
Abstract
Coronavirus disease 2019 (COVID-19) has spread to nearly every continent, with over 2.6 m cases confirmed worldwide. Emergency departments care for a significant number of patients who are under investigation for COVID-19 or are COVID-19-positive. When patients present in the emergency department, there is an increased risk of spreading the virus to other patients and staff. We designed an emergency department telehealth program for patients physically in the emergency department, to reduce exposure and conserve personal protective equipment. While traditional telehealth is designed to be patient-specific and device-independent, our emergency department telehealth program was device-specific and patient-independent. In this article, we describe how we rapidly implemented our emergency department telehealth program, used for 880 min of contact time and 523 patient encounters in a 30-day period, which decreased exposure to COVID-19 and conserved personal protective equipment. We share our challenges, successes and recommendations for designing an emergency department telehealth program, building the technological aspects, and deploying telehealth devices in the emergency department environment. Our recommendations can be adopted by other emergency departments to create and run their own emergency department telehealth initiatives.
Introduction
Coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has spread throughout the world, with over 23.5 m cases currently. 1 Many hospitals and emergency departments (EDs) are facing increasing numbers of patients who are COVID-19 positive or are patients under investigation (PUIs) for COVID-19. 2 , 3 Although many patients with COVID-19 symptoms are not sick enough to be admitted to the hospital, when they present in the ED they increase the risk of spreading the virus to other patients. Repeat exposure to patients with COVID-19, despite proper personal protective equipment (PPE), may increase the risk for healthcare staff. 4 In April 2020, the CDC published that 9282 US healthcare workers have contracted the disease.5–8 Furthermore, each additional visit in a room may consume PPE, for which supplies may be limited. Lastly, nosocomial infection is also a concern with COVID-19. 9 , 10
Traditionally, telehealth has been used in the outpatient setting, to provide low-acuity care for patients. Many hospitals have adopted tele-neurology to evaluate patients for strokes as well as tele-psychiatry. 11 , 12 The use of telehealth has increased significantly over the past several years, from only 35% of US hospitals fully or partially implementing a telehealth system in 2010 to 75% in 2017. 13
During the COVID-19 pandemic, many specialities are utilising telehealth for their outpatient practices to decrease patient and clinician exposure, including internal medicine, orthopaedics, psychiatry and neurology.14–17 Telehealth has been used in EDs for virtual triage, 18 evaluation of strokes 19 and consultations. 20 However, telehealth for patients physically in the ED by ED providers has not yet been widely implemented. EDs see a majority of patients that come to a hospital and care for a large number of COVID-19 patients, many who initially present as undifferentiated. Telehealth initiatives – where patients and staff can be in different areas of the ED and communicate virtually – can decrease patient and staff exposure to COVID-19, decrease the use of PPE and improve patient and provider communication.
We rapidly deployed an ED telehealth program during the COVID-19 pandemic. Our approach to telehealth was unique – we used telehealth physically within the ED to evaluate and reassess patients, limit exposure and conserve PPE. While traditional telehealth is designed to be patient-specific and device-independent, our ED telehealth program was device-specific and patient-independent. In this article, we describe how we rapidly implemented our ED telehealth program.
Our institution
We are a large, suburban, level-1 trauma centre, nonprofit academic hospital in Long Island, New York, USA, with approximately 100,000 emergency department visits annually. Our hospital serves a county of 1.5 m people. We are at the epicentre of COVID-19 and have cared for several thousand of PUIs and COVID+ patients. In total, 30% of PUIs that arrive in our ED need to be admitted, with 10% needing intensive care unit (ICU) level of care immediately and another 15% who need these resources within 48 h. 21
Traditionally, our ED has 67 adult beds, nine paediatric beds and another 20–30 beds that can be placed in hallways. To rapidly increase our ED capacity during the COVID-19 pandemic, we opened a field tent in an offsite location from 11:00–23:00 daily, to treat low-acuity patients aged 15–65 years with symptoms suggestive of COVID-19. High risk patients and those <15 or >65 years old were treated in the main ED.
Our need for ED telehealth
As of 26 June 2020, 6623 patients have presented in our hospital with COVID-19 symptoms and many have been evaluated in the ED initially. Thus, ED staff have significant exposure to COVID-19 patients. Our ED staff include 40 attending physicians, 48 resident physicians, 19 advanced practice providers, 121 nurses and 65 clinical assistants. Many of these providers need to go into the room multiple times to communicate with patients (Figure 1).
