
Abstract
Introduction
The aim of this review was to systematically evaluate the available evidence on the effectiveness of internet-based telerehabilitation among patients after total joint arthroplasty regarding pain, range of motion, physical function, health-related quality of life, satisfaction, and psychological well-being.
Methods
This was a systematic review with meta-analysis based on the Cochrane Handbook for Systematic Reviews of Interventions guidelines. Studies published in English or Chinese were searched using defined search periods, databases, and search terms. Two reviewers assessed independently the quality of studies. RevMan 5.3 was used for meta-analysis. Heterogeneity was assessed using the χ2 and I2 statistic. A random effect model and mean difference (MD) with 95% confidence interval (CI) was adopted. Standardised mean difference (SMD) was used if the outcome was measured by different scales.
Results
Eleven studies with 1020 participants were analysed. Compared to face-to-face rehabilitation, internet-based telerehabilitation showed no significant difference in outcomes of pain (SMD–0.11, 95% CI–0.32 to 0.10), range of motion in flexion (MD 0.65, 95% CI–1.18 to 2.48) and extension (MD–0.38, 95% CI–1.16 to 0.40), patient-reported physical function (SMD 0.01, 95% CI–0.15 to 0.17), health-related quality of life (SMD–0.09, 95% CI–0.26 to 0.07), satisfaction (SMD–0.04, 95% CI–0.21 to 0.14), and psychological well-being (SMD 0.10, 95% CI–0.13 to 0.33). Internet-based telerehabilitation showed better outcomes in physical functional tests (SMD–0.54, 95% CI–1.08 to–0.01).
Discussion
This review suggests that internet-based telerehabilitation has comparable effectiveness to face-to-face rehabilitation on rehabilitation outcomes among patients after total joint arthroplasty.
Keywords
Introduction
Total joint arthroplasty (TJA) is an effective operation to treat end-stage osteoarthritis, and it mainly occurs in older populations. 1 Due to the ageing of the population and the increase in the prevalence of osteoarthritis, the incidence of TJA has increased globally. 2 Demand for post-operative rehabilitation is rapidly growing and is challenging the sustainability of face-to-face rehabilitation services. 3 Technology advancements have led to telerehabilitation supplementing or providing an alternative to face-to-face rehabilitation to meet this increasing demand for the rehabilitation of patients after TJA. 4
Telerehabilitation refers to delivering rehabilitation services via information and communication technologies that are internet-based, such as videoconferencing, or non-internet-based, such as using the telephone.5–7 Telerehabilitation increases the accessibility of rehabilitation services, especially for those who live in remote areas with limited healthcare availability 8 or during a special period such as the COVID-19 pandemic. 9 For patients who have more pain and limited mobility right after surgery, telerehabilitation helps to maintain the continuity of care by enabling patients to access rehabilitation services at home. 3 , 6 With telerehabilitation, patients after TJA can exercise in a familiar home environment, which helps reduce patients’ stress and increase their satisfaction. 6 , 10
The effectiveness of telerehabilitation among patients after TJA has been synthesised by recent systematic reviews. 3 , 4 , 8 , 11 , 12 These reviews reported that telerehabilitation was as effective as face-to-face rehabilitation in relieving pain, as well as in improving range of motion (ROM) and physical function. However, these reviews reported outcomes from two forms of telerehabilitation: internet-based and non-internet-based. No review has specifically evaluated the effectiveness of internet-based telerehabilitation. With the rapid development of the internet, technologies such as videoconferencing and mobile applications (apps) are increasingly being used in telerehabilitation. These technologies enable the demonstration of exercises as well as verbal and visual interactions. 13 Patients can learn about rehabilitation repeatedly at any time and location. 14 The effectiveness of internet-based telerehabilitation should be synthesised to support evidence-based practice.
Previous systematic reviews focused on pain, ROM, and physical function as rehabilitation outcomes. The expert consensus on best practice in rehabilitation after TJA suggests that rehabilitation outcomes should include not only body structure/function (e.g. pain and ROM) and activity/participation (e.g. physical function), but also other outcomes such as health-related quality of life (HRQoL) and patients’ satisfaction with rehabilitation outcomes/process. 15 Additionally, psychological well-being outcomes have been recommended because many patients after arthroplasty experienced psychological problems such as anxiety and depression.16–18 Thus, in addition to pain, ROM, and physical function, other outcomes such as HRQoL, satisfaction, and psychological well-being should be included to gain a holistic understanding of the effectiveness of internet-based telerehabilitation.
This review aimed to systematically evaluate the available evidence on the effectiveness of internet-based telerehabilitation among patients after TJA regarding pain, ROM, physical function, HRQoL, satisfaction, and psychological well-being.
Methods
Study design
This was a systematic review with meta-analysis following the methods in the Cochrane Handbook for Systematic Reviews of Interventions. 19 The process and results were reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (PRISMA). 20
Literature search strategy
Trials published in English or Chinese were searched from the following computerised databases from inception to 14 May 2020: PubMed, CINAHL® Complete, EMBASE, Cochrane Library, Scopus, Web of Science, Joanna Briggs Institute EBP Database, PsycINFO®, Physiotherapy Evidence Database, Directory of Open Access Journals, ProQuest Databases, SPORTDiscus with Full Text, Academic Search Ultimate, Centre for Reviews and Dissemination, China National Knowledge Infrastructure, and Wanfang Data. Hand searching was performed by scanning the reference lists of included studies.
