
Abstract
Introduction
Telehealth service provision has accelerated during the Coronavirus disease 2019 (COVID-19) pandemic. As the pandemic continues, clinical practices have discovered ways to resume operations. Opportunities exist to understand patient preferences for telehealth clinical services and to tailor offerings to different demographic groups.
Methods
We conducted a survey of patients receiving telehealth services through our outpatient practice to understand the types of healthcare services for which patients report preferences for telehealth.
Results
We received 551 survey responses (response rate = 20.8%; 551/2650). More than half of patients indicated being ‘very likely’ to use telehealth services to refill medication(s) (67.3%), prepare for an upcoming visit (66.1%), review test results (60.3%), or receive education (54.2%). Males had lower odds of preferring telehealth services for reviewing test results (odds ratio (OR) = 0.57; 95% confidence interval (CI): 0.34–0.94) or mental health issues (OR = 0.54; 95% CI: 0.38–0.77). Respondents who received a video visit were significantly more likely than those who received a telephone visit to report preferences for using telehealth for education, care plan discussions, long-term health issues, and mental health.
Discussion
Patient preferences for telehealth services vary by services provided and respondent demographics. Experience with telehealth increases the likelihood for future use of these services.
Introduction
Telehealth allows healthcare providers to leverage information technologies, video imaging, and telecommunication to deliver services at a distance. 1 Prior to the Coronavirus disease 2019 (COVID-19) pandemic, 2 the greatest growth of telehealth was anticipated to occur within the context of a medical home. 3 Response to COVID-19 resulted in an unprecedented shift and acceleration of care delivery toward remote medical services and telehealth in both medical and pre- and post-surgical service lines.4,5
Prior to COVID-19, telehealth seemed to be addressing the challenges of time, distance, and burden of medical care access. Attending a telehealth visit in the local community or from the home of a patient outweighs the inconvenience of travelling long distances for the same service, particularly for people with chronic health conditions, parents with young children, and caregivers of elderly patients. 6 Among cancer survivors, telehealth reduces treatment burden and life disruption and enhances reassurance. 7
Patient perceptions of telehealth services vary depending upon the service provided and patient population. Among dermatology patients, only 19% of participants prefer telehealth over office visits. 8 In a study of military Veterans assessing interest in telepsychiatry, only one-third of participants indicated a preference for telepsychiatry compared to office visits, with no observed preference differences by patient demographics. 9 In a survey of CVS MinuteClinics, one-third of participants preferred telehealth to office visits and women were more likely to prefer telehealth. 10 In a study of over one million patients scheduling visits in primary care, females were more likely than males, blacks were more likely than whites, and patients aged ≥ 65 years were less likely than patients aged 18–44 years to choose telehealth over an office visit. 11
Our multispecialty outpatient, non-emergent clinical practice temporarily ceased elective services in the initial stages of the COVID-19 pandemic. Telehealth services were rapidly deployed throughout the practice and available for patients to address a variety of needs, acute and chronic, either via video or phone. Patients could elect face-to-face or video consultations when COVID-19-related risk mitigation interventions were fully implemented. As the pandemic continues, clinical practices are resuming safe clinical operations, and along with this, patient preferences for telehealth services will change. 12 Within this context, opportunities exist to continue clinical services for certain populations who prefer that they be provided through telehealth. In order to determine types of healthcare services for which patients are interested in using telehealth, we conducted a survey of patients with a recently completed telehealth service within one of our internal medicine ambulatory clinical practices.
Methods
Clinical setting and technology
The Mayo Clinic is a charitable, non-profit academic medical centre with three main campuses in Minnesota, Arizona, and Florida. Our Rochester, MN, site provides both destination and community care. Our survey was deployed in the Department of Medicine (DOM), a multispecialty practice of 474 physicians serving more than 200,000 unique patients annually. Divisions in the DOM include community internal medicine (primary care), general internal medicine (consultative medicine), allergic diseases, endocrinology, gastroenterology/hepatology, haematology, infectious diseases, nephrology/hypertension, pulmonary and sleep medicine, and rheumatology. In response to the COVID-19 epidemic, consultative services were provided through telehealth in all our divisions.
Telehealth services were scheduled as regular appointments and delivered through our synchronous electronic health record (EHR)-facilitated videoconferencing system. In this system, the EPIC™ (Verona, WI) scheduling function allows providers to launch a Zoom™ (San Jose, CA) conference with the patient. The patient’s Zoom™ conference was facilitated through the Mayo Clinic ‘app’, which provides downloading Zoom™ functionality on their mobile device, but patients could also use a desktop computer. When the appointment check-in time arrived, the patient launched Zoom™ and Mayo Clinic staff members met with them to troubleshoot patient technologic capabilities and proceed with the ‘rooming procedure’ (i.e. medication reconciliation). If videoconferencing was deemed not to be technologically feasible, providers converted the visit to a telephone consultation.
