
Abstract
Abstract
Introduction
The use of telemedicine in orthopaedics can provide high-quality orthopaedic services to patients in remote areas. Tele-orthopaedics is widely acknowledged for decreasing travel, time and cost, increasing accessibility and quality of care. In the absence of a comprehensive review on tele-orthopaedics applications and services, here, we systematically identify and classify the tele-orthopaedic applications and services, and provide an overview of the trends in the field.
Methods
In this study, a systematic mapping was conducted to answer six research questions, we searched the databases Scopus, PubMed, IEEE Digital Library and Web of Science up to 2019. Consequently, 77 papers were screened and selected on the basis of specific inclusion and exclusion criteria.
Results
We found that mobile-based teleconsultation was mostly asynchronous, while non-mobile teleconsultation was synchronous. The results showed that the physician–patient relationship was more common than other interactions, such as physician–physician and physician–robot interactions. In addition, more than half of the services provided by tele-orthopaedics have been used for orthopaedic diseases/traumas in which joint replacement and fracture reduction have been the most important orthopaedic procedures. It has been noted that more attention has been paid to tele-orthopaedics in developed countries such as the USA, Australia, Canada and Finland.
Discussion
Telemonitoring (teleconsultation and telemetry) and telesurgery (telerobotics and telementoring) were found to be the two major forms of tele-orthopaedics. Mobile phones were used asynchronously in most of the teleconsultations. The development of different applications may result in the use of multiple smartphones applications in real-time teleconsultation. The use of smartphones is expected to increase in the near future.
Introduction
Musculoskeletal conditions are prevalent, and their impacts are also pervasive. 1 There are many musculoskeletal conditions that require clinical care by health-care providers. Musculoskeletal conditions related to the muscles, bones, joints and tissues such as tendons and ligaments comprise more than 150 diagnoses that affect the locomotor system. The World Health Organization (WHO) reported the most common musculoskeletal conditions as osteoarthritis, osteoporosis, back and neck pain, bone fractures, injuries and rheumatoid arthritis. 2 According to the latest report from Global Burden of Disease (GBD) in 2017, musculoskeletal conditions make the highest contribution to global disability, while low back pain has remained the single leading cause of disability since 1990. 3 These conditions do not target a particular age, sex or region; they can affect anyone and were the leading cause of disability in four out of the six WHO regions in 2017. 2 Due to the widespread prevalence of musculoskeletal conditions and the lack of orthopaedic services available everywhere, people can benefit from the use of telecommunication technologies.
Health care is currently affected by information and communication technology (ICT). New forms of health, including telemedicine, telehealth and e-health, have facilitated the exchange of information between different parties and from patients to specialists. ICT has also increased accessibility and quality, productivity, efficacy and effectiveness of health care, and has reduced the costs in many areas of health care. 4 It is an important component of e-health, including hardware, software, networks and media for data collection, storage, processing, transmission and presentation (video, audio, image and text data) of related services for prevention, diagnostics, treatment, monitoring, educational and management purposes remotely.5–7
As an important part of telehealth, telemedicine focuses mainly on providing care services by health-care specialists 8 and does not include prevention and improvement aspects of health care, education and management services. 9 Telemedicine is often used for follow-ups, chronic disease management, drug management, specialised consultation and some clinical services through secure remote audio/video communication. 10
Telehealth is a newer and more general concept for telemedicine. Unlike telemedicine, telehealth has educational, research and managerial uses that benefit a wide range of health-care providers, including nurses, psychologists, managers and non-physicians. 11 Telehealth provides health-care services (clinical and non-clinical) such as preventive, therapeutic, research, assessment, health management services and continuing education to service providers.12,13
Several types of telemedicine have been developed for different health domains, including telenursing, telepharmacy telesurgery, telegenetics, telerehabilitation, telehomecare, teletrauma care, telecardiology, telepsychiatry, teleradiology, telepathology, teledermatology, teledentistry, teleaudiology and teleophthalmology.14 Some studies have evaluated the advantages of using telemedicine services in orthopaedics 15 which increase patient satisfaction, 16 reduce travels and save patients’ time.17,18
