstract
Introduction
Evidence of telehealth for chronic disease management is scarce and contradictory.
Objectives
We aimed to evaluate the safety and efficacy of teleconsultations as support in the care transition of patients with stable coronary artery disease (CAD) from tertiary to primary care.
Methods
A randomized noninferiority clinical trial was undertaken in patients with CAD from a tertiary hospital in a middle-income country. Patients with functional angina class 1 or 2 and meeting discharge criteria were randomized to remain in the cardiology outpatient clinic for 12 months (control group, CG) or continue follow-up in a primary care unit with clinical support via telemedicine (intervention group, IG). The primary outcome was the maintenance of the functional angina class after 12 months. Secondary outcomes included control of risk factors and clinical outcomes.
Results
In total 271 patients (mean age, 66 years) were included; 81.1% and 91% of the IG and CG, respectively, maintained stable angina symptoms, thus noninferiority could not be shown between the groups. Regarding emergency room visits at 1 year, the IG (7.6%) was noninferior to the CG (6.0%) (absolute difference, 1.6%; noninferiority margin (NIM), –4.8% to 8.2%). For control of risk factors, 30.7% and 29.6% of the IG and CG, respectively, had blood pressure <130/80 mmHg (absolute difference, 1.1%; NIM, –10.5% to 12.8%), and 48.9% and 33.3% of diabetic patients in the IG and CG, respectively, had glycated haemoglobin <7% (absolute difference, 15.6%; NIM, –6.8% to 36%).
Conclusions
In our study, the difference in the patients’ angina functional class did not result in greater seeking of emergency care, supporting that discharge from the outpatient clinic with telemedicine is safe for patients with stable CAD treated at the tertiary level. The control of risk factors in these patients was noninferior to patients followed up in primary care. ClinicalTrials.gov (NCT02489565).
Introduction
Coronary artery disease (CAD) remains one of the major diseases of the 21st century because of its high morbidity and mortality. 1 According to the World Health Organization, more than three-quarters of deaths from cardiovascular diseases occur in low- and middle-income countries. 2 In Brazil, CAD is one of the main causes of death and is also a source of large healthcare expenditures. 3
Many patients with CAD are stable for long periods of time, requiring only control of risk factors and reassessment of prescribed medications. These services can be provided in primary care and referred to tertiary care when the condition becomes unstable. However, the Brazilian healthcare network is characterized by heterogeneity among hospital complexes with regard to the incorporation of technology and the complexity of services, with a concentration of financial and personnel resources in large cities, resulting in regional imbalances. 4 Within this context, high-complexity specialized outpatient clinics face overcrowding and restricted access, with many of those patients being from distant cities who could be followed up at their place of residence.
Within the current epidemiological and economic context of Brazil and the world, advances in telehealth actions have modified modern medicine in a scenario where distance and resource inequality are critical factors. Currently in the United States, it is estimated that more than 60% of all health institutions and 40–50% of all hospitals employ some form of telehealth. 5 One of the telehealth formats for conducting healthcare support and permanent health education activities is teleconsultation. Teleconsultations are registered consultations conducted among workers, professionals and managers in the health field through telecommunication tools with the objective of answering questions about clinical procedures, health actions and issues related to the work process. 6
Studies have shown that care support via telehealth is able to reduce the number of exams and requests for referrals to other care levels. 7 However, the evidence base for telehealth in the management of chronic diseases is generally weak and contradictory. In the context of CAD, there is evidence of improvement in the profile of risk factors with the aid of telehealth; 8 however, actions aimed at reducing unfavourable outcomes remain underexplored, especially when the communication between interlocutors occurs in real time.
Considering the context of developing countries and the experience with telehealth in the Brazilian scenario, we conducted a noninferiority study to evaluate the safety and efficacy of using teleconsultations in the transition from tertiary care to primary care in patients with stable CAD.
Methods
Design and eligibility
This was a randomized noninferiority clinical trial that compared two groups of patients with CAD who met clinical criteria for outpatient discharge at a tertiary hospital in the South of Brazil. One group was randomized to follow-up in primary care with telehealth clinical support (intervention group, IG), and another group continued routine outpatient follow-up (annual follow-up) in the specialized outpatient clinic of the hospital (control group, CG). The study methodology was previously published. 9 The study is registered in the international registry ClinicalTrials.gov under number NCT02489565.
