
Abstract
Introduction
The primary purpose of this review was to evaluate patient and physician preference and satisfaction for teleconsultation in orthopaedic surgery compared to traditional face-to-face consultation. In addition, we evaluated the effects of teleconsultation on patient length of visit, healthcare costs, range of motion (ROM), pain, quality of life (QOL), and ongoing management plans.
Methods
A systematic review of MEDLINE, Embase, Web of Science, and Cochrane Library was conducted according to PRISMA guidelines. Randomised control trials and case control studies comparing teleconsultation with traditional, face-to-face consultation in the management of orthopaedic conditions were included. The primary outcome measures were patient and physician preference and satisfaction. Secondary outcomes included patient length of visit, healthcare costs, ROM, pain, QOL, and ongoing management plans.
Results
A total of 13 articles meeting the eligibility criteria were included for systematic review and 8 for meta-analysis. There was no significant difference in patient satisfaction, length of visit, or time spent with the physician between the telemedicine and in-office control group. The mean difference of patient preference for telemedicine was significantly higher in the telemedicine group compared to the in-office visit group (OR 1.44, 95% CI 1.12–1.87, p = 0.005).
Discussion
Telemedicine was not inferior to face-to-face office visits in regard to patient and physician preference and satisfaction. Therefore, it would be an effective adjunct to face-to-face office visits, serving as a mechanism of triage and long-term continuity of care.
Introduction
Telemedicine, the use of electronic technologies to deliver healthcare remotely, has recently gained great interest as a result of the COVID-19 pandemic.1–5 With demand for healthcare services escalating and resources limited, conventional face-to-face office visits have proven to be a challenge for patients and healthcare workers alike. Telemedicine consultation (i.e. teleconsultation) offers a potential solution to such challenges by using real-time videoconferencing between physician and patient, as well as between physician and specialist, to deliver more timely and convenient care.6,7 By removing geographic and economic barriers, teleconsultation enhances access to healthcare, 8 reduces unnecessary costs, 8 and improves patient satisfaction and health-reported outcomes. 9 When used as a triage mechanism, teleconsultation reduces unnecessary follow-up appointments, 10 lowers hospital costs, 11 and improves physician workflow and satisfaction.12,13
Even before the arrival of COVID-19, the use of teleconsultation has been steadily increasing across the United States, Canada and Europe. 14 However, it has not been equally adopted across all healthcare fields. While the benefits of teleconsultation have been demonstrated in the fields of radiology, cardiology, dermatology, psychology and general surgery, 15 its role in orthopaedic surgery is not as clear.16–18 Most of the existing literature on orthopaedic teleconsultation relies on asynchronous communication through a ‘store and forward’ approach, where patients send images to physicians regarding their medical condition.19–22 In a recent scoping review, Behmanesh et al. discovered that most teleconsulations are conducted asynchronously using mobile phones, a practice that is expected to increase in the next few years. 23 However, such asynchronous methods have come under scrutiny due to the lack of personal interaction between patient and provider.24,25
A strong patient–physician relationship has not only been shown to enhance patient satisfaction, but also to foster trust between patient and physician, leading to overall improved health outcomes. 26 With advancements in technology and improved Internet access, the use of synchronous real-time videoconferencing allows for a more personal approach to telemedicine that most closely resembles traditional office visits. Such methods have gained strong patient interest in the setting of primary care; however, further studies are needed to determine the content, safety, efficacy and cost-effectiveness of employing such technologies in the field of orthopaedics. 27 The purpose of this review was to evaluate patient and physician preference and satisfaction for real-time video-based teleconsultation in the management of orthopaedic conditions compared to traditional face-to-face office visits. In addition, we evaluated the use of teleconsultation on patient length of visit, healthcare costs, range of motion (ROM), pain, quality of life (QOL), and ongoing management plans.
Methods
Search strategy
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for systematic reviews. 28 A comprehensive search of available literature from the electronic databases MEDLINE, Embase, Web of Science, and Cochrane Library was conducted on 5 April 2020 by two independent reviewers (CM and DK). The following MeSH terms were used: “telemedicine” OR “telehealth” AND “orthopaedics” OR “orthopaedic procedures” OR “orthopaedic surgery” OR “teleorthopaedics” AND “tele-orthopaedics”.