To the best of our knowledge, no accurate definition of tele-orthopaedics has been provided, and no review study has been conducted to identify and classify different applications in the field. According to the preliminary search, some studies have used the term ‘tele-orthopaedics’ to provide orthopaedic services. For example, Caffery et al. evaluated different tele-orthopaedic services in Australia and define tele-orthopaedics as the delivery of orthopaedic services remotely between an orthopaedic surgeons and patients. These services are often used for real-time teleconsultation before, during and after treatment. 19 One study used a mobile-based tele-orthopaedics system to transfer data, audio, video and images securely to specialists. 20 In another study, email-based telemedicine was used as a tele-orthopaedic service to provide orthopaedic care to patients with acute orthopaedic injuries in remote areas. 21
In this study, we used a systematic mapping review (SMR) to identify and classify the applications and services for tele-orthopaedics and to identify knowledge gaps in the field. For this purpose, previous studies were systematically reviewed for all tele-orthopaedic applications and services, orthopaedic interactions and orthopaedics diseases/injuries related to tele-orthopaedics. This study provides an overview for researchers to select appropriate subjects for primary and secondary studies. The status of tele-orthopaedics in e-health is also discussed, and a precise definition is presented. In addition, the results will help stakeholders, in particular developers and graduate students, to select appropriate subjects for further research. This study can be considered as a starting point for researchers aiming to conduct secondary studies such as systematic reviews. 22
Method
The method used in this study was a SMR, conducted to provide an overview of a research area through identifying, classifying and analysing studies published in the field of tele-orthopaedics. Although the SMR and the systematic literature review (SLR) are similar in searching and selecting the study process, they differ in terms of goals, research questions, search strategies, scope, quality assessment and results. 23 While the aim of the SLR is to identify, evaluate and interpret all evidence, the SMR is primarily concerned with structuring and classifying the research area rather than answering detailed research questions.24,25 Unlike the SLR, which has specific research questions, the research questions of the SMR are generic. As a result, the search scope in the SMR is wider than that of the SLR, which is typically more in-depth in terms of analysis and review than the SMR. The results of the SMR can often be used in a more rigorous SLR. 23
The main reasons for performing a SMR are identifying the nature and extent of the empirical study data, mapping out the researches in the field and identifying gaps and clusters in a set of primary studies in order to identify topics and areas for conducting new primary researches and more complete systematic reviews. 24
This study was conducted on the basis of the process proposed by Petersen et al.
26
:
Definition of research questions Definition of inclusion/exclusion criteria Data collection • Formulating search strategy and searching for papers resulting in a set of papers (identification process) • Screening and selecting the relevant papers, resulting in a set of relevant papers (selection process) Data extraction, classification and analysis, resulting in a systematic map (mapping process).
Research questions
According to the broad nature of questions in the SMR, the main research question of this study was: What applications, services and entities are included in tele-orthopaedics? In order to answer this question, it was necessary to answer a number of detailed questions. Therefore, the research questions were categorised as topic research questions (TRQ) and publication research questions (PRQ), as presented in Table 1.
Research questions.

Inclusion/exclusion criteria
Inclusion and exclusion criteria were used to exclude studies that were not relevant to answering the research questions. Table 2 shows the inclusion and exclusion criteria used to select and exclude articles based on our objectives.
Inclusion and exclusion criteria.

Search strategy
This part included the identification of keywords, the formulation of a search strategy and the identification of data sources for the search for tele-orthopaedic articles. Preliminary searches for tele-orthopaedics revealed the related keywords, including tele-orthopaedic, telemedicine, telehealth, e-health and m-health, which were used together with their synonyms in the search strategy. Table 3 presents the search strategy in Web of Science, Scopus, PubMed and IEEE Xplore databases. The search included articles published up to 2019.
Search strategy for databases.

Study selection
After the removal of the papers on the basis of the exclusion criteria, we carried out the selection of papers in two steps. First, two authors independently reviewed the titles and abstracts of the papers based on the inclusion and exclusion criteria and then removed the irrelevant papers (Figure 1). Only when a paper received two positive votes (from two voting authors) was it included in the study. If it received one positive vote, it was up to the positive vote of a third author to decide whether it should be included. Otherwise, it was excluded.

Information flow related to the identification, screening and selection of studies related to tele-orthopaedics.