Patients of both sexes, aged 18 years or older, diagnosed with CAD class I or II angina according to the Canadian Cardiovascular Society Classification (CCSC) at the time of randomization were included. To be able to be discharged from the specialized outpatient clinic, the patients were clinically stable, without a cardiovascular event and decompensated clinical condition in the past year. The inclusion period was from May 2014 to November 2016, and the patients were followed up for 1 year after discharge.
Patients eligible for inclusion were randomized 1:1 using random block sizes of six and four, by a computerized list provided by randomization.com. Group assignment was performed by opening a sealed opaque envelope in front of the patient after she or he signed an informed consent form and completed the initial research questionnaire. After that, the groups were managed as shown in Figure 1.
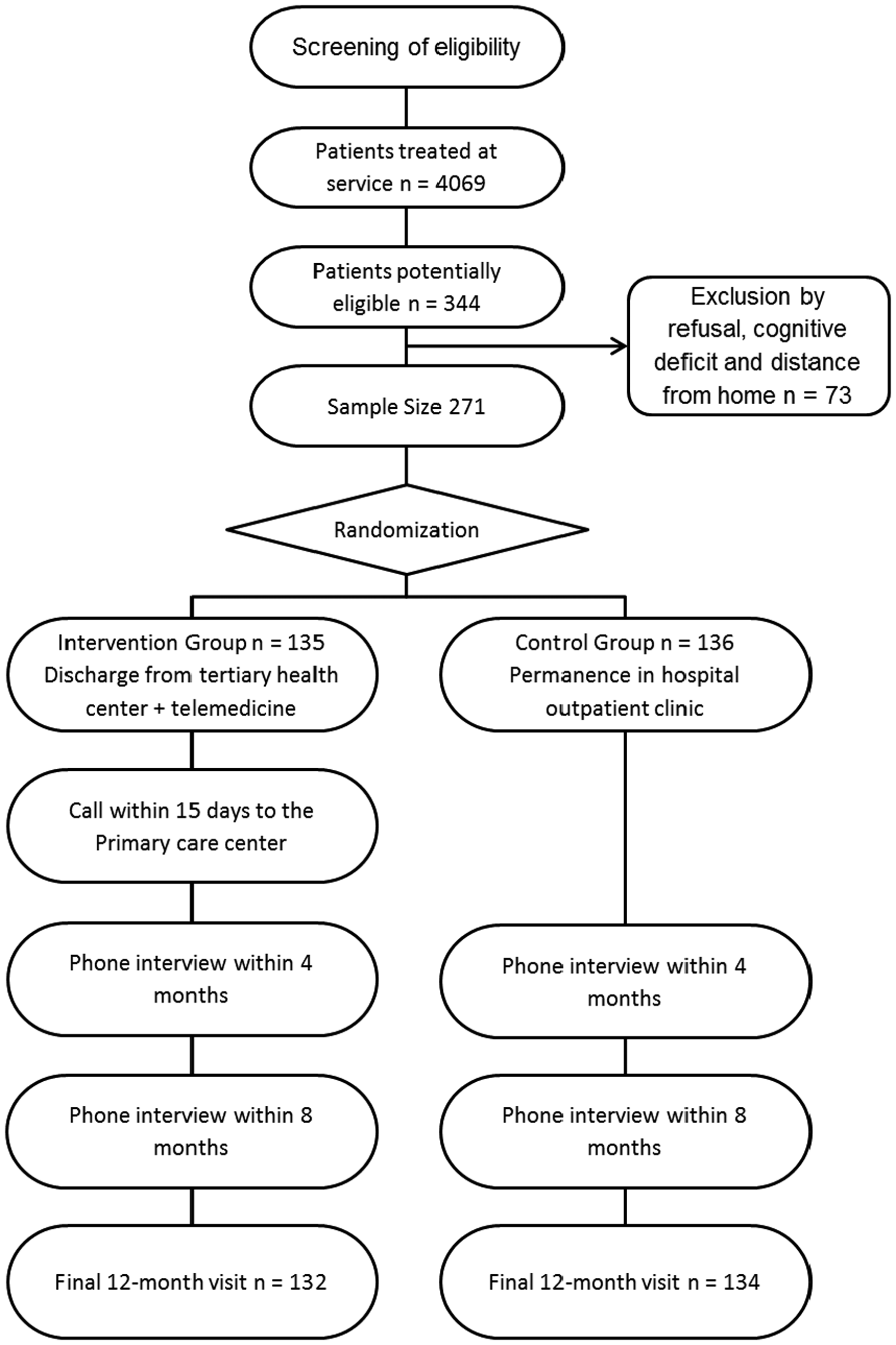
Flowchart of the eligibility and randomization process used for the study.