If, upon scheduling, patients indicated that they could not complete a video visit, then they were scheduled as telephone calls. In these cases, the preferred phone number was listed under the appointment description and providers called the number to initiate the visit.
Survey population
In order to understand the types of healthcare services for which patients report preferences for telehealth, we generated a simple random sample of patients with a completed telehealth visit within one of our ambulatory clinical practices. Valid appointments were identified at the beginning of each week if they had been marked as ‘completed’ (as opposed to ‘cancelled’, ‘rescheduled’, or ‘no show’) over the most recent period of seven days. For the first three weeks of our surveying period, we performed a simple random sample of 50 completed appointments. We increased our sampling to 250 per week once we were comfortable with the question set and with the sampling workflow. Appointment lists were limited to one appointment per unique patient (based on medical record number), within one of our internal medicine practice areas. We collected the following demographic information from our registration files in order to decrease the number of questions for our respondents: age at time of appointment, gender, race, ethnicity, mailing address grouped into geographic region from our Rochester, Minnesota practice site.
Questionnaire
Our intent was to obtain real-time feedback on how our telehealth services were being perceived by patients during a time of rapid increase in services. We could not identify a contemporary validated questionnaire that addressed our topics of interest. Questions were constructed through relevant literature review and author consensus. We asked questions to understand patient experiences with telehealth, type of telehealth services the patient had (video visit versus telephone), and reason(s) for the visit. We also included a table of the types of services we could deliver via telehealth: recent/new health concern, refill medication(s), long-term health issues, reviewing test result(s), preparing for an upcoming visit, education about a health condition, and a telehealth visit with both their primary care doctor and specialist to discuss care plan(s). Because patients seen in our community internal medicine practice are commonly referred to psychiatry and/or psychology, we inquired about preferences regarding the use of telehealth services for mental health. We asked respondents to report their likelihood using telehealth for each service type on a five-point Likert scale (Very likely, Somewhat likely, Neither likely nor unlikely, Somewhat unlikely, and Very unlikely).
All surveys were deployed at the beginning of the week (Monday or Tuesday) for the most recent seven days of completed visits. Surveys were launched via Qualtrics survey software (Provo, UT, USA). Patients received an email invitation to participate in our survey, then one follow-up reminder three days after the initial invitation. We launched our initial surveys on Tuesday, April 28, 2020. A new cohort was invited weekly until closing the survey on Monday, July 20, 2020. We invited a total of 13 rounds of patients (n = 2650). Our survey was launched as a quality improvement initiative and did not require review according to the guidance of the Mayo Clinic Institutional Review Board. A copy of our survey instrument is provided as a supplemental file.
Statistical analyses
Summary statistics were created to describe our survey respondents, including frequency (n) and proportion (%). Continuous age was collapsed into 15-year age intervals. To understand the factors associated with the odds of preferring telehealth based on service need, we created a single flag to represent ‘Very likely’ and ‘Somewhat likely’ for each type of healthcare service. Unadjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated for each patient and appointment factor. All data management and statistical analyses were performed using Statistical Analysis Software (SAS) Version 9.3 (Cary, NC, USA).
Results
Survey respondents
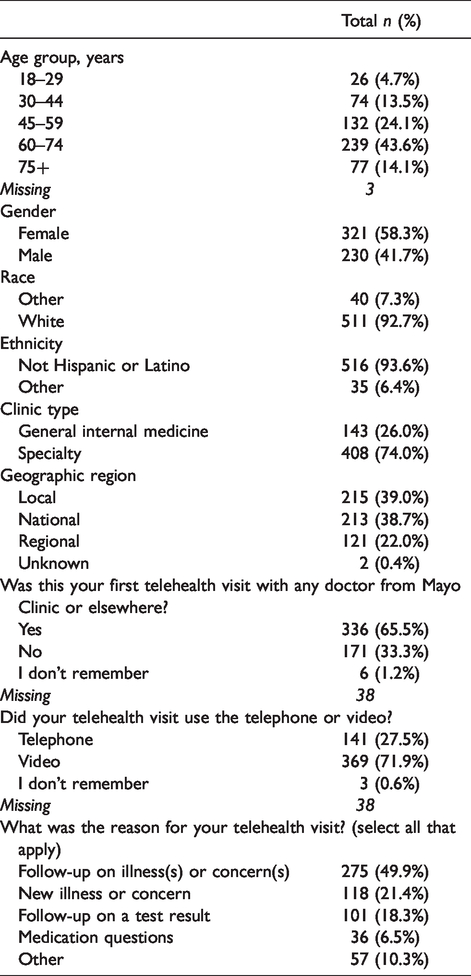
We had a total of 551 responses to our telehealth survey (response rate = 20.8%, 551/2650). The average age of our survey respondents was 59 years, with a median of 62 years. The majority of our respondents were female, white race, and of non-Hispanic or Latino ethnicity (Table 1). Three quarters of our respondents had their telehealth visit in one of our specialty practices as opposed to our general internal medicine groups. A majority of respondents reported that this was their first telehealth experience (65.5%) and had their telehealth visit via video (71.9%). Respondents had their telehealth visits predominantly to follow-up on an illness or concern (49.9%), evaluate a new illness or concern (21.4%), or as a follow-up for a test result (18.3%).