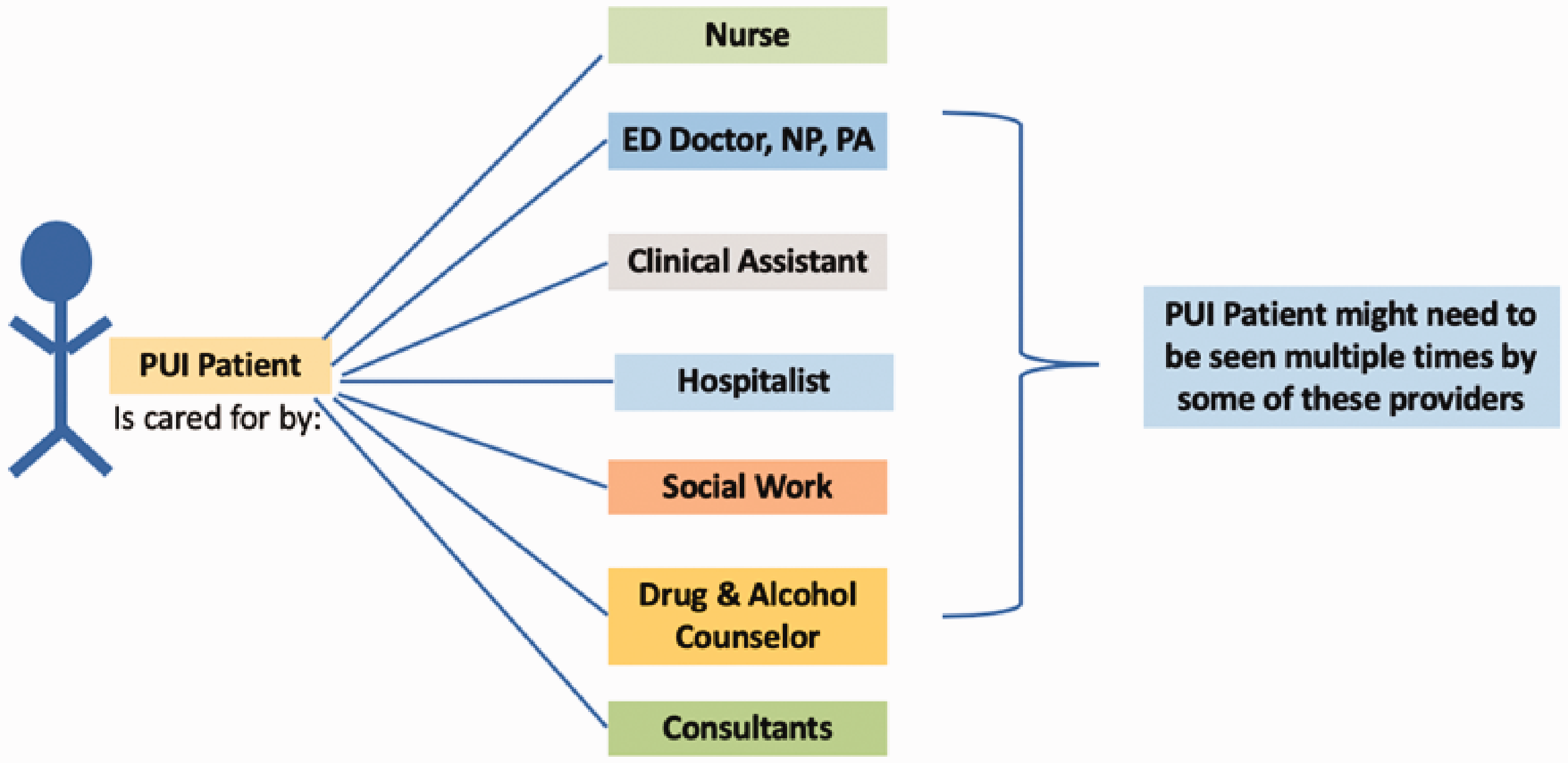
A patient under investigation (PUI) in the emergency department (ED) is cared for by multiple providers, some who need to see the patient multiple times during the ED visit.NP: Nurse Practitioners; PA: Physician Assistant.
To limit exposure and curb the spread of COVID-19 in our ED, we rapidly deployed an ED telehealth program for patients physically in our ED – for all patients, regardless of whether they were being admitted or discharged. Telehealth devices (iPads or iPod touches) were given to patients who were PUIs, when they were in an ED room. Patients who come to the main ED are often first evaluated in a single room, to allow for privacy. After the initial assessment by the ordering provider (generally a doctor, Nurse Practitioner (NP) or Physician Assistant (PA)) many of the remaining encounters could be performed through video-conferencing with ED staff. Nurses, clinical assistants, clerks, drug and alcohol counsellors, social workers, doctors, NPs and PAs all participate in the ED telehealth program to communicate with patients. In addition, consultant services and hospitalists also can call the patient’s ED telehealth device and evaluate the patient virtually.