Intervention
The intervention analysed was discharge from the specialized outpatient clinic at the tertiary care hospital with counter-referral to the family health centre closest to the patient’s residence and with clinical support via the State’s telemedicine platform (TelessaúdeRS-UFRGS), using an information and communication technology tool (teleconsultation), accompanied by a guarantee of return to the outpatient clinic in case of disease exacerbation with disease management by consulting physicians. The TelessaúdeRS team included a specialized cardiologist with access to the patients’ outpatient discharge records and who was available to primary care physicians from Monday to Friday from 8:00 am to 5:30 pm via a toll-free line. The TelessaúdeRS group contacted the health centres within 1 month after discharge to determine whether the patient had contacted the primary care centre.
Patients were interviewed by telephone at 4 and 8 months of follow-up using the standardized instrument applied at the entry to the study. The calls were made by independent evaluators, hired and trained specifically for this purpose. An in-person visit focusing on the evaluation of symptoms, disease decompensation episodes and treatment adherence was made for both groups 12 months after randomization.
If the patient remained clinically stable, she or he continued follow-up in primary care or received an effective discharge from the tertiary clinic.
Outcomes
The primary outcome analysed was the permanence in CCSC class I or II after 1 year of follow-up.
The secondary outcomes analysed were control of risk factors (blood pressure <130/80 mmHg; low-density lipoprotein (LDL) <100 mg/dl; glycated haemoglobin (HbA1) <7% for patients with diabetes; smoking cessation if a smoker; and regular physical activity of 150 minutes/week); access to the health system; occurrence of disease instability within 1 year (emergency visit due to acute coronary syndrome, chest pain, decompensated heart failure (HF), acute arrhythmias and stroke); and rate of patients in the IG who sought medical consultations in primary care within 6 months of the referral.
Sample size calculation and data analysis
The sample size was calculated as 140 patients in each group, considering a noninferiority margin of 10% and incidence of 92% of the main outcome, that is, maintenance of CCSC 12 months after the start of follow-up. An additional 10% margin was added to account for losses to follow-up. This was based on the rate of patients with an increase in angina to a higher CCSC reported by a previous study for a control group receiving optimal treatment for CAD. 10 For calculation of the sample size, a ß of 0.9 and an α of 0.05 (two-sided) were considered.
We assessed the main outcome by subtracting the prevalence of controlled symptoms by the end of follow-up between the IG and CG and calculating the 95% confidence intervals. If the lower bound of the confidence interval reached the noninferiority margin (10% absolute difference), experimental treatment would be considered not noninferior to the CG. The same procedures were followed for secondary outcomes. Patients who presented incomplete data at the end of follow-up were excluded from the analysis for the corresponding outcomes. The confidence intervals were estimated using the Miettinen–Nurminen method. 11 The analyses were performed in the PASW Statistics v.18.0 and SAS Studio software environment.
Ethics approval and consent to participate
Ethics approval was obtained from an institutional review board (CAAE: 28064614.0.0000.5327). All participants were extensively informed about the study, including confidentiality aspects and the right to withdraw from the study at any time, without providing an explanation and with no effect on the quality of treatment.
Results
First inclusion was performed in May 2014, and the last inclusion was performed in November 2016; the last follow-up visit was performed in November 2017. Overall, 344 patients were assessed for eligibility. From those, 271 fulfilled the inclusion criteria and were randomized. The inclusion period was stopped earlier since losses to follow-up were less than 10%. Patient flow is depicted in the flowchart in Figure 1. Included patient characteristics were similar between groups and are presented in Table 1. The mean age was 66.6 years, and most patients were male; approximately 75% of the patients had angina only for strenuous or rapid or prolonged exertion. Almost all patients were on statins, antiplatelet agents and beta-blockers.