Data extraction
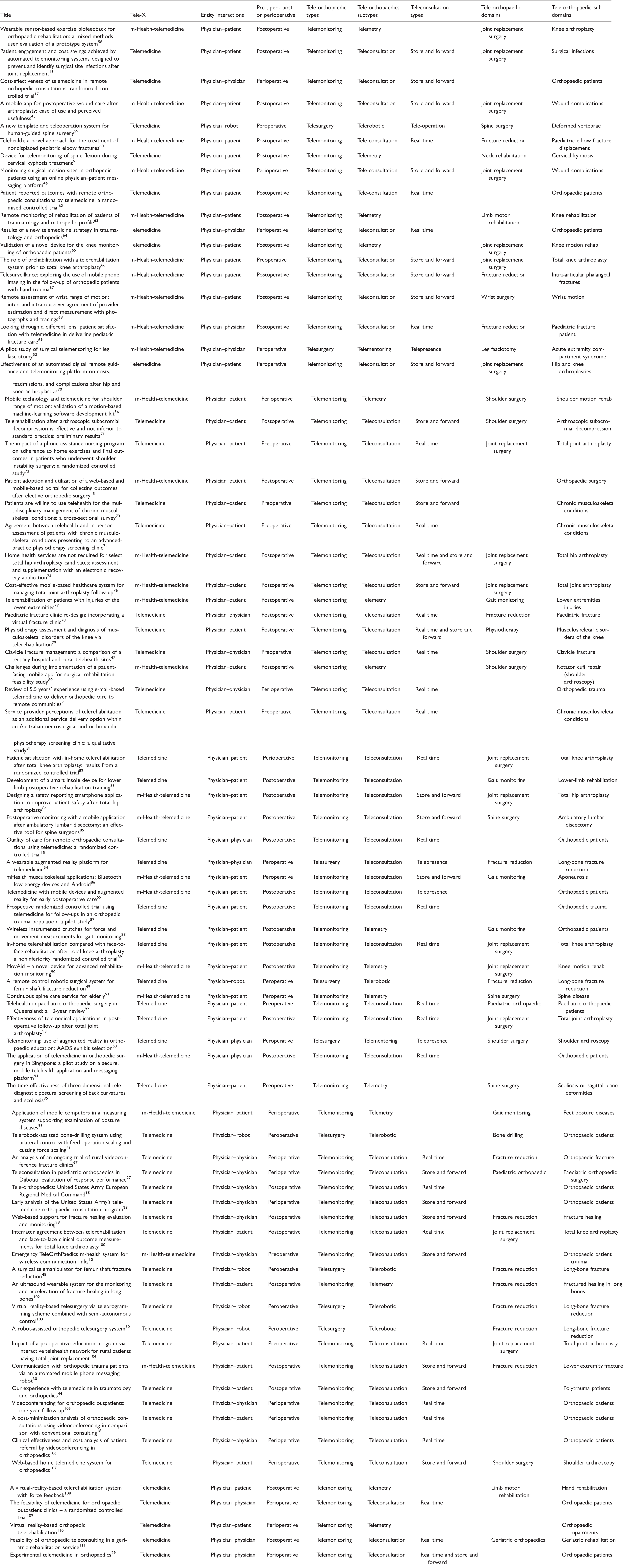
The search yielded 604 articles. After removing 219 duplicate articles, we screened 385, 205 and 132 articles by titles, abstracts and full texts, respectively. Finally, 77 relevant studies were selected for analysis (Table A in the Appendix). EndNote X9, which is a reference management tool, was used to manage the large number of references and to remove duplicates.
Data extraction results (More data available in the supplementary file)
Results
The data related to each question were entered, collected, cleaned and sorted in a Microsoft Excel spreadsheet. The data were first classified and analysed, then illustrated as tabular or visual representations for better understanding and appropriate data analysis. The results of each question were assessed separately as follows.
TRQ1: tele-orthopaedic types
Figure 2 presents the results of the tele-orthopaedic types in a hierarchical model. In the first (innermost) level, tele-orthopaedics was divided into non-mobile-based and mobile-based tele-orthopaedics, with 66% and 34% of selected articles, respectively. In the second level, tele-orthopaedics was divided into two general categories: telemonitoring (88%; non-mobile: 43 articles; mobile: 24 articles) and telesurgery (12%; non-mobile: 8 articles; mobile: 1 article). Teleconsultation (synchronous/real-time teleconsultations and asynchronous/store and forward teleconsultations), accounting for 68% of the articles, and telemetry, accounting for 20% of the articles, are the two main types of telemonitoring in orthopaedics. In addition, 4% of the articles discussed telepresence (used in telementoring) for training and guidance during surgery, and one article discussed telepresence for patient monitoring.

Tele-orthopaedic hierarchy plot.
TRQ2: orthopaedic entity interactions
In this study, individuals such as physicians or patients and devices such as robots that have important roles in providing health care to patients were considered to be orthopaedic entities. The different types of interaction between orthopaedic entities in tele-orthopaedics are physician–patient, physician–physician and physician–robot interactions.
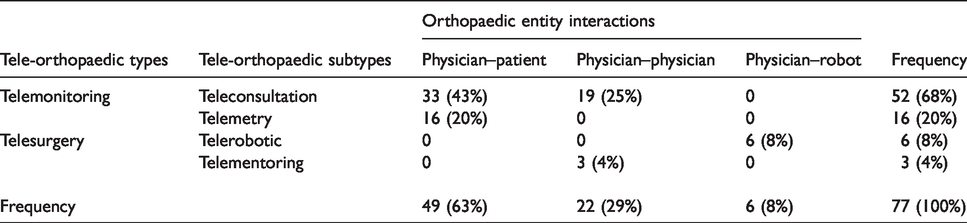
Table 4 shows that the frequency of mobile phone use and non-use in physician–patient interactions is approximately the same. Six articles also used physician–robot interactions in orthopaedic surgeries, while no article discussed the use of mobile phones for physician–robot interactions. Table 4 also shows that the proportion of mobile phone use in physician–physician interaction was very low (5% vs. 23%). Table 5 shows that physician–patient interactions were more widely used in teleconsultation (43%). The only type of interaction in telemetry was physician–patient, while telepresence (telementoring) included only physician–physician interactions and telerobotics used robot–physician interaction.