The search terms were: arthroplast*, joint replacement, telerehabilitat*, “tele rehabilitat*”, telemedicine, telehealth, “tele health”, e-health, eHealth, mHealth, “mobile health”, “digital health”, “digital physiotherapy”, “AI-powered rehabilitat*”, “remote consultation”, “remote rehabilitat*”, videoconferencing, internet.
The inclusion criteria were: (1) participants were adults (≥18 years) after primary TJA; (2) the post-operative rehabilitation program was delivered via the internet, such as videoconferencing, interactive virtual system, mobile apps, and email; (3) the comparison was conventional care, such as face-to-face outpatient rehabilitation, home-visit, or usual care; (4) the outcomes consisted of at least one of the following: pain, ROM, physical function, HRQoL, satisfaction, psychological well-being; and (5) the study design was a randomised controlled trial (RCT).
Studies were excluded if: (1) they focused on revision, unicompartmental or bilateral joint replacement; (2) the intervention adopted non-internet technologies (e.g. using the telephone and short message services), merged both internet-based and non-internet-based forms, combined face-to-face rehabilitation and telerehabilitation, or were telecommunications between health professionals; (3) the comparison was an alternative telerehabilitation such as using the telephone; (4) the outcomes of TJA could not be separated from that of other surgical procedures; and (5) articles were abstracts or conference posters.
Search outcomes
Initially, 1351 records were found. After duplicates were removed, 601 records were screened by two independent researchers (QW and SWC) on the titles and abstracts. Inconsistencies were discussed until a consensus was reached. A total of 586 records were excluded. The full texts of 15 remaining studies were assessed against the eligibility criteria. Four studies were further excluded. The remaining 11 full-text studies were appraised for methodological quality and none were excluded. A manual search was conducted by screening the reference lists of the included studies, and no further studies were obtained. All included studies were published in English. No Chinese literature was included as it could not meet the inclusion criteria. The PRISMA flow diagram 20 is presented in Figure 1.
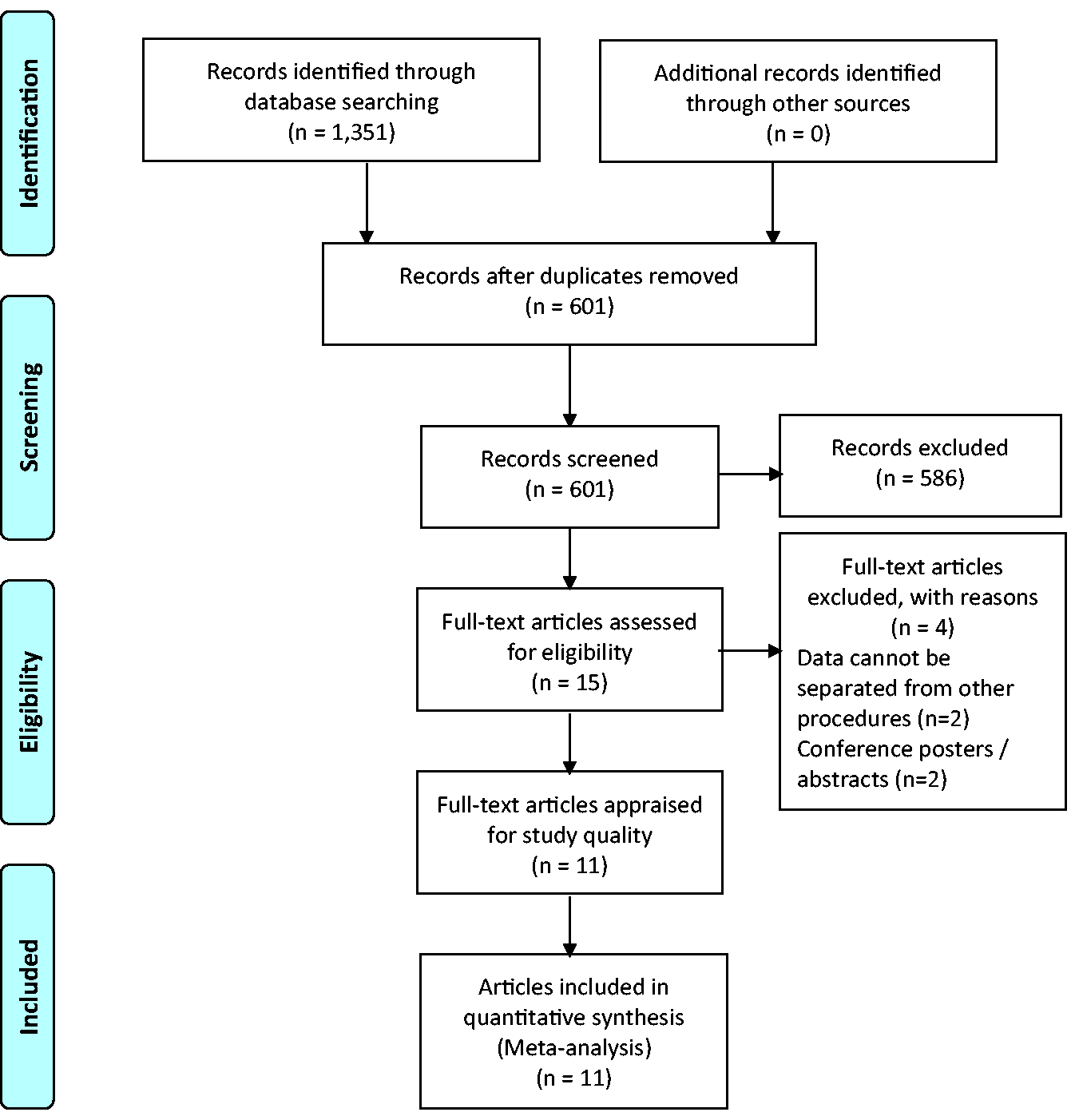
PRISMA flow diagram for study selection.