Eligibility criteria
We applied the following inclusion criteria: (a) teleconsultations performed by a medical doctor or surgeon, (b) randomised control trial or case control study, (c) published only in English, (d) published between 1 January 2000 and 1 January 2020, (e) full text available. Studies were excluded if they met the following criteria: (a) evaluation of telerehabilitation (i.e. physiotherapy), telemonitoring or wearable devices, (b) web-based follow-up, (c) non-peer reviewed, (d) review article. Preliminary studies for which a follow-up article was available were also excluded (Figure 1).
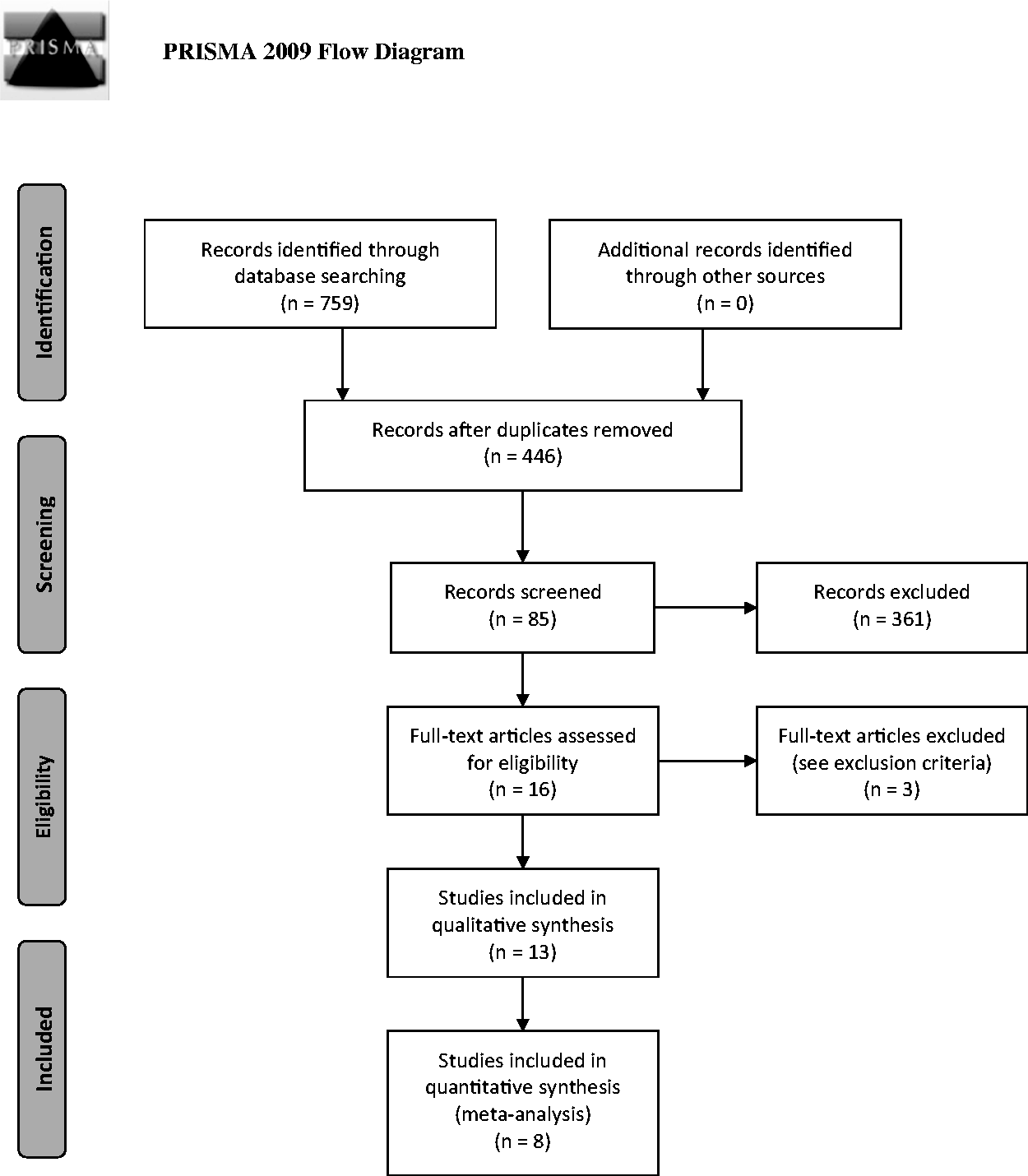
Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flowchart.