Number (%) of orthopaedic entity interactions versus tele-orthopaedic types.

Number (%) of tele-orthopaedics and orthopaedic entity interactions.
TRQ3: time periods of tele-orthopaedic uses
In this study, orthopaedic procedures were defined as surgical, rehabilitative and curative procedures applied to correct abnormalities related to bones and joints. Tele-orthopaedic services can be used at different time periods (before, during, after or throughout orthopaedic procedures). Table 6 shows the time periods that different types of tele-orthopaedics are used. Most of the articles (36%) discussed the use of tele-orthopaedic services after orthopaedic interventions. Telemonitoring (telemetry and teleconsultation) have always been used in all periods of care. Robotics, virtual reality (VR) and augmented reality (AR) technologies in telesurgery (telemetry and telementoring) have been used in the peroperative period.
Tele-orthopaedic services versus care periods of orthopaedic.

TRQ4: Orthopaedic diseases/trauma
Tele-orthopaedics delivered certain services to patient with orthopaedic problems. In this study, the orthopaedic problems discussed in different articles were evaluated in a hierarchal model at three levels (Figure 3). The first (innermost) level consisted of four sections, including orthopaedic surgery, trauma, rehabilitation and not defined in the selected articles. According to Figure 3, about 50% of tele-orthopaedic articles were presented to orthopaedic surgeries of which about half were related to joint arthroplasty (JA). Knee arthroplasty (KA), hip arthroplasty (HA) and shoulder arthroplasty (SA) with eight, three and one articles, respectively, are the three main forms of JA.
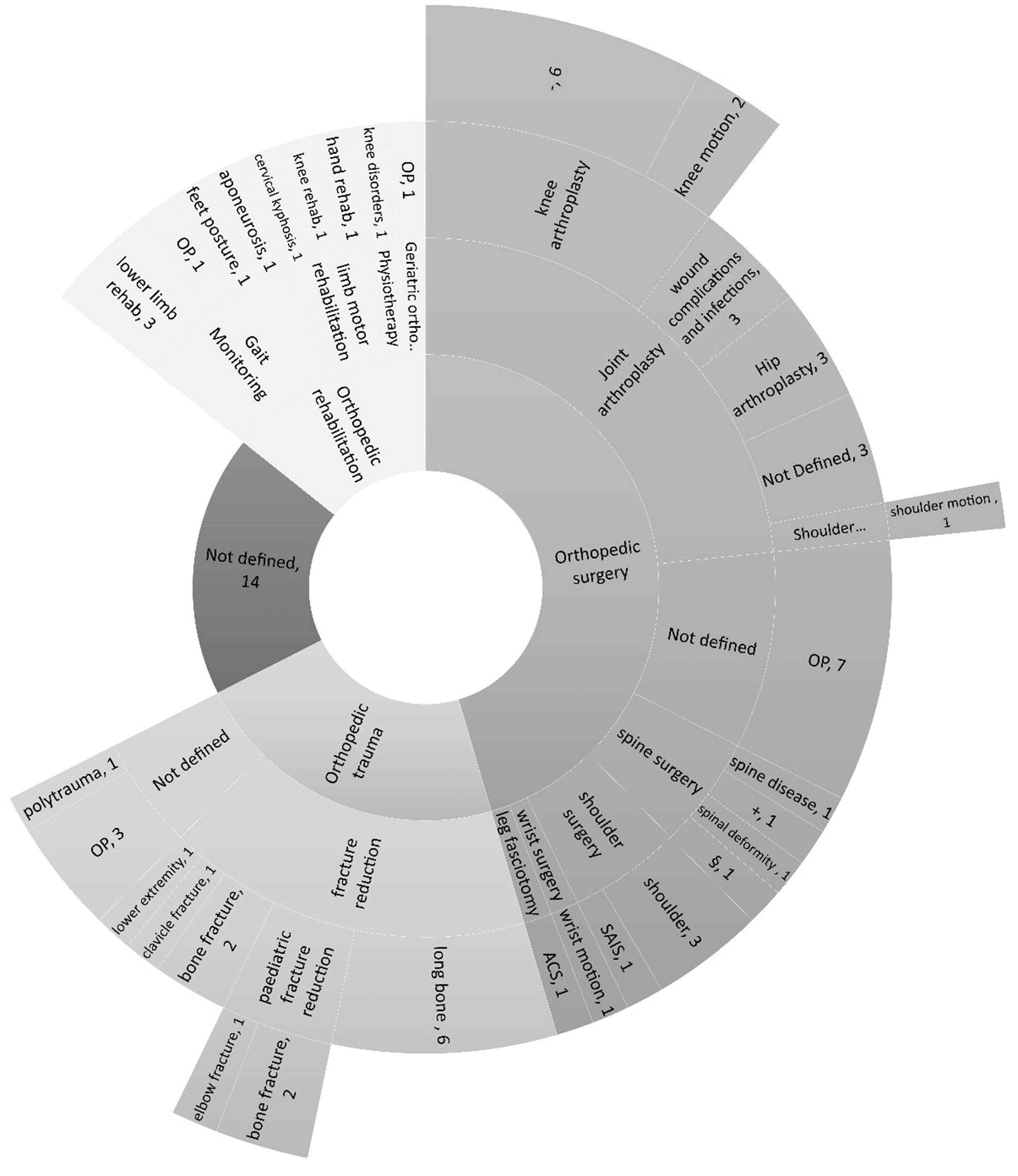
Orthopaedic diseases/trauma in tele-orthopaedics.