Survey respondents (n = 551).
Likelihood of using telehealth services based on service need
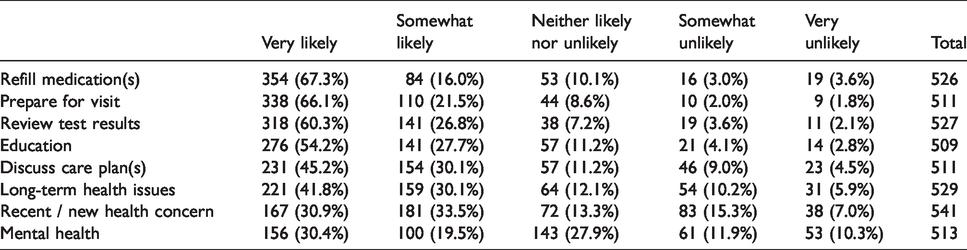
A majority of respondents indicated being ‘very likely’ to use telehealth services to refill medication(s) (67.3%), prepare for an upcoming visit (66.1%), review test results (60.3%), or for education (54.2%) (Table 2). Less than one-third of patients were ‘very likely’ to use telehealth services for a recent or new health concern or for mental health issues.
Likelihood of using telehealth services by service type.
Factors associated with higher odds of using telehealth based on service need
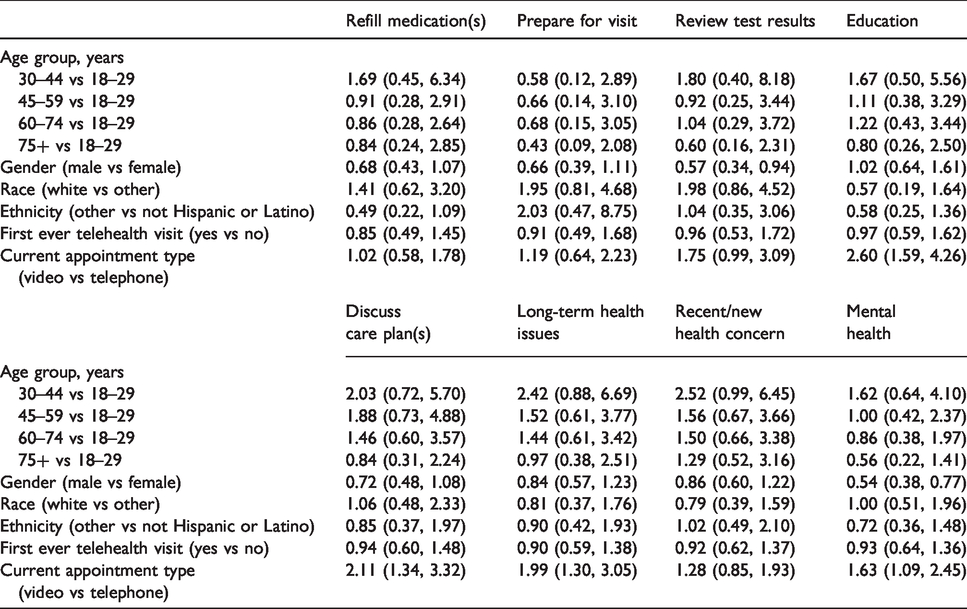
Compared with female respondents, male respondents had lower odds of preferring telehealth services for reviewing test results (OR = 0.57; 95% CI: 0.34–0.94) or for mental health concerns (OR = 0.54; 95% CI: 0.38–0.77) (Table 3). Respondents whose current visit was conducted via video, as opposed to telephone, had higher odds of preferring telehealth services for education (OR = 2.60; 95% CI: 1.59–4.26), discuss care plans (OR = 2.11; 95% CI: 1.34–3.32), long-term health issues (OR = 1.99; 95% CI: 1.30–3.05), and mental health issues (OR = 1.63; 95% CI: 1.09–2.45).