Study selection
Figure 1 outlines the PRISMA flow diagram for inclusion and exclusion of articles for this study. Our initial search was filtered by English-language articles published between 1 January 2000 and 1 January 2020 and yielded 759 articles. After duplicates were removed, 446 articles were screened by title and subsequently 85 articles screened by abstract. Sixteen articles received full-text screening with 13 eligible for systematic review and 8 for meta-analysis. Three articles were preliminary studies whose updated versions were already included for review, and as a result were excluded as duplicates. Five studies were excluded from the meta-analysis due to the lack of comparable outcomes. All online screening was performed using Covidence online software (Covidence, Melbourne, Australia), with both reviewers (CM and DK) voting on article inclusion or exclusion according to the predetermined criteria. Articles for which the reviewers’ recommendations conflicted were discussed to reach consensus.
Outcomes of interest
The primary outcomes of interest were patient and physician preferences and satisfaction. Secondary outcomes included patient length of visit, healthcare costs, and functional outcomes such as ROM, pain, QOL, and ongoing management plans.
Data analysis
Data were extracted from all eligible studies using a standardised Excel (Microsoft, Redmond, WA) spreadsheet by two reviewers (CM and DK). Data included study characteristics, demographics, initial or follow-up visit, orthopaedic condition being treated and outcome measures. Data from eight studies were pooled in a statistical meta-analysis using RevMan 5.3 (Cochrane, London, UK), 29 with risk ratios pooled using the Mantel–Haenszel method for a random effects model, due to the heterogeneity among studies. Descriptive statistics were used to summarise demographic data. We calculated risk ratios on pooled data with a 95% confidence interval (CI) for variables of interest. A p-value <0.05 was deemed statistically significant. Heterogeneity was calculated using chi-squared and I-squared tests.
Risk of bias
Risk of bias was evaluated using the revised Cochrane Risk of Bias tool for randomised trials (RoB2) 30 for the 10 randomised control trials and the Risk Of Bias In Non-Randomised Studies of Interventions (ROBINS-I) 31 for the three case control studies.
Results
Study characteristics
Eight studies were conducted in Europe,15,32–38 four in North America,2,16,39,40 and one in South America 41 (Table 1). Participants were recruited from either an outpatient clinic15,32,33,35,37,40,41 or hospital-based setting2,16,34,36,38,39 for the management of a specific orthopaedic condition. In most studies, consultations were used to follow up2,16,34,36,38,39 or in combination with an initial visit,32,33,35,37,40 with only two studies using teleconsultation as an initial method of contact.15,41 In all studies except for one, individuals were randomly grouped into either the telemedicine or control group; Good et al. 34 had all patients undergo telemedicine and control interventions. Videoconferencing was the main method of teleconsultation, with telephone interviews used in one study. 36 In eight studies the teleconsultation was conducted at the patient’s home; however, five studies required the patient to travel to a remote medical centre.32,33,35,37,38 The main outcome measures evaluated were patient and physician preference and satisfaction, with secondary measures including healthcare costs, length of visit, ROM, pain, QOL, and ongoing management plans.
Summary of individual studies.

RCT: randomised control trial; F/u: follow-up; LOV: length of visit; ROM: range of motion; QOL: quality of life; RoB: Risk of Bias (L: low, M: medium, H: high); ORIF: open reduction and internal fixation.