Baseline demographics and clinical characteristics of the study population (N=271).
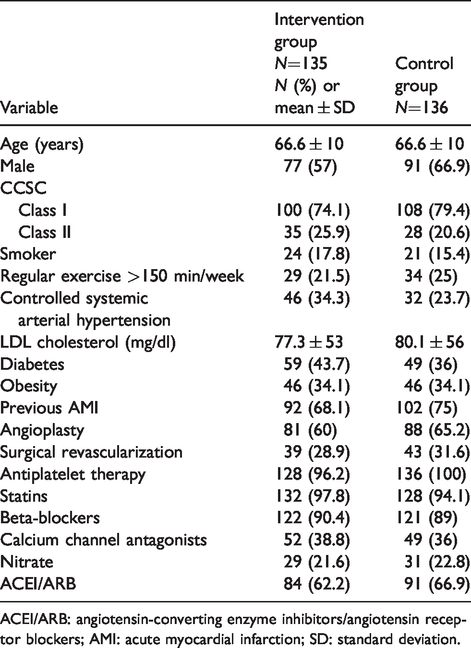
ACEI/ARB: angiotensin-converting enzyme inhibitors/angiotensin receptor blockers; AMI: acute myocardial infarction; SD: standard deviation.
Five patients did not complete the follow-up evaluation due to death (three in IG and two in CG) and were not included in the main analysis due to lack of symptom information; one patient was restricted to a wheelchair, and no other exclusions for the main outcome occurred.
For the main outcome, maintenance of CCSC I or II, 81.1% of the patients in the IG and 91.0% of patients in the CG had stable symptoms. The absolute difference was –9.9% (95% CI –18.5 to –1.6%). The noninferiority margin was surpassed, and noninferiority could not be shown.
The intervention group was noninferior to the control group with a lower number of emergency visits, diabetes control, no smoking and exercise >150 min per week. For the remainder of the secondary outcomes, noninferiority was not shown, but inferiority was not identified. The results are shown in Table 2.
Primary and secondary outcomes at 1 year of follow-up – noninferiority analysis.
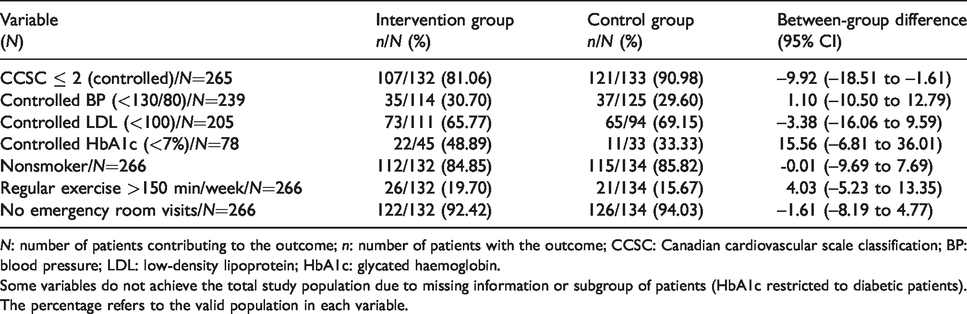
N: number of patients contributing to the outcome; n: number of patients with the outcome; CCSC: Canadian cardiovascular scale classification; BP: blood pressure; LDL: low-density lipoprotein; HbA1c: glycated haemoglobin.
Some variables do not achieve the total study population due to missing information or subgroup of patients (HbA1c restricted to diabetic patients). The percentage refers to the valid population in each variable.
Regarding access to primary care, 57 (43.2%) patients in the IG did not seek a primary care consultation within 6 months of the referral.
Discussion
In this clinical trial, we observed a higher proportion of patients with stable symptoms when managed in high-complexity outpatient care compared with patients followed up in primary care, and it was not possible to define it as noninferior to the strategy of care in primary health units with telemedicine support. This finding may be explained by the fact that this is a subjectively assessed outcome, in which the perception of symptoms by the patient may have been affected by the safety of care in a tertiary hospital, as well as by the evidence that a large part of the patients in the IG referred to primary care did not seek a medical consultation within 6 months of follow-up. However, the difference in the patients’ angina functional class did not result in greater seeking of emergency care, an objective indicator of clinical worsening.
