
Abstract
Introduction
This study evaluated the impact of a telephone support programme with telemonitoring on changes in healthy eating and active exercise in adults with prediabetes using the stage of change framework.
Methods
We performed a post hoc analysis using data from the Japan Diabetes Outcome Trial-1. A total of 2607 participants aged 20–65 years with impaired fasting glucose were recruited from the workplace/community in Japan and randomized to a one year telephone support programme intervention arm (n = 1240) or self-directed control arm (n = 1367). Participants in both arms received monthly data feedback from a weight scale and pedometer. The main outcome measure was the stages of change toward healthy eating and active exercise. The secondary outcome was fasting plasma glucose (FPG).
Results
After the one year intervention, the adjusted odds ratio of progressing to the action/maintenance stage in the intervention vs. control arm for healthy eating was 1.31 (95% confidence interval (CI) 1.21–1.43; p < 0.001), but that for active exercise was 1.07 (95% CI 0.99–1.15; p = 0.062). The intervention decreased FPG levels in participants in the contemplation stage, but not in the precontemplation, preparation and action/maintenance stages.
Discussion
These findings suggest that the telephone support programme by healthcare providers advanced the stage of changes toward healthy eating in people with prediabetes. In particular, it decreased FPG levels in the contemplation stage.
Keywords
Introduction
In Japan, specific health checkup services are provided for all insured persons and dependents aged 40–74 years. These health checkups are intended to identify persons requiring health guidance, in order to decrease the prevalence of type 2 diabetes (T2D), metabolic syndrome and cardiovascular disease.1,2 A weight gain of 10 kg or more since the age of 20 is associated with increased medical expenditure. 3 Non-specific health checkup services are provided optionally for dependents aged 20 to 39 in some large companies and communities to reduce metabolic syndrome at the age of 40 and medical expenditure. 4 The results of specific health checkups are ranked by level, and the appropriate health guidance (group, individual, telephone and email support) is provided. 5 Participants receiving health guidance were found to show greater improvements in metabolic profiles with proportionally smaller pharmacological treatment initiations compared with nonparticipants over the course of 3 years. 6 In the current coronavirus disease (COVID-19) pandemic, telephone support programmes are generally preferred over face-to-face group or individual support programmes.
On the other hand, specific health checkup services use standardized self-administered questionnaires. These questionnaires are also used to assess changes in healthy eating and active exercise. Stages of change lie at the heart of the transtheoretical model (TTM), as studies on change have found that individuals move through a series of stages when modifying behaviour. The stage of the change framework suggests that intervention programmes could possibly be tailored to the individual’s stage of readiness. 7
Telephone support is a lifestyle intervention that offers moderate benefits for glycaemic control and blood pressure in patients with T2D. 8 The Japan Diabetes Outcome Intervention Trial-1 is a nationwide telephone support programme that uses telemonitoring to prevent T2D in the workplace/community. 9 However, little is known about the efficacy of the telephone support programme in promoting healthy eating and active exercise. This study evaluated the impact of the programme on changes in healthy eating and active exercise in adults with prediabetes using the stage of change framework.
Methods
Study design
This prospective, pragmatic, cluster-randomized, controlled trial included 43 health examination centres (clusters) across Japan. A post hoc analysis of a cluster-randomized controlled trial was performed. This study was conducted according to the principles of the Declaration of Helsinki.
Participants
Using the health checkup data, candidates who met the inclusion criteria were identified in each group. The inclusion criteria were age 20–65 years and impaired fasting glucose, defined as a fasting plasma glucose (FPG) level of 100–125 mg/dL (5.6–6.9 mmol/L). The exclusion criteria were diagnosis of diabetes, history of using antidiabetic agents and glycated haemoglobin level ≥6.5%. Forty-three health examination centres were randomly assigned to an intervention (n = 1,240) or to a self-directed control arm (n = 1,367) by independent statisticians, according to a computer-generated list.