Risk of bias within studies
Figures 2 and 3 depict the assessed risk of bias for the 10 randomised control trials, 30 and Figures 4 and 5 for the three case control studies. 31
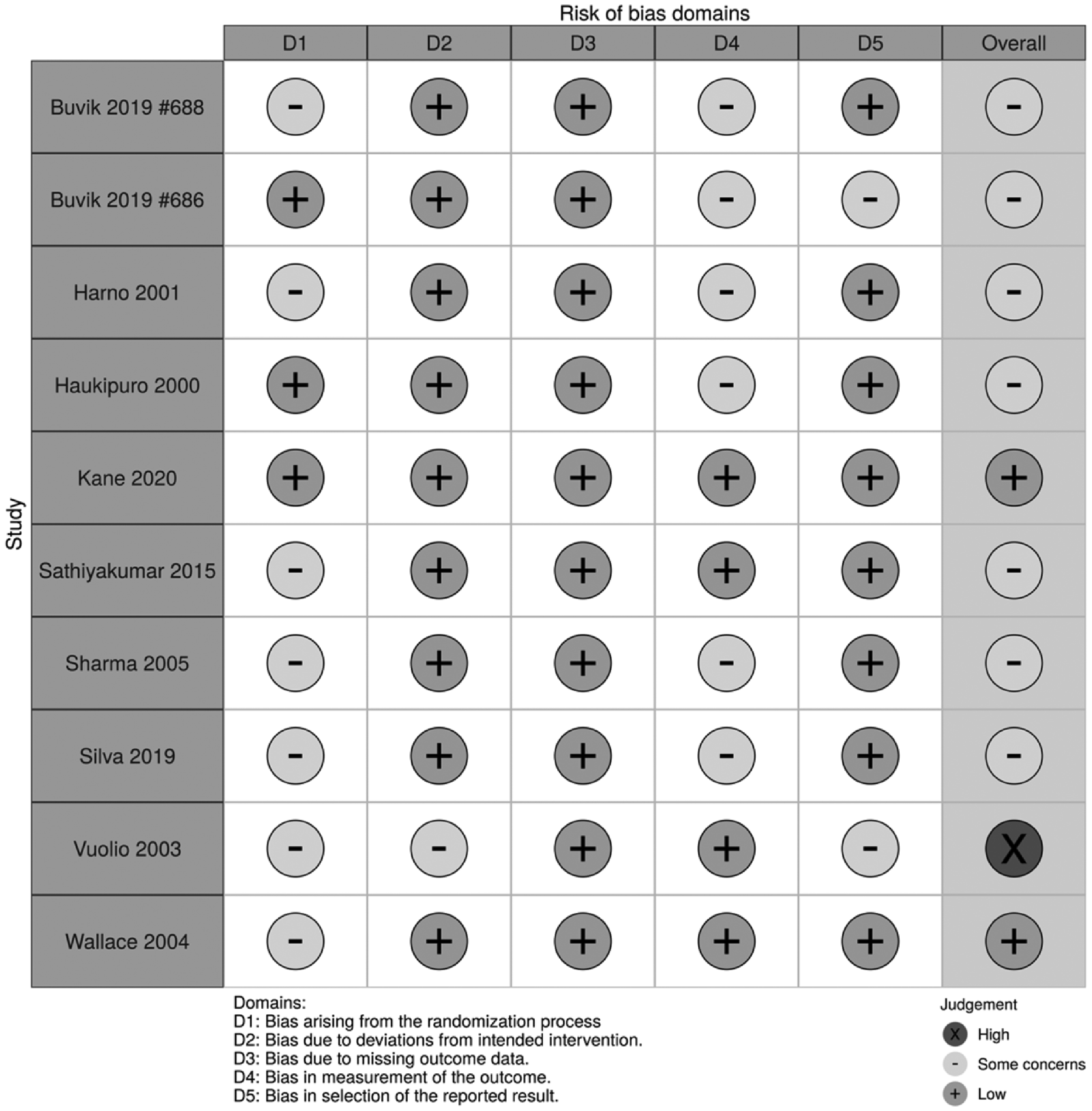
Revised Cochrane Risk of Bias tool for randomised trials (RoB2) summary.Buvik 2019 #688 refers to reference 32, and Buvik 2019 #686 refers to reference 33.