Approximately a quarter of tele-orthopaedic articles were related to orthopaedic trauma, and a significant proportion of them (about half) discussed reduction of fractures. A number of articles (18%) did not clearly refer to the specific orthopaedic problem, and these were categorised as not defined. The rest of the articles were related to orthopaedic rehabilitation (13%).
PRQ1: distribution of publications
Figure 4 presents the annual trend in the distribution of tele-orthopaedic articles from 1996 to 2019. No upward trend was observed in publications related to tele-orthopaedics prior to 2009, and no relevant studies were published for a number of years. The first articles about non-mobile-based and mobile-based tele-orthopaedics were published in 1996 and 2004, respectively. Overall, the most articles (16; mobile-based: 9; non-mobile-based: 7) were published in 2019. There has been an increasing trend in the use of mobile-based tele-orthopaedics since 2013.
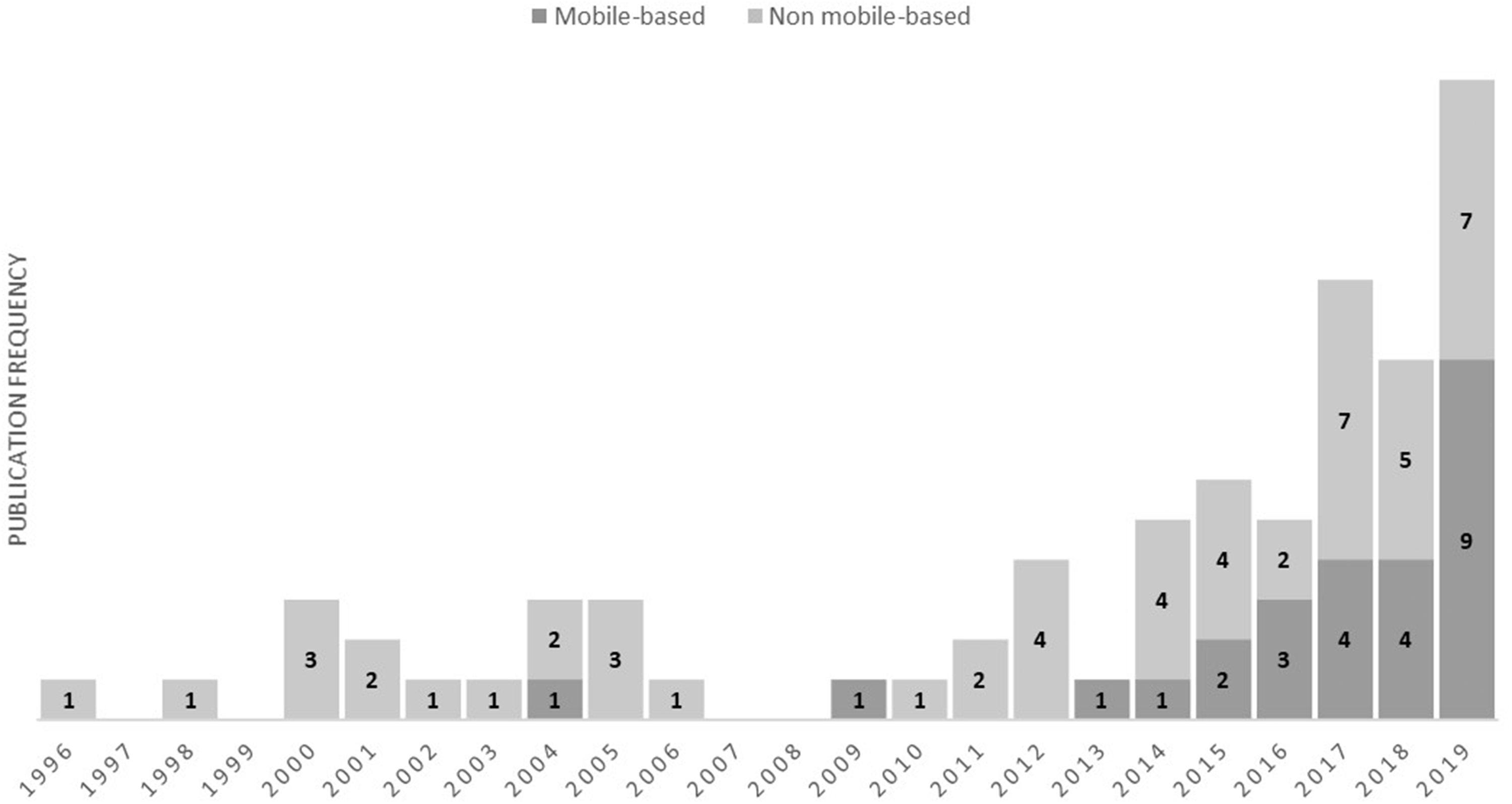
Tele-orthopaedic publications trend per year.