Telephone support programme with telemonitoring
Healthcare providers such as public health nurses and registered dieticians assessed lifestyle, stage of change, health status and knowledge of diabetes. The assessments were performed using a self-administered questionnaire. 9 Their support as coaches included assisting the participants in making realistic and measurable goals to increase self-efficacy, discussing the advantages and disadvantages of health behaviour changes with the participants, and identifying barriers to health behaviour change and discussing problem-solving approaches for improving the ability to address barriers with the participants. The participants of both arms received a weight scale (HBF-354 IT-2, Omron Healthcare Co., Ltd) and a pedometer (HJ-710 IT, Omron Healthcare Co., Ltd.) with a storage function. They could send accumulated data to the lifestyle support centre free of charge using a transmitter (DC-100; JMS Co., Ltd., Japan; Figure 1). Participants in the intervention arm received 1 year of goal-focused lifestyle support from healthcare providers by telephone, but the control arm did not. The research team determined the number of calls, and healthcare providers in the lifestyle support centre initiated the call participants. The intervention arm received five to six phone calls (mean 5.6 ± 3.2 calls) per year, with the length of each call being between 15 and 30 minutes. The first session was an ‘introduction and welcome call,’ and subsequent sessions were ‘support calls.’ During the support call, the goal achievement and design of a correction plan were evaluated. The participants in the control arm received a pedometer and periodically received newsletters, which contained health-related information.
Data collection
Data on age, height, body weight, body mass index, FPG level, triglyceride (TG) level, high-density lipoprotein cholesterol (HDL-C) level, systolic blood pressure (SBP) and diastolic blood pressure (DBP) were collected at baseline and after the one year intervention. Healthy eating was defined as restrained eating, consumption of low fat and nutritionally balanced meals and slow eating. Healthy exercise habits were defined as regular moderate-intensity exercise for at least 30 minutes, two or more times a week. 10 Active exercise includes activities such as aerobic dance, brisk walking, jogging, swimming, cycling and sports. However, it does not include physical activity at work. A five-item response format was used for assessing healthy eating and exercise habits based on the TTM of the stages of change.11,12 The five stages of change are precontemplation (no intent to take action), contemplation (intention to take action within the next 1 month), preparation (intention to take action within the next 1 month, with some behavioural steps in this direction already taken), action (overt change in behaviour for ≤6 months) and maintenance (overt change in behaviour for >6 months). Participants completed questionnaires on importance and confidence (self-efficacy) for healthy eating and active exercise using five-point Likert scales. 11
Data analysis
Data on the participants in the action and maintenance stages were combined in the analysis. Categorical variables were compared with χ2 or Fisher’s exact test, and continuous variables were compared with the t-test or nonparametric Wilcoxon rank-sum test. Logistic regression was used to calculate odds ratios (ORs) and 95% confidence intervals (CIs) by adjusting for potential confounders, including age and sex. The trend test was performed using the Cochran–Armitage or Jonckheere–Terpstra trend test. The data were analyzed using Stata/IC version 13.1 software (StataCorp, College Station, TX, USA) and Statistical Package for the Social Sciences software, version 24.0 (IBM Corp., Armonk, NY, USA). Patients with missing data were omitted from the relevant analysis. Statistical significance was set at p < 0.05.
Results
Demographics
At baseline, 5.9% of participants were in the precontemplation stage, 50.6% were in the contemplation stage and 25.5% were in the preparation stage in the change towards healthy eating. At baseline, 9.4% were in the precontemplation stage, 50.2% were in the contemplation stage and 12.0% were in the preparation stage in the change towards active engagement in exercise activity (Table 1). There was no significant difference in the proportion of stage of changes between the arms. There were no significant differences in FPG levels for trend of stage, although the proportion of men in the intervention and control arms tended to decrease according to advanced stages (P for trend: 0.017 and 0.002, respectively). The baseline changes in healthy eating were significantly associated with eating breakfast, nutritional balance, restrained eating, avoiding sugar-sweetened beverages and vegetable consumption (Table 2). We found significant effects of the stage of change on importance and confidence (self-efficacy).
Baseline characteristics of the participants according to the baseline stage of changes for healthy eating (n = 2574).

Values are presented as percent (%) or mean (standard deviation).FPG; fasting plasma glucose; BMI: body mass index.
Baseline characteristics of the participants according to the baseline stage of changes (n = 2574).

* p < 0.05 (vs. baseline). p-value (intervention arm vs. control arm after one year intervention).
SVs: servings.
Stage of change and cardiovascular risk factors
The ORs of progressing to the action/maintenance stage for the intervention and control arms for healthy eating and active exercise after 1 