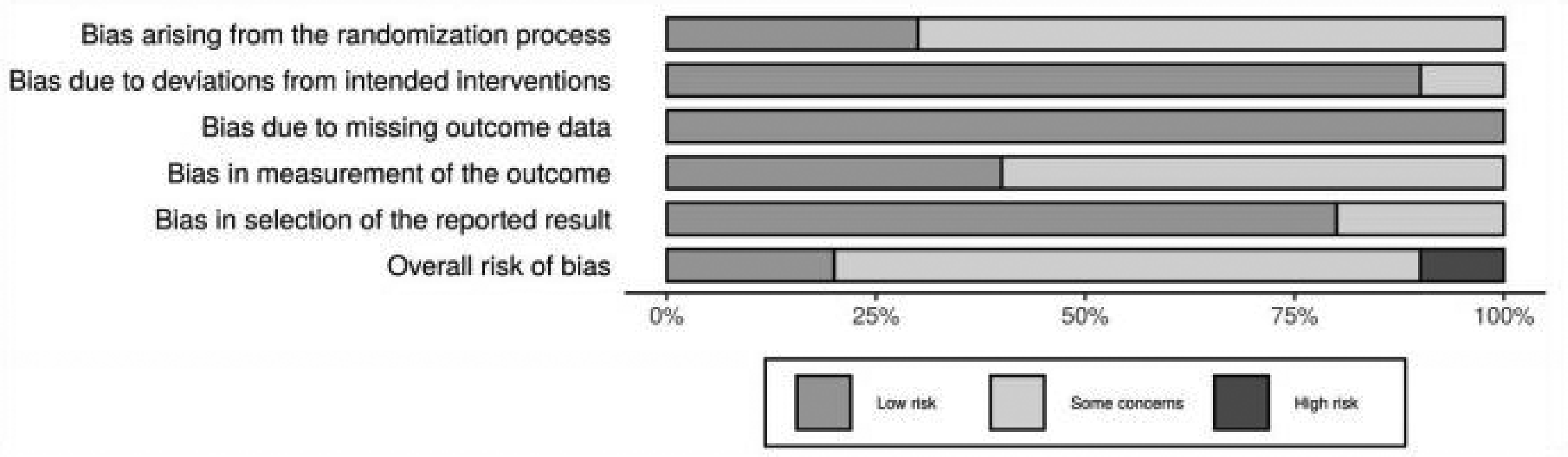
Revised Cochrane Risk of Bias tool for randomised trials (RoB2) bar graph.

Risk Of Bias In Non-Randomised Studies of Interventions (ROBINS-I) summary.
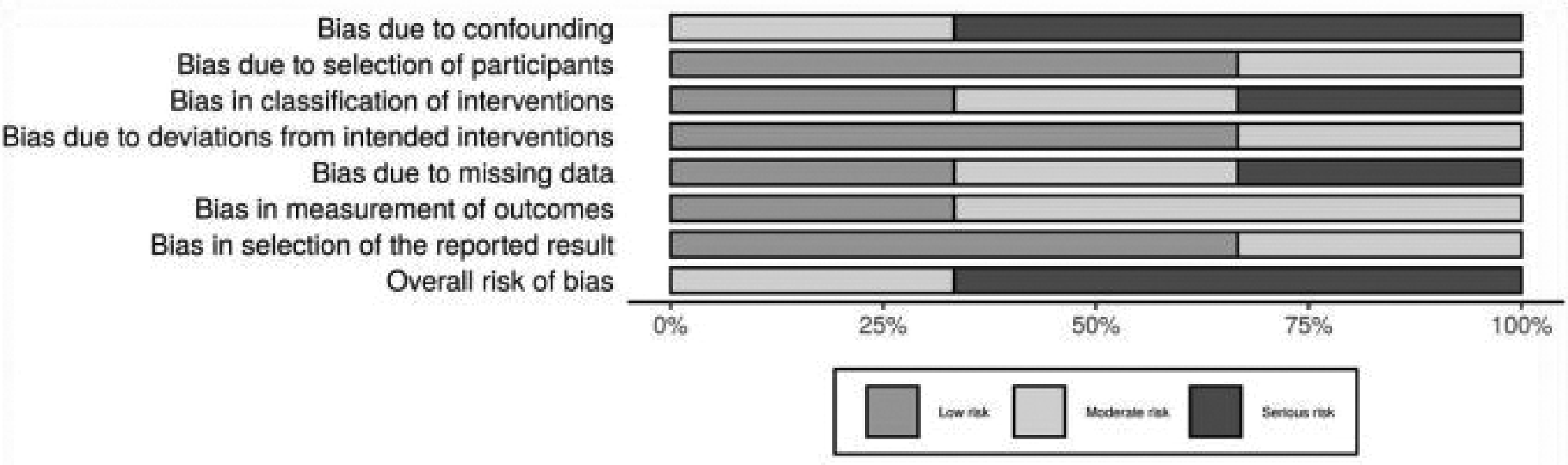
Risk Of Bias In Non-Randomised Studies of Interventions (ROBINS-I) bar graph.