Methodological quality assessment
The methodological quality of the included studies was assessed using the Joanna Briggs Institute Critical Appraisal Tools: Checklist for Randomised Controlled Trials. 21 This checklist includes 13 items, and for each item, there are four possible appraisal results: yes, no, unclear, or not applicable.
Two researchers (QW and SWC) appraised each included study independently. The discrepancy was resolved by discussion until reaching a consensus. In the appraisal results, each “yes” was assigned one point and the total score of each study was calculated. The study was considered poor quality if its score was less than six (i.e. half of the maximum), moderate quality if between six and nine (i.e. 50–75% of the maximum), and good quality if it scored 10 and above. Studies with poor quality were to be excluded. Out of the 11 studies, seven were rated as good quality and four moderate quality (Table 1). No studies were excluded.
Summary of quality appraisal for included studies.
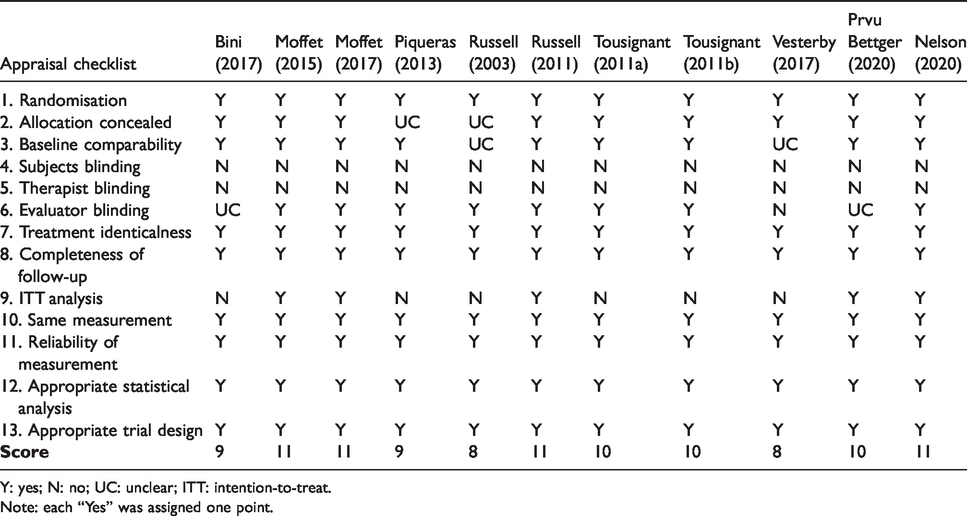
Y: yes; N: no; UC: unclear; ITT: intention-to-treat.
Note: each “Yes” was assigned one point.
Data extraction and analysis
A data extraction sheet was created based on the Cochrane Handbook guidelines. 22 The extracted data included author, year of publication, country, participants (e.g. sample size, age, gender, and surgery), intervention (e.g. delivery medium, session, duration, frequency, and follow-up), comparison, outcome measures, and key findings.
The Cochrane Collaboration’s Review Manager Software (RevMan 5.3) was used for meta-analysis. The results from the intention-to-treat (ITT) analyses were preferentially pooled. Heterogeneity among the included studies was assessed using the χ2 and I2 statistic. A P-value of no more than 0.05 or I2 value greater than 50% was considered substantial heterogeneity. If the heterogeneity was substantial, the sensitivity analysis was conducted to assess the impact of individual study. A random effect model was adopted in this review. As the outcomes were continuous data, a mean difference (MD) with 95% confidence interval (CI) was adopted in the effect size analysis. For outcomes measured by different scales, MD was replaced by standardised mean difference (SMD).
Results
Characteristics of studies
Eleven studies were included in this review. The studies were conducted in Canada (n = 4), Australia (n = 3), the USA (n = 2), Spain (n = 1), and Denmark (n = 1). Nine studies focused on total knee arthroplasty (TKA) while two on total hip arthroplasty (THA). A total of 1020 arthroplasty patients (877 TKAs and 143 THAs) were recruited in these studies. Their mean age was 66.6 years, and the majority were females (58.7%). The characteristics of the included studies are presented in Table 2.
Characteristics of the included studies.