Odds of reporting increased likelihood (‘Very likely’, ‘Somewhat likely’) of using telehealth services by demographic (odds ratio (95% confidence interval)).
Discussion
We observed that the majority of patients reported being very likely to use telehealth services for medication refills, preparing for a clinical visit, reviewing test results, and receiving education; less than one-third of patients were very likely to use telehealth for a recent or new health concern or a mental health issue. Compared to women, men had lower odds of preferring telehealth services to review test results and for mental health issues. Use of video telehealth services was associated with higher odds of wanting to use telehealth for education, discuss care plans, long-term health issues, and mental health issues compared to use of telephone for the visit.
We observed the lowest percentage of preference overall was for ‘telemental health’ services. Our finding is similar to that from US Veterans, among whom less than one-quarter were ‘extremely comfortable’ using telemental health from home or at a local clinic and only one-third would prefer telemental health over face-to-face visits. 9 This may be related to a desire on the part of patients to establish rapport with a provider 13 or concerns about confidentiality. 14 This result may also be due to our survey cohort seeking medical specialty services initially. Importantly, telemental health services have demonstrated effectiveness for improving symptoms, 15 and no differences have been observed in the therapeutic efficacy of telemental health compared to face-to-face interventions. 16
We observed that the odds of patient preference for telehealth was higher if their appointment leveraged video rather than telephone. Previous research has also observed that prior experience with a video visit, compared to a telephone visit, within the past year was associated with selecting a telehealth visit over an office visit. 11 Future acceptance of telehealth services for populations less likely to prefer it may be higher as many individuals are being ‘required’ to experience it in the current pandemic.
Men had lower odds than women to have a preference for reviewing test results and for addressing mental health issues using telehealth. Previous surveys have observed that women are more likely to prefer telehealth 10 and are more likely to choose a telemedicine visit (either phone or video) than male patients. 11 Understanding gender preferences emphasizes the potential importance of maintaining specific service offerings for women challenged with childcare, spousal care, and elder caregiving, 17 but also suggests that opportunities exist to increase the appeal of these services to men.
We observed that the second lowest preference for telemedicine services overall was for recent or new health concerns. Patient concerns about inaccurate diagnoses may exist. 18 However, previous studies have observed that for low-acuity illnesses, the diagnostic accuracy between telehealth and clinical encounters is comparable. 19 Furthermore, video telehealth visits provide improved diagnostic accuracy over telephonic assessments. 20 We also observed that almost three-quarters of patients would be ‘somewhat’ or ‘very likely’ to use telehealth for long-term health issues. Previous studies have identified that patients are more likely to select telehealth visits if it occurs with their primary care provider. 11 As primary care evolves, our data suggest that opportunities exists to expand telehealth options for chronic disease management, which has been demonstrated to reduce costs and improve health outcomes. 21
Our survey is limited by the fact that we conducted a cross-sectional assessment during a pandemic, which may not represent usual patient preferences. Our population was predominantly white and non-Hispanic, which likely explains why we did not observe differences in telehealth choices by race as has been observed previously. 11 Additionally, our respondents are not representative of patients who have limited English proficiency (LEP) and an active patient online account was required to schedule a telehealth visit; only 20% of LEP patients have an active online account compared to 65% of non-LEP patients. We also had a low survey response rate, and because this was a quality improvement survey, we were not adequately powered to detect differences in some comparisons.
Strengths of our survey include the minimization of response bias due to timely assessment within seven days of appointment and a random sampling approach to minimize sampling bias. The survey is also unique in that the average age of survey respondents was 59 years, with a median age of 62 years, which is older than the typical age of telehealth users.
As organizations return to normal clinical operations, ours and existing data should encourage practices to reflect on opportunities to continue to provide patients the option for telehealth services beyond the current pandemic. Continuing clinical services to specific subpopulations who prefer telehealth services and discovering new opportunities to appeal to subpopulations less inclined to use it will provide flexibility, access, and uninterrupted clinical care to patients in current and future pandemics.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JOE has a consulting arrangement with Nesmah™ outside the topic of the current submission. No other authors have conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This survey was supported by Community Internal Medicine, Department of Medicine, Mayo Clinic.
Supplemental material
Supplemental material for this article is available online.