Results of individual studies
Patient and physician preference and satisfaction
Four studies demonstrated no significant difference in patient or physician satisfaction as a result of teleconsultation.2,16,33,35 Wallace et al. 38 revealed a significant increase in patient satisfaction in the telemedicine group (p < 0.001). A statistically significant number of patients preferred telemedicine to traditional in-office visits in three studies.2,33,35 Haukipuro et al. 35 reported that 97% of patients in the telemedicine group chose videoconferencing for the next visit compared to 75% in the control group (p < 0.001). Not only did Kane et al. 2 show a stronger patient preference for telemedicine, but a stronger preference for telemedicine was achieved among surgeons (p < 0.001).
Length of visit
Four studies demonstrated a longer length of consultation in the traditional office group when compared to the telemedicine group.2,35,39,40 In addition to shorter consultation times, Atanda et al. 40 reported shorter wait times in the telemedicine group (2 vs 33 min, p < 0.001). Silva et al. 39 reported an average consultation length of 17.6 min (95% CI 14.9–20.3 min) and 47.2 min (95% CI 40.2–54.1 min) for patients in the telemedicine and control group, respectively (p < 0.001). When travel time was included, the length of consultation increased significantly in the control group to 110.7 min (95% CI 98.2–123.2 min) compared to the telemedicine group (p < 0.001).
Healthcare costs
In all but one study, telemedicine was found to reduce healthcare costs. Atanda et al. 40 revealed a significant healthcare cost reduction of US$24 per patient (US$114 in-office vs US$90 telemedicine group; p < 0.001). In contrast, Wallace et al. 38 demonstrated a total inflation of healthcare costs by £133 per patient (95% CI £53–213, p = 0.023) as a result of implementation of the technology and annual fees; however, there was a significant reduction in overall patient costs of £7.24 (95% CI £4.62–9.87, p < 0.0001) mostly due to savings in transportation. Buvik et al. 32 and Wallace et al. 38 calculated production loss (i.e. time spent away from work), estimating a mean inflation of €130.73 and £10.76 (95% CI £9.77–11.75, p < 0.0001) per patient in the telemedicine and control group, respectively.
Functional outcomes
There was no significant difference in ROM between teleconsultation and in-office visits.2,34,36,39 Following arthroscopic rotator cuff repair, patients demonstrated comparable passive flexion and extension regardless of consultation style (p = 0.339). From a physician’s perspective, there was no difference in the ability to assess ROM (p = 0.339). 2 A significant reduction in pain was reported by Buvik et al. 33 at 12-month follow-up (p = 0.025). Despite the use of different pain scales, no significant difference between the telemedicine and in-office groups was reported in the remaining three studies.2,36,39 QOL was assessed using either the European Quality of Life Five-Dimension Index (EQ-5D)32,33 or the Short Form-12 (SF-12), 38 both of which indicated no significant difference between groups. Vuolio et al. 37 identified no significant difference in management plans between teleconsultation and in-office groups, either in first-admission or follow-up patients (p-values not provided).
Meta-analysis
Eight studies were included in the meta-analysis due to comparable outcomes between studies. The mean difference in patient satisfaction between the telemedicine and control group was 0.10 (95% CI –0.07–0.27, p = 0.27; Figure 6). The mean difference in patient length of visit was –11.13 (95% CI –25.77–3.51, p = 0.14; Figure 7). The risk ratio of patient preference for telemedicine was 1.44 (95% CI 1.12–1.87, p = 0.005; Figure 8). The mean difference in time spent with the physician was –0.08 (95% CI –0.63–0.47, p = 0.77; Figure 9).
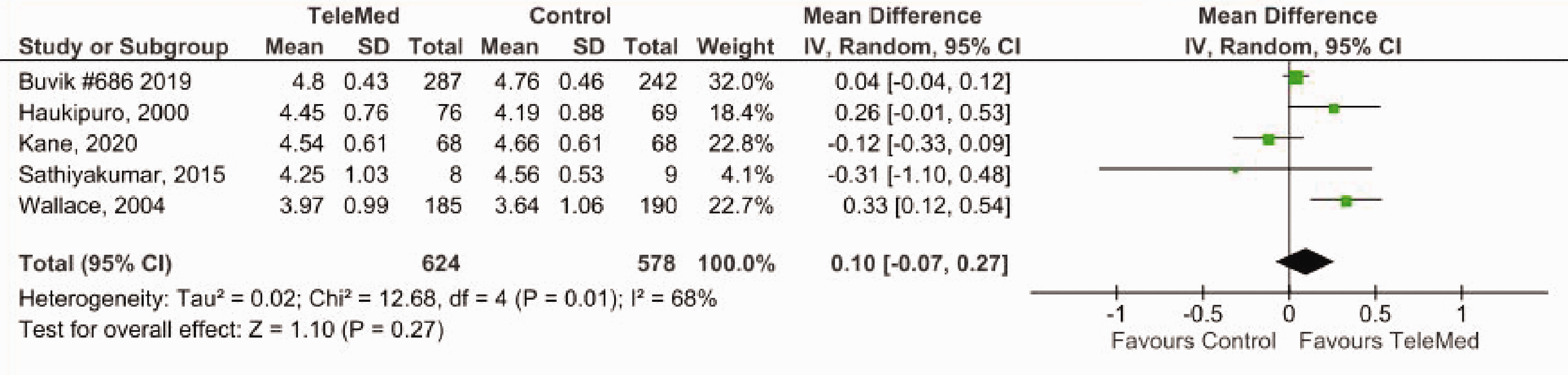
Mean difference in patient satisfaction in telemedicine vs control.