TKA: total knee arthroplasty; VAS: Visual Analogue Scale; VR12: Veterans-RAND 12-Item Health Survey; KOOS-PS: the Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form; ROM: range of motion; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index; KOOS: Knee Injury and Osteoarthritis Outcome Score; HCSQ: Health Care Satisfaction Questionnaire; TUG: timed up-and-go test; PSFS: Patient-Specific Functional Scale; SQLU: Spitzer Quality-of-Life Uniscale; SMAF: Functional Autonomy Measurement System; SF36: 36-Item Short Form Health Survey; HSQ: Healthcare Satisfaction Questionnaire; THA: total hip arthroplasty; OHS: Oxford Hip Score; PROMIS: Patient-Reported Outcomes Measurement Information System; HOOS: Hip disability and Osteoarthritis Outcome Score; SF12: 12-Item Short Form Health Survey.
*The study reported the mean age of each group rather than that of total population.
#EQ-5D is the name of instrument rather than an acronym. EQ-5D-3L has three levels of responses for each item, while EQ-5D-5L has five levels.
The delivery mediums for telerehabilitation varied: six studies used videoconferencing,23–28 two used mobile apps, 29 , 30 one used the Virtual Exercise Rehabilitation Assistant, 31 one used Interactive Virtual Telerehabilitation, 32 and another used videoconferencing combined with a resource package. 33 The intervention commenced on the day after surgery (n = 1), immediately after hospital discharge (n = 2), one week after discharge (n = 7), and two weeks after discharge (n = 1). Seven studies conducted 45 to 60 minutes’ rehabilitation per session and the other four had no time limit on the session.29–31, 33 The frequency of rehabilitation exercises varied across studies: daily (n = 2), weekly (n = 2), biweekly (n = 4), and no limit (n = 3). Three studies did not have longer-term follow-up of the participants after interventions,25–27 while eight studies followed up at three months (n = 3), four months (n = 3), six months (n = 1), and six and 12 months (n = 1) post-operatively.
Risk of bias of studies