In contrast, the strategy of discharge with telemedicine support was found to be noninferior in the control of diabetes, smoking cessation and physical activity after 1 year of follow-up. These data support the efficacy of primary care in controlling risk factors of patients with chronic diseases. In a previous investigation with TelessaúdeRS/UFRGS, more than 50,000 clinical consultations were registered between 2010 and 2016, involving approximately 15,000 healthcare professionals through teleconsultations and telediagnosis and tele-education activities. Approximately 66% of primary care physicians who wanted to refer patients to tertiary care changed their minds after a discussion with the teleconsulting physician. Despite the structural limitations of Brazilian primary care, telemedicine is potentially useful for improving the quality of care and streamlining the flow between different care levels, avoiding unnecessary trips and biased access to the system. 12
In the literature, evidence for the efficacy of telehealth in the management of patients with chronic diseases is heterogeneous. In a review published in 2012 on the use of telemedicine in the last two decades, 141 randomized clinical trials were selected, with a total of 37,695 patients, that evaluated different telehealth actions (telemonitoring, telephone support, videoconferencing, email, web messaging or online chat) in the follow-up of five chronic conditions (chronic obstructive pulmonary disease, asthma, systemic arterial hypertension, diabetes mellitus and congestive HF). The results of the reviewed studies had high variability, and it was not possible to determine if telehealth strategies, as a single group, are effective for patient management. 13
In a systematic review by Cochrane that included 27 studies, when only patients with HF were evaluated, patients followed up with structured telephone support had a 13% lower chance of mortality from all causes (data from 9222 patients) and a 15% lower chance of hospitalizations related to HF (data from 7030 patients) when compared with patients who did not receive teleconsultation support. In our study, the hard outcome evaluated was the need for emergency visits, demonstrating that follow-up of patients with chronic CAD in primary care was noninferior; however, mortality and other major cardiac events were not assessed. 14
In Brazil, the structure of patient referral to various care levels in the public health system (SUS) occurs through a referral and counter-referral system, a fundamental point to ensure the accessibility, universality, and comprehensiveness of care. However, access to tertiary care levels, especially for consultations with specialists or for complementary exams not available in primary care, is, in large part, extremely difficult and time-consuming. 15 In addition, the current healthcare network is characterized by heterogeneity among hospital complexes with respect to the incorporation of technologies and service complexity, with a concentration of financial and personnel resources in large cities resulting in regional imbalances. Given this context, high-complexity specialized outpatient clinics face overcrowding and restricted access, with many patients of those being patients from distant cities who could be followed up at their place of residence. 4
Some limitations of our study must be addressed. This was a randomized trial of one outpatient clinic in Brazil, and therefore may not be representative of other referral institutions, although health care delivered was based on contemporary national guidelines for the public health system. The control of risk factors was suboptimal in a significant proportion of patients, mainly because of the difficulty of access to free medicines and low patients’ adherence. However, these factors were similarly challenging for both groups. In addition, complete follow-up was not achieved for some secondary outcomes as some patients did not manage to return to the hospital (research centre) for final evaluation. These patients were evenly distributed in the groups.
Based on our results, discharge from the outpatient clinic with teleconsultation support for patients with stable chronic ischaemic heart disease treated at the tertiary level is safe. In addition, the control of risk factors was found to be noninferior for patients followed up in primary care. In practice, discharges increase the number of visits available at the specialized outpatient clinic for cardiac patients in a more severe health state and allow patients with stabilized disease comfort and easier access to safe follow-up at a location closer to their residence.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by a grant from the Brazilian Ministry of Science and Technology (MCTI/CNPq/MS - SCTIE/DECIT Grant/Funding Number: 401463/2013–3) and Hospital de Clínicas de Porto Alegre/UFRGS. Prof. Polanczyk holds a research scholarship from CNPq (#313041/2017-2). The study protocol was submitted to external peer review by the funding body in the process of obtaining funding.