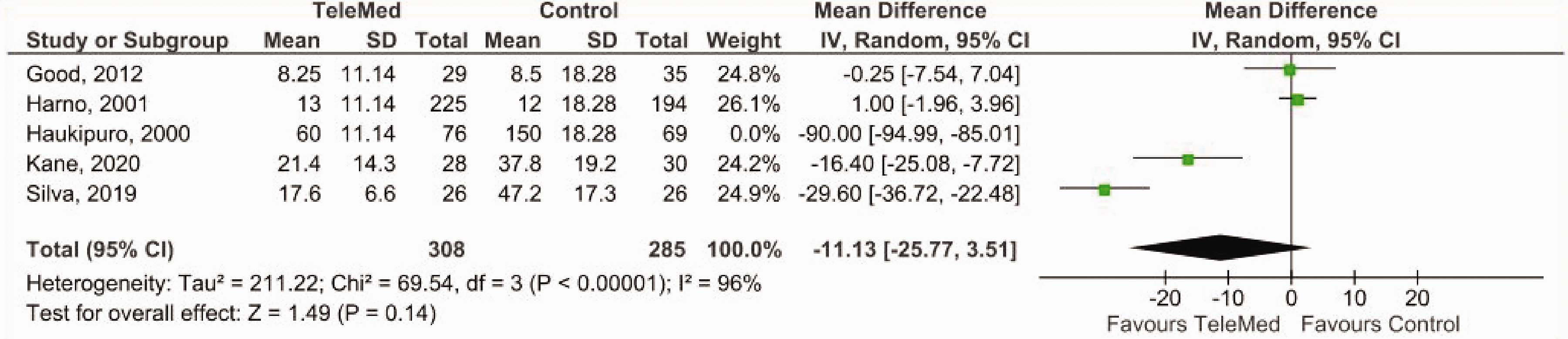
Mean difference in patient length of visit in telemedicine vs control.
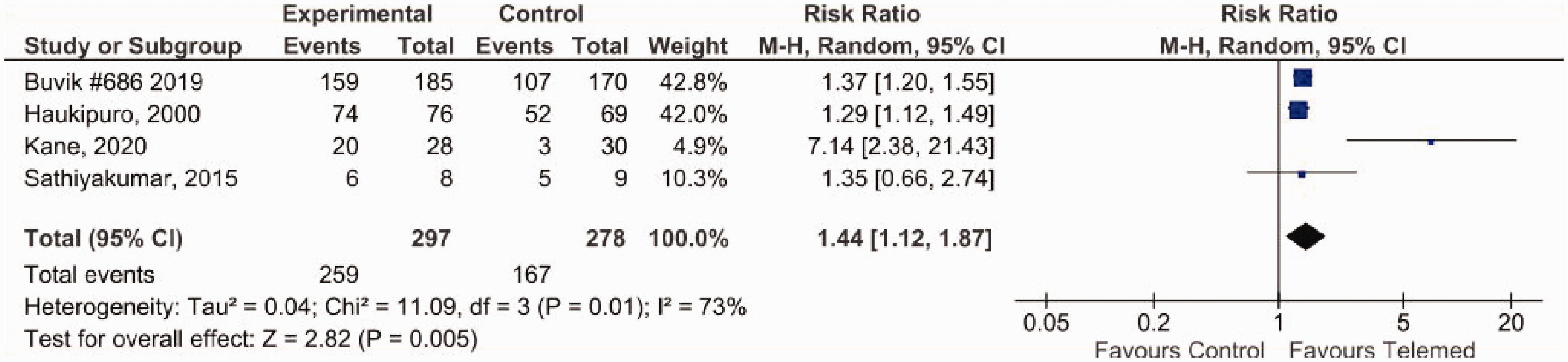
Risk ratio of patient preference for telemedicine vs control.