Of all the articles selected for this study, 82% and 18% of them were published or presented in scientific journals or conferences, respectively (Figure 5). The 63 journal articles were published in 34 different journals, of which about 41% were published in three journals, including the Journal of Telemedicine and Telecare, Telemedicine and e-Health and Journal of Arthroplasty (Figure 6).
Contributions of journals and conferences in tele-orthopaedics.

Contributions of journals in tele-orthopaedics.
PRQ2: active countries
Figure 7 shows that 26 different countries have contributed to tele-orthopaedics applications. The USA and Australia have published the largest numbers of articles on tele-orthopaedics (23 and 8 articles, respectively), followed by Canada and Finland, each with five articles.

Countries contributing to tele-orthopaedics.
It should be noted that some tele-orthopaedic services have been used to establish interactions between orthopaedic entities in different countries. For example, due to the shortage of paediatric orthopaedic surgeons and resources in Djibouti, teleconsultation has been established with paediatric orthopaedic specialists in French medical centres. 27 Another study investigated teleconsultation with US medical centres for common musculoskeletal problems, including fractures, sprains and tendon injuries to the US army in Iraq, Navy Afloat and Afghanistan. 28 However, few efforts have been made in many of these areas to address these problems.
Discussion
In this study, studies related to tele-orthopaedics were reviewed using systematic mapping. Approximately 82% of these studies were published in professional journals with a good impact factor, and the rest were presented at international conferences. The Journal of Telemedicine and Telecare and Telemedicine and e-Health were the most relevant journals, publishing 35% of the studies in this field. A growing trend in the number of studies in this field has been observed in the results of this study, demonstrating that the use of mobile devices in tele-orthopaedics is increasing. The first paper that was found in the current review was published in 1996 and discusses the synchronous consultation and sending of images between physicians remotely. 29 The first article on mobile-based tele-orthopaedics was published in 2004, which elaborates on the use of a mobile-phone messaging system to facilitate physician–patient interaction. 30 In 2019, the number of studies focusing on mobile use in tele-orthopaedics was higher than at any other time. This further demonstrates the importance of mobile devices in providing orthopaedic services to patients.
The current study reviewed active countries in the field of tele-orthopaedics and showed that the USA, Australia, Canada and Finland are more active among 26 countries, conducting more than half of the studies in different forms of tele-orthopaedics. The results of this study show that countries with a higher number of tele-orthopaedic services are among developed countries, indicating that the policies of developed countries in the field of telemedicine play an important role in the application of telecommunications technologies in the provision of orthopaedic services to patients and in reducing costs as well. Countries such as the USA, Australia, Canada and China are among the top 10 largest countries that are logically more involved in health-care issues in providing orthopaedic services to patients remotely. Therefore, they are more likely to use tele-orthopaedic services. Their geographical vastness necessitates more advanced health-related communication opportunities, which in turn culminates in attempts to expand tele-orthopaedics by means of telecommunications technology research.
There is a significant difference between the USA and the rest of the active countries in the provision of tele-orthopaedic services to patients. The USA alone contributed 30% of the studies in this field. Tele-orthopaedics in the USA may have been of interest for a number of reasons, including: musculoskeletal problems are the leading cause of disability and poor quality of life 31 (musculoskeletal problems affect more than one out of every two people aged ≥18 years and nearly three out of four people aged ≥65 years in the USA32), musculoskeletal problems are the most prevalent and chronic conditions in all people in their midlife, 31 the economic impact of musculoskeletal problems, 33 the USA’s geographical size and the advancement of telecommunications technologies in the country.
According to the WHO, musculoskeletal conditions were the leading cause of disability in four regions, including the Americas, South East Asia, Europe and the Western Pacific. Of the six WHO regions in 2017, these conditions were ranked second and third in the Eastern Mediterranean and Africa, respectively. 2 However, due to lack of access to orthopaedic resources in many of these regions, orthopaedic services are still not properly provided in many of these regions, in particular South East Asia, the Eastern Mediterranean and Africa. Tele-orthopaedics can help reduce or alleviate these deficiencies in order to deliver orthopaedic services to patients. The results of this study show that tele-orthopaedics is well developed in North America, the Western Pacific and Europe. In three other regions, including developing and underdeveloped countries, however, telecommunications technologies have not yet been used to provide services to orthopaedic patients.