Regulations
In the past, telehealth software was required to be compliant with the Health Insurance Portability and Accountability Act (HIPAA), which made it challenging and expensive to acquire. On 17 March 2020, the Office for Civil Rights (OCR), which is part of the Department of Health and Human Services, announced an enforcement discretion that it would waive ‘potential penalties for HIPAA violations’ for telehealth communications during the COVID-19 pandemic. 22 According to the OCR, patients and providers can communicate through any ‘non-public facing remote communication products’, including popular video chat applications. 23
Rapid implementation
Our objective was to create a telehealth program where providers and patients, physically in the ED, could communicate frequently while decreasing exposure to COVID-19 and conserving PPE.
Our institution had already been using Microsoft Teams, a chat-based collaboration platform, for outpatient telehealth visits. Our initial ED telehealth prototype involved patients downloading the Teams application (app) on their phone and ED staff booking online appointments with each patient. This model, however, had a few problems: providers found it time-consuming to book appointments for each ED patient and patients had difficulty downloading the app due to guest Wi-Fi speed, forgetting their passwords and email access issues.
While traditional telehealth is designed to be patient-specific and device-independent, we found that this model did not work for patients already in the ED. Instead, we developed an ED telehealth program that was device-specific and patient-independent. The Teams application has a video chat feature, where one can have a video call with another individual who is also using the app. We decided to utilise this feature for the ED telehealth program.
When patients arrived in the ED, we gave them ED telehealth devices (such as iPods and iPads) that already have Teams downloaded on them. Each device had its own name on Teams and the provider could connect to the patient by searching for the device name. The provider clicks the ‘call’ button and the patient’s device will ring, similar to a phone call on a smart phone. When the patient answers, they are connected to a video chat with their provider (Figure 2).
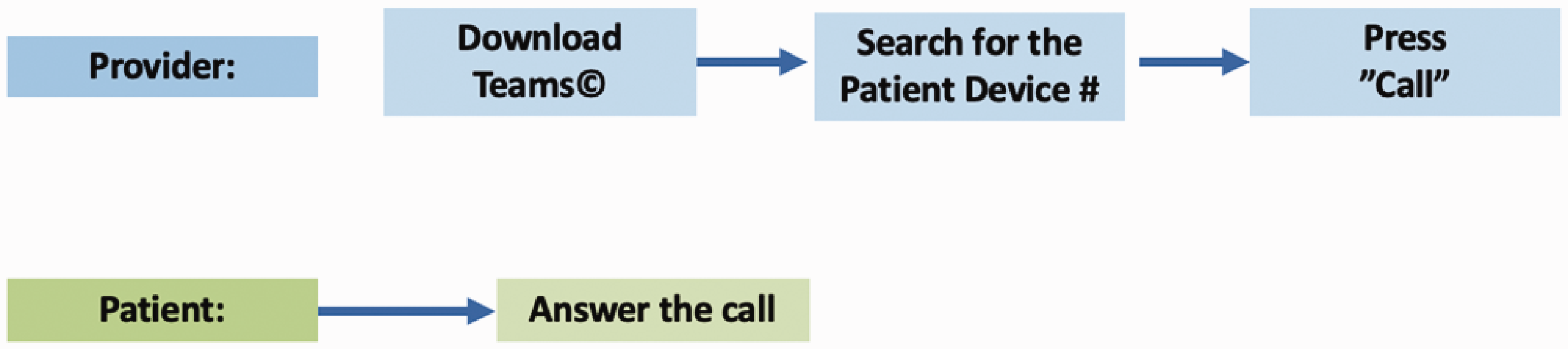
Creating emergency department (ED) telehealth visits in the final prototype.
Technological implementation
Microsoft Teams is a desktop and mobile app (for iOS and Android) that is part of the Office 365 suite and is a platform for chat-based communication. Teams communications data are encrypted in transit and at rest. 24 In our ED, providers use their own mobile devices and download the Teams app, signing in with their institutional login. We chose to do this because we wanted to save the ED telehealth devices for patients.