Mean difference in time spent with physician in telemedicine vs control.
Discussion
Widespread adoption of telemedicine has long been a challenge, facing resistance and criticism among many specialties, especially orthopaedics.4,18 The arrival of COVID-19 has pushed telemedicine to the forefront of clinical practice, shedding light on its applicability and transformative potential. 5 This review has demonstrated that there is strong evidence in favour of teleconsultation among orthopaedic patients, even beyond COVID-19.
Previous studies have demonstrated the importance of patient satisfaction in compliance with medical care.16,42 Most of the studies in this review (12) found no significant difference in patient satisfaction following teleconsultation when compared to traditional office visits. Interestingly, Wallace et al. 38 demonstrated an increase in satisfaction among telemedicine users largely attributed to shorter wait times. Considering that most of the literature has demonstrated shorter overall visit times as a result of teleconsultation, this suggests the potential for telemedicine to have a positive impact on the patient experience and enhance medical compliance.
When patients were asked their preference for consultation (i.e. telemedicine or in-office visit), an astounding 97% of patients in the telemedicine group preferred subsequent teleconsultations, 35 regardless of whether or not teleconsultation was used as an initial or follow-up appointment.34,35 Reasons in support of teleconsultation included ease of visit, convenience and its cost-saving capability.34,35 All but one study showed a reduction in healthcare-associated costs as a result of telemedicine. 38 Reasons for lower costs included reduced travel expenses such as transportation, parking fees and tolls; lower production loss from not having to take time off from work to attend appointments; and lower childcare costs associated with in-person visits. 32 It should not be overlooked that while travel costs were significantly lower in the telemedicine group, some studies still required patients to travel to a remote centre to conduct teleconsultation, therefore still incurring a small cost to the patient.32,33,35,37,38 Such findings suggest even greater savings, should the teleconsultation be conducted from the comfort of their home. However, one study 38 found an increase in hospital costs associated with the implementation of telemedicine technologies and annual maintenance fees, which may explain hospital resistance to telemedicine.
Our findings revealed that not only are patients generally accepting of telemedicine, but many surgeons also prefer its use over conventional office visits. 2 In regard to functional outcomes such as ROM, pain and QOL, no significant differences were found between teleconsultation and in-office visit groups,2,32–34,36,38,39 suggesting similar therapeutic efficacy between groups. In addition, no significant changes in long-term patient management plans were observed, indicating that teleconsultations are not inferior to office visits when it comes to diagnosing or managing orthopaedic conditions. 37
Our meta-analysis demonstrated that patients exposed to telemedicine are roughly 1.5 times more likely to prefer it for subsequent appointments over traditional office visits. This reinforces the natural inclination to prefer the comfort of the known rather than experiment with the unknown. 2 No significant differences in patient satisfaction, length of visit or time spent with the physician were determined between groups, suggesting that telemedicine is on an equal footing with traditional office visits in these respects.
A major limitation of this review was the small sample size due to a gap in the literature regarding orthopaedic telemedicine. This may explain the high heterogeneity obtained from our meta-analysis, indicating a considerable degree of variability across studies. Another explanation for the high heterogeneity may be attributed to the different scales used to assess functional outcome measures such as ROM, pain and QOL. It should be noted that many of the findings made by Wallace et al. 38 were not specific to orthopaedics, as they included other medical specialties in their research. As mentioned previously, a small number of studies conducted teleconsultation at remote medical centres,32,33,35,37,38 thereby increasing the likelihood of confounding variables. Lastly, because healthcare systems differ internationally, the results of this study may not be generalisable to regions that utilise different healthcare systems.
The findings of this review provided strong evidence to support the use of teleconsultation in orthopaedic surgery. While further research is needed to assess the ability of teleconsultation to replace traditional office visits, we believe that telemedicine can serve as an effective adjunct by providing a mechanism of triage and long-term continuity of care.4,5
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.