Tele-orthopaedic services are categorised into orthopaedic surgery and orthopaedic trauma that involve various diseases/traumas. In orthopaedic surgery, JA procedures, one of common orthopaedic surgeries, are usually performed when joints have been damaged. 34 KA, HA and SA with 23%, 9% and 3% of tele-orthopaedic surgeries are the main three procedures of JA, respectively. This finding is also in line with a hospital discharge study for arthritis conditions in the USA in 2011, in which all discharges are performed on the KA, HA and SA with 1.8%, 1.2% and 0.2% of total procedures. 34 Bone fractures are also one of the most common musculoskeletal injuries/traumas. In 2013, about 25% of musculoskeletal injuries/traumas treated in a health-care facility were related to bone fracture in the USA. 35 The results of this study indicate that fracture reduction is the main orthopaedic procedure, with 80% of orthopaedic injuries/traumas used in the treatment of bone fractures in the correct alignment.
The mapping results indicate that different types of interactions exist between orthopaedic entities, including physician–physician, physician–patient and physician–robot interactions. Although the physician–physician and physician–robot interactions are in fact an indirect interaction between a physician and a patient, the proportion of physician–patient interactions (63% of studies) was more than twice that of the other two interactions. The physician was present in all these interactions and provided orthopaedic services to patients. In view of the important role of physicians in the delivery orthopaedic services to patients remotely, and because of the prominent curative aspects of these services, tele-orthopaedics is considered to be a subset of telemedicine. According to the results and definitions of telemedicine, a hierarchical model was proposed for tele-orthopaedics (Figure 8). In this model, e-health was placed in the outermost level and included telehealth, telemedicine and tele-orthopaedics in a hierarchical fashion.

Tele-orthopaedics in the hierarchical structure of e-health, telemedicine, telemedicine and m-health.
Increased use of mobile phones leads to access to health-care services, reduces the costs and provides the opportunity for delivering high-quality services.36,37 m-Health is subset of e-health that provides health-care services based on mobile technologies. 37 The results of this study showed increased use of smartphones in orthopaedics, from one article in 2013 to nine articles in 2019. Telemedicine has a longer history than m-health. with the first paper in tele-orthopaedics published in 199629 and the first article on the use of the mobile phone in tele-orthopaedics published eight years later. 30 One third of the articles used mobile technology in tele-orthopaedics. Therefore, a marked increase is expected in the use of mobile technology in tele-orthopaedic services in the future. Some studies used mobile devices as measurement or data presentation tools in e-health. For example, Pereira et al. used the mobile phone as a goniometer for measuring and presenting the range of motion in patients with knee motion limitation. 38
Tele-orthopaedics is divided in two major types: telemonitoring (88%) and telesurgery (12%). The former uses audio/video and other information processing and electronic communication technologies to monitor the status of patients remotely. Teleconsultation (68%) and telemetry (20%) are considered two forms of telemonitoring. Teleconsultation is one of the most important methods of care based on information technology. 39 Real-time (36%) and store and forward (32%) are two methods of teleconsultation interactions used to present an interaction between the patient and health-care provider for monitoring and providing feedback.40,41 In addition, telemetry is a form of telemonitoring that is used to transfer biological and physiological data from a remote location to another place for interpretation and decision making. 42
The results of this study showed that the telemonitoring was the most important service in both forms of mobile-based and non-mobile-based tele-orthopaedics. A number of applications, such as mobile apps, 43 emails,21,44 web forms or mobile portals 45 and messaging platforms, 46 have been developed for collecting medical data through mobile-based teleconsultation that allow patients to complete the information related to their health status and forward it to their physicians. Therefore, these consultations were categorised as asynchronous teleconsultation. Synchronous non-mobile-based teleconsultations (32%) and asynchronous mobile-based teleconsultations (17%) were used more than two other forms in tele-orthopaedics.
Teleconsultation has received attention for guiding patients at different periods of time (before, during and after orthopaedic interventions). The interactions between orthopaedic entities in teleconsultation take two main forms: patient–physician (43%) and physician–physician (25%). The results of this study indicate that the different types of teleconsultations focus on patient–physician interactions. In physician–physician consultations, after visiting a patient, the physician interacts with another physician or specialist elsewhere in order to assess the patient’s status.15,47
With respect to telesurgery, we found in our analysis of selected studies that two types of telesurgery (telerobotics and telepresence) have been used in tele-orthopaedics. Most robot-based orthopaedic operations have employed telemanipulate technology, which includes a slave–master system.48–51 AR/VR technologies also have been used to realise the specialist’s presence in operations and to direct other specialists.52–54 In one study, physicians used mobile and AR/VR technologies to deliver postoperative care to patients. This service can be considered as synchronous consultation. 55 In another study, physicians used mobile and AR/VR technology in leg fasciotomy as telepresence. 38 In telementoring, the physician is virtually present from another location using telepresence, and specialists can participate in a surgical or curative procedure using smartphones and AR/VR technology.54,55
Definition of tele-orthopaedics
There seems to be a lack of a comprehensive and precise definition for tele-orthopaedics in the field. According to the results of this study and the definition of telemedicine, it is now possible to present an accurate definition for tele-orthopaedics as follows: tele-orthopaedics is subset of telemedicine that enables orthopaedic surgeons to deliver orthopaedic services using communication and information technologies to patients with chronic orthopaedic disorders or orthopaedic trauma remotely.