The ED telehealth devices for patients are iPod touches or iPads (Apple Inc., Cupertino, California, USA; iOS 13). We connected these devices to our Apple Development Enrollment Program (DEP) portal, which allows us to enrol and configure our Apple devices. These devices are connected to our mobile device management application, MDM Jamf Pro, which allows us to restrict software, enforce encryption and customise security settings. We allowed the ED telehealth devices to only have one main app, Teams. In addition, the devices are connected to a secure Wi-Fi connection, which is permanent and managed.
Donation of devices
We made a short video (<1 min) about our ED telehealth experience, which explained how and why we were using the ED telehealth as well as showed a sample patient-provider telehealth encounter. Our hospital launched a call for donation of iPads and this video was published on our institutional social media sites to help illustrate how we are using Telehealth to connect. Through the call for donations, our hospital received 232 iPad donations, which were used for connecting patients with their providers or their families.
ED deployment
We chose to launch the telehealth initiative, with 45 telehealth devices, in our Acute Care zones because they had the greatest number of PUIs. There are two Acute Care Zones in the ED and for each zone, we placed iPods and iPads by the lead nurse’s desk (located in the zone) and the devices were signed out for PUIs. The devices were cleaned using Super Sani-Cloth Disinfectant Germicidal Wipes or an equivalent, which were approved by our hospital’s infection control team.
The patients keep the ED telehealth devices for their entire ED stay, allowing multiple providers, including nurses, doctors, PAs, NPs, social workers, alcohol and drug counsellors, hospitalists and consultants, to connect with the patient. After the first week, we placed the telehealth devices on stands in patient rooms for ease of use.
Education for providers
To educate our providers about the ED telehealth, we sent out an email to all ED staff about how to use the devices. In addition, we attached a video of how to download and use Teams. We also enlisted ‘ED telehealth champions,’ a group of three ED residents, to help with teaching ED staff about how to use the devices.
Language and translation
Approximately 30% of our PUIs are Hispanic/Latino and many speak Spanish as their first language. We have certified translators at our institution that also use Microsoft Teams. When a provider is speaking with a patient using Teams video conference, they can add the translator to the conference, resulting in a three-way conversation. In addition, using Teams, an outside phone number can be called, such as the number for the language interpreter services.
Our experience
In our ED, a provider (usually a doctor, NP or PA) initially evaluates the patient in person and all subsequent encounters (i.e. updating the patient, answering the patient’s questions, reassessing the patient) may be performed through the ED telehealth devices. Some of our social workers, drug and alcohol counsellors, hospitalists and consultants complete their entire evaluation using ED telehealth. Patients can also call their providers using the app. Our telehealth program was used for 880 min of call time and 523 encounters (465 calls and 58 messages) in a 30-day period. This helped limit exposure to PUIs and COVID+ patients and conserved PPE, such as gowns, gloves and masks.
Based on our experience, we recommend the following for others planning to rapidly deploy telehealth within their EDs:
Telehealth model
For communicating with patients within the physical ED, we suggest providing patients with telehealth devices to reduce the number of steps patients needed to download and sign-in to the telehealth program.
Hardware
Telehealth devices can be tablets, phones or other Wi-Fi-enabled devices (i.e. iPods). We recommend devices that are cost-effective for your ED and also suggest a request for donations from the community.
Software
Under the COVID-19 OCR enforcement discretion, popular video chat platforms can be used. We recommend choosing a chat service with end-end encryption that can also provide HIPAA compliant video communication.
Security
We suggest using device management software for ED telehealth devices to create security settings and enforce encryption for devices given to patients.
Education
We recommend education to providers about how to use the devices and troubleshooting. In addition, staff should educate patients how to use the device – consider using educational videos (in multiple languages) and posters or signs.
Sanitation
We recommend working with your hospital’s infection control team to decide how to clean and store the ED telehealth devices.
Language and translation
If in-person translators are available, they can download the app your ED is using for telehealth services and connect to a patient-provider call. There are also third party translation services that can be connected by dialling a phone number.
Limitations
This initiative took place in a large, academic medical centre at the epicentre of COVID-19 in the USA. Other hospitals and institutions that are in different geographical locations may have different experiences. This project also relied on institutional and community support to acquire ED telehealth devices.
Conclusion
There has been a dramatic increase in COVID-19 cases around the world. ED patients and staff are exposed to the virus and ED telehealth can decrease exposures, conserve PPE and improve communication between patients and providers. In this article, we discussed our rapid deployment of a successful ED telehealth program. Our experiences can be used by other EDs and hospitals to create and run their own ED telehealth initiatives.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.