Table 1 summarises the assessment of the methodological quality of the included studies. All studies were rated as having adequate randomisation, treating groups identically, having complete follow-up, measuring outcomes in the same way for groups, having reliable measures, and adopting appropriate statistical analysis and trial design. However, none of the included studies blinded the participants or the therapists who delivered telerehabilitation. Outcome assessors were blinded in eight studies, while two 29 , 31 did not describe assessor blinding and one 33 could not establish blinding. Five of 11 studies adopted the ITT principle in data analysis,23–25, 30 , 31 but the other six did not. The methods used for allocation concealment were not described in two studies. 26 , 32 The baseline comparability regarding demographic characteristics and outcomes cannot be distinguished in two studies. 26 , 33
Outcomes
In this review, the effectiveness of internet-based telerehabilitation for TJA was determined by six outcomes, including pain, ROM, physical function, HRQoL, satisfaction, and psychological well-being.
Pain
Six studies measured patients’ pain. Meta-analysis showed no significant difference between the experimental and control groups regarding the reduction of pain scores from baseline, either at the completion of interventions (SMD–0.11, 95% CI–0.32 to 0.10, P = 0.30, six RCTs, 794 participants) or at follow-up (SMD 0.01, 95% CI–0.15 to 0.17, P = 0.88, four RCTs, 691 participants). The heterogeneity was acceptable (I2 = 48% and 8%, respectively) (see Figure 2).
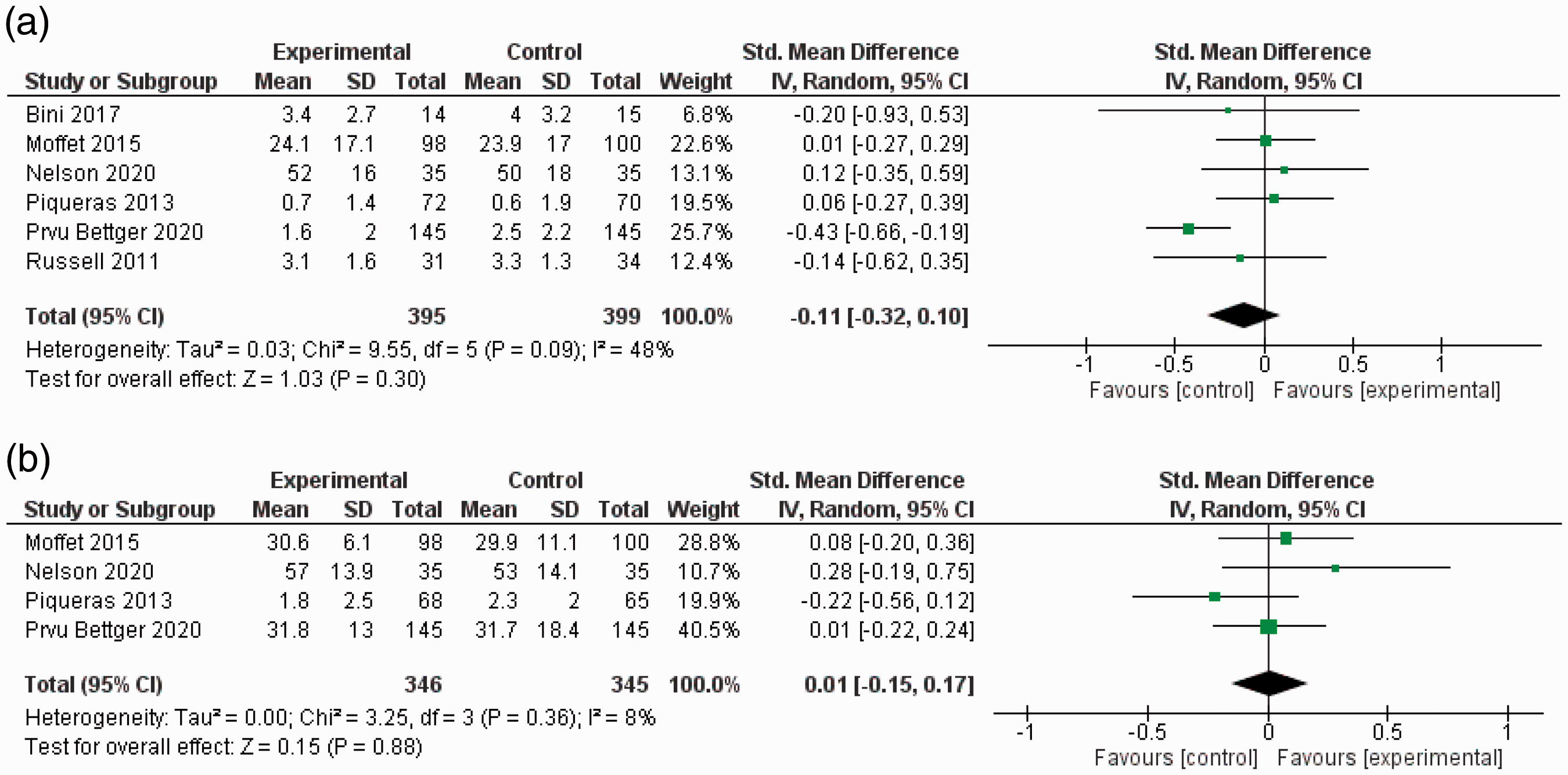
Meta-analysis of the change from baseline in pain scores. (a) Change from baseline in pain scores at the completion of interventions; (b) change from baseline in pain scores at follow-up.
ROM
Four studies measured the ROM of knee. At the completion of interventions, the improvements were similar in the experimental and control groups, regarding flexion degrees (MD 0.65, 95% CI–1.18 to 2.48, P = 0.48, four RCTs, 446 participants) and extension degrees (MD–0.38, 95% CI–1.16 to 0.40, P = 0.34, four RCTs, 446 participants). There was no heterogeneity (I2 = 0%). Similar results were found at follow-up (flexion: MD 1.16, 95% CI–1.25 to 3.57, P = 0.35, three RCTs, 372 participants, I2 = 0%; extension: MD 0.31, 95% CI–0.56 to 1.18, P = 0.49, three RCTs, 372 participants, I2 = 0%) (see Figure 3).
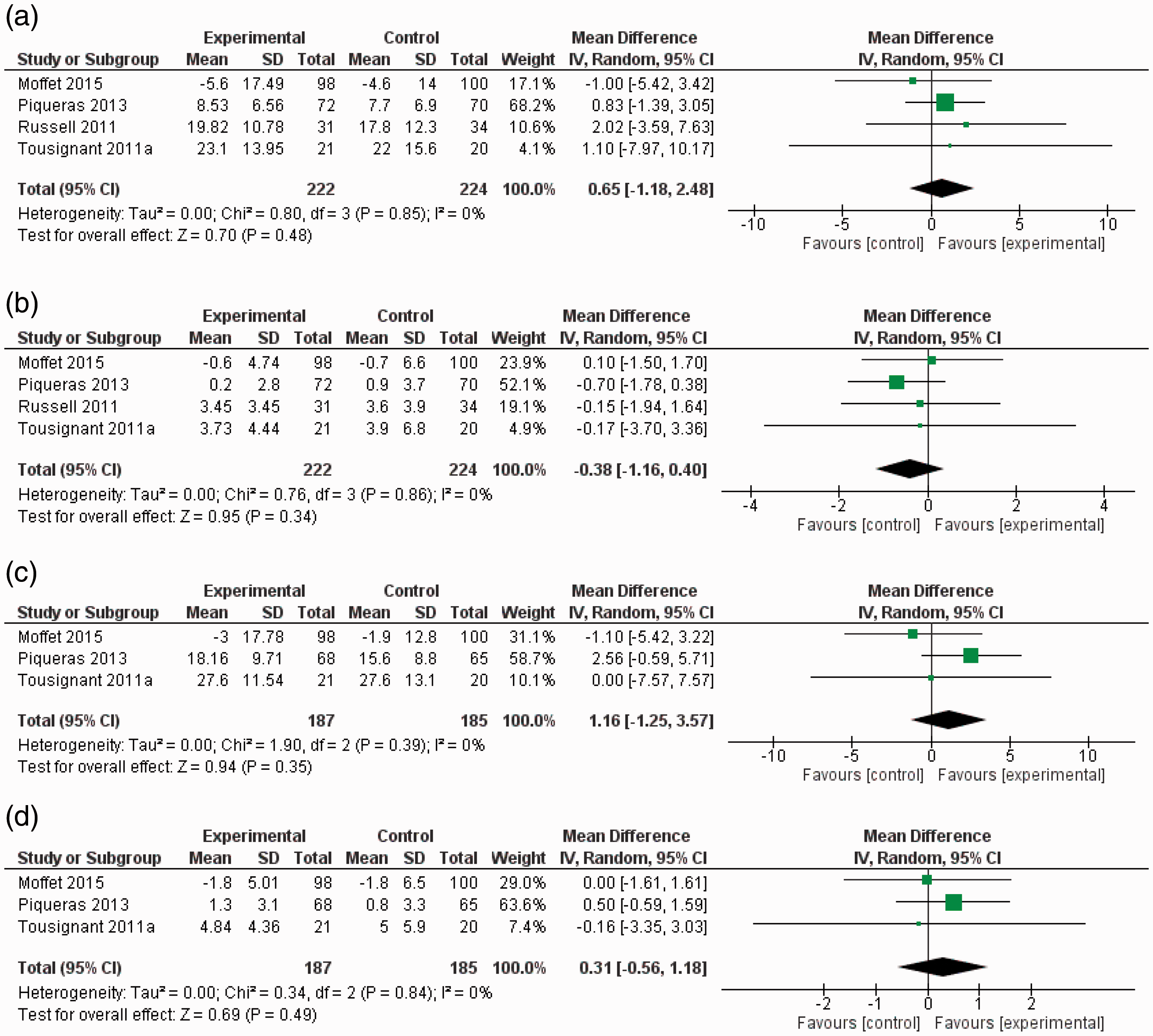
Meta-analysis of the change from baseline in range of motion. (a) Change from baseline in ROM (flexion) at the completion of interventions; (b) change from baseline in ROM (extension) at the completion of interventions; (c) change from baseline in ROM (flexion) at follow-up; (d) change from baseline in ROM (extension) at follow-up.
Physical function
In terms of physical function recovery, patients’ performance in validated tests (e.g. timed up-and-go test) and self-reported outcomes were analysed. The change in physical function from baseline in five studies that used validated tests was pooled. The experimental groups achieved better outcomes than control at the completion of interventions (SMD–0.54, 95% CI–1.08 to–0.01, P = 0.05, five RCTs, 547 participants, I2 = 89%). No significant difference was found at follow-up (SMD 0.13, 95% CI–0.27 to 0.52, P = 0.53, three RCTs, 401 participants, I2 = 73%) (see Figure 4). Due to substantial heterogeneity, one study was removed at a time from the analysis to detect its impact. The heterogeneity became insignificant after the removal of one RCT. 32 The results remained similar after this removal: at the completion of interventions (SMD–0.23, 95% CI–0.43 to–0.04, P = 0.02, four RCTs, 405 participants, I2 = 0%), and at follow-up (SMD–0.06, 95% CI–0.30 to 0.18, P = 0.60, two RCTs, 268 participants, I2 = 0%).
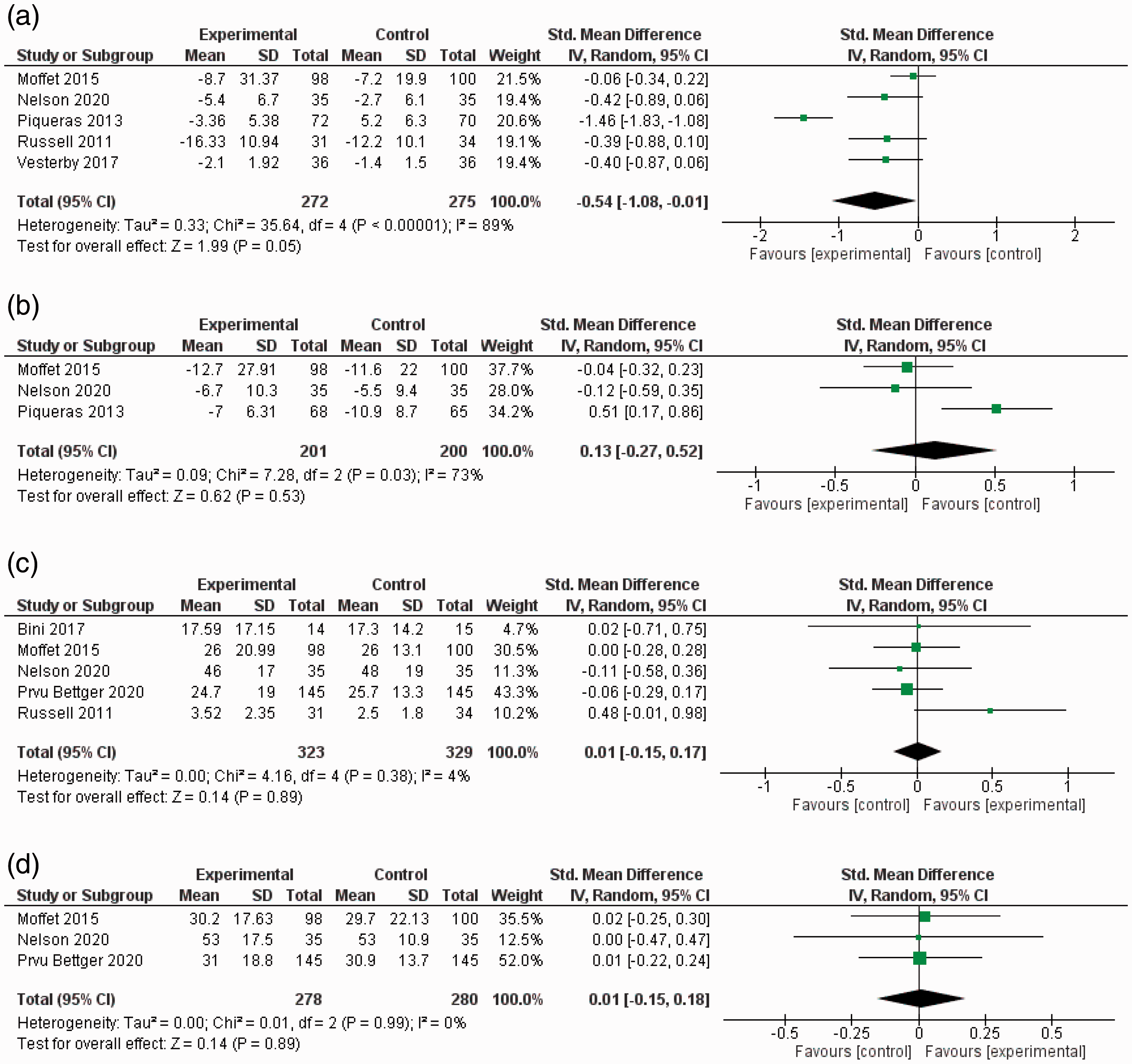
Meta-analysis of change from baseline in physical function. (a) Change from baseline in physical function tests at the completion of interventions; (b) change from baseline in physical function tests at follow-up; (c) change from baseline in self-reported scales at the completion of interventions; (d) change from baseline in self-reported scales at follow-up.
Five studies provided the data of patient-reported physical function improvements. Meta-analysis did not show between-group difference, either at the completion of interventions (SMD 0.01, 95% CI–0.15 to 0.17, P = 0.89, five RCTs, 652 participants, I2 = 4%) or at follow-up (SMD 0.01, 95% CI–0.15 to 0.18, P = 0.89, three RCTs, 558 participants, I2 = 0%) (see Figure 4).
HRQoL
Five studies reported HRQoL. Compared to the control groups, the experimental groups showed no significant difference in the change from baseline, at the completion of interventions (SMD–0.09, 95% CI–0.26 to 0.07, P = 0.26, five RCTs, 652 participants) and at follow-up (SMD 0.09, 95% CI–0.07 to 0.24, P = 0.28, four RCTs, 630 participants). The studies had no substantial heterogeneity (I2 = 7% and 0%, respectively) (see Figure 5).

Meta-analysis of change from baseline in health-related quality of life. (a) Change from baseline in HRQoL at the completion of interventions; (b) change from baseline in HRQoL at follow-up.
Satisfaction
Six studies assessed patients’ satisfaction with rehabilitation outcomes/process, and three of them compared the results between the experimental and control groups. Meta-analysis showed that there was no significant between-group difference (SMD–0.04, 95% CI–0.21 to 0.14, P = 0.67, three RCTs, 512 participants) and heterogeneity was not substantial (I2 = 0%) (see Figure 6).

Meta-analysis of satisfaction level after interventions.
Psychological well-being
Four studies reported the outcomes on psychological well-being. One study 33 measured patients’ anxiety using the Visual Analogue Scale. Three studies used the self-report Mental Health Component sub-scores (MCS) in Veterans-RAND 12-Item Health Survey, 29 12-Item Short-Form Health Survey, 30 and Patient-Reported Outcomes Measurement Information System. 31 The experimental and control group achieved similarly significant reductions in anxiety after intervention. 33 The improvement of MCS in three studies was pooled and no significant between-group difference was found (SMD 0.10, 95% CI–0.13 to 0.33, P = 0.39, three RCTs, 389 participants). The heterogeneity was not substantial (I2 = 11%) (see Figure 7).

Meta-analysis of change from baseline in mental health component scores.
Discussion
This systematic review presented the available evidence on the effectiveness of internet-based telerehabilitation among patients after TJA regarding pain, ROM, physical function, HRQoL, satisfaction, and psychological well-being. The present review focused on internet-based telerehabilitation, which differed from previous reviews that included both internet-based and non-internet-based forms of telerehabilitation. This review generated new knowledge on the effectiveness of internet-based telerehabilitation.
The present review compared the improvement of HRQoL pre- and post-interventions based on the data of five RCTs. 24 , 25 ,29–31 No significant between-group difference was found. To the best of our knowledge, this is the first meta-analysis that included HRQoL as an outcome in telerehabilitation among patients after TJA. Previous reviews described improvements of HRQoL in telerehabilitation among patients with knee osteoarthritis 11 and after arthroplasty, 34 but none had conducted meta-analysis due to the insufficient data obtained from the included studies. The meta-analysis in the present review consolidates previous evidence by providing a more precise estimation of the effectiveness of telerehabilitation on HRQoL compared to face-to-face rehabilitation. 35 Patients’ perceived health after TJA is not only attributed to improvements in clinical symptoms but also psychological well-being, social relationships, and environments. 36 , 37 The outcomes of HRQoL represent patients’ overall health and they can be used to assist clinical decision-making for patients after TJA. 38 Thus, HRQoL is recommended as one of the outcome measures when evaluating patients’ rehabilitation after TJA. 15
The present review pooled the MCS of patient-reported measures in three RCTs and found that internet-based telerehabilitation is comparable to face-to-face rehabilitation regarding improvement of patients’ psychological well-being. These findings suggest that internet-based telerehabilitation has potentially positive effects on psychological well-being. Such findings contribute to a holistic understanding of the effectiveness of internet-based telerehabilitation. Poor psychological well-being or psychological problems are experienced by many patients after arthroplasty, 17 , 18 and these problems negatively impact patients’ rehabilitation outcomes such as pain and joint function. 39 , 40 However, only four reviewed studies included psychological well-being as an outcome. Future studies could include psychological well-being as one of the outcome measures to comprehensively understand the effects of telerehabilitation.
Patient satisfaction is another important healthcare outcome when evaluating telerehabilitation. 23 Previous reviews showed that TJA patients were highly satisfied with the technical features and communication pattern in telerehabilitation. 4 The present review found that patients had high levels of satisfaction using internet-based telerehabilitation, which was comparable to face-to-face rehabilitation. The included RCTs reported that patients who used telerehabilitation were satisfied with their recovery in physical activities, their relationships with healthcare professionals, and the delivery and organisation of the programs. 23 , 27 , 31 Some patients preferred internet-based telerehabilitation to face-to-face rehabilitation because it had the advantage of eliminating transportation time and providing “personalised” treatment. 6 , 10
The present review found that internet-based telerehabilitation had similar effectiveness with face-to-face rehabilitation on the outcomes of pain, knee ROM, and patient-reported physical function. These findings varied from previous reviews that reported that telerehabilitation had better outcomes in pain relief, 34 knee extension degree, 12 and patient-reported physical function. 11 Compared with previous reviews, the present review focused on RCTs investigating internet-based telerehabilitation and did not include non-randomised trials 11 or non-internet-based telerehabilitation forms such as using the telephone. 11 , 34 Further, the present review was based on a larger number of studies and participants, which increased the power of the meta-analysis. 41 The results of the present review provide a high level of evidence on the effectiveness of internet-based telerehabilitation on pain, ROM, and physical function.
Although the quality of the included studies was from moderate to good, some methodological quality issues were observed. Blinding was not possible for participants or healthcare providers in the included studies as they both knew the mode of rehabilitation that participants received. Awareness of group assignment might influence participants’ behaviour in the trial, such as compliance with the intervention or participants’ response to outcome measures. 42 Healthcare providers with the knowledge of group assignment may treat the participants differently. 43 Six out of 11 studies did not adopt the ITT principle in their analyses. This might lead to an overestimated efficacy of the intervention by removing non-compliers and dropouts from the final analysis. 44 It might also reduce the statistical power since the sample size decreases after excluding non-compliers and dropouts. 44
Despite the methodological limitations, the present review suggests that internet-based telerehabilitation is as effective as face-to-face rehabilitation in improving pain, ROM, physical function, HRQoL, satisfaction, and psychological well-being in patients after TJA. This review provides the aggregated evidence on HRQoL, psychological well-being, and satisfaction, which were not mentioned in previous similar reviews.
Limitations
Internet-based telerehabilitation is a multi-component intervention, which includes various services such as treatment, consultation, and education. This review did not analyse the specific efficacy of each service. Only trials published in English or Chinese were searched because the authors can only understand these two languages. Relevant studies published in other languages might be excluded.
Implications for practice and research
Internet-based telerehabilitation appears to be a promising alternative for patients after TJA, especially for those who are not able to participate in face-to-face rehabilitation services due to geographic distance, physical impairment, and pandemic isolation. Healthcare providers could have more confidence in using internet-based telerehabilitation with the evidence provided by this review. Psychological well-being and HRQoL should be included in the outcome measures of future studies. Although double-blinding may not be possible, assessor blinding should be used in future studies to reduce bias. ITT analysis should be adopted in future studies.
Conclusion
In this systematic review with meta-analysis, internet-based telerehabilitation showed comparable effectiveness with face-to-face rehabilitation for the patient after TJA regarding pain, ROM, physical function, HRQoL, satisfaction, and psychological well-being. This review supports the use of internet-based telerehabilitation for patients after TJA.
Supplemental Material
sj-pdf-1-jtt-10.1177_1357633X20980291 - Supplemental material for The effectiveness of internet-based telerehabilitation among patients after total joint arthroplasty: A systematic review and meta-analysis of randomised controlled trials
Supplemental material, sj-pdf-1-jtt-10.1177_1357633X20980291 for The effectiveness of internet-based telerehabilitation among patients after total joint arthroplasty: A systematic review and meta-analysis of randomised controlled trials by Qingling Wang, Regina L-T Lee, Sharyn Hunter and Sally W-C Chan in Journal of Telemedicine and Telecare
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.