Knowledge gaps in tele-orthopaedics
Different applications have been designed and developed to establish physician–patient interactions, especially for teleconsultation. In the majority of these interactions, the data related to the patient’s health status are collected by the patient after orthopaedic procedures and sent to the physician (store and forward teleconsultation), while no attention has been paid to the use of mobile devices in real-time teleconsultation. The use of mobile devices in real-time teleconsultation as audio/video is an interesting subject for researchers and care providers in the field. Video-conferencing systems such as TV or computer systems are often used to establish physician–physician interactions. The immobility of these systems is one of the disadvantages of this type of consultation. Therefore, it seems that the use of mobile phones or tablets is more useful for this type of interaction.
Teleconsultation has been employed in all treatment stages (pre-, per- and postoperative) mainly for monitoring, training and guiding patients. The results of this study show that little attention has been given to perioperative teleconsultation. Also, perioperative physician–physician consultations are referred to as telementoring, in which AR/VR technologies are used. According to the advantages of AR/VR technologies in tele-orthopaedics, especially for teleconsultation and telementoring, these technologies may have a significant role in decreasing costs and enhancing the quality of treatment.56,57 On the other hand, mobile devices have been used in many tele-orthopaedic services, but only one study investigated mobile-based telesurgery. 52 So, there is still a long way to go to use AR/VR, mobile devices and robots in tele-orthopaedics.
Limitations
A number of limitations regarding this study are worth mentioning. Although the four main databases (medical and engineering databases) that cover the articles in the field were selected to conduct search strategy, other databases were not considered. Searching the reference lists of selected articles were not considered. Thus, it is possible that some relevant studies have been missed. Unlike a systematic review, quality assessment of selected articles is optional in SMR. Therefore, in this study, we did not consider a quality assessment of the chosen articles.
Conclusion
Recently, the number of requests for access to orthopaedic services (consultation, diagnosis and treatment) has increased, but despite that, advancements in telecommunication technology for tele-orthopaedics are still in their early stages. Tele-orthopaedics has been part of telemedicine, providing interactions mostly between physicians and patients. By mapping the articles in the field, two major forms of tele-orthopaedics have been identified: telemonitoring and telesurgery.
One third of the studies referred to the use of mobile devices in tele-orthopaedics. It seems that the use of mobile phones in tele-orthopaedics will increase in the future. As mobile devices are rarely used in telesurgery, advancements in AR/VR technologies and mobile devices can help surgeons use mobile phones in orthopaedics surgeries.
Two-way online/offline interactions between an orthopaedic entity (patient, health-care provider or robot) and a provider by means of audio/video-based telecommunications technologies can be used for consultative orthopaedic services. Mobile apps or messaging services (email or short message) are used for mobile-based consultation to collect patient data and send them to the physicians. Mobile phones are used asynchronously in the majority of the consultations. Another form of consultation is real-time audio/video communication between the patient and the physician. Developing various real-time apps for smartphones can result in more smartphones being used in real-time teleconsultation.
Most tele-orthopaedic services were provided postoperatively to patients with orthopaedic surgery or orthopaedic trauma. Most of these services were given to patients with chronic orthopaedic conditions, most of whom had been treated by surgery. Joint replacement and fracture reduction are the two important procedures for orthopaedic patients in need of orthopaedic services.
A great deal of attention is being paid to tele-orthopaedics in both developed and large countries due to its impact on cost reduction and the availability of orthopaedic services. Following developments in ICT and the increasing use of smartphones, many residents still do not benefit from orthopaedic services at home. Tele-orthopaedics can be expected to be used in any country to distribute orthopaedic services fairly and equitably among patients at affordable cost.
Supplemental Material
sj-xlsx-1-jtt-10.1177_1357633X20919308 - Supplemental material for Tele-orthopaedics: A systematic mapping study
Supplemental material, sj-xlsx-1-jtt-10.1177_1357633X20919308 for Tele-orthopaedics: A systematic mapping study by Ali Behmanesh, Farahnaz Sadoughi, Farid Najd Mazhar, Mohammad Taghi Joghataei and Shahram Yazdani in Journal of Telemedicine and Telecare
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was a part of a PhD dissertation supported by Iran University of Medical Science (Grant No: IUMS/SHMIS-97-3-37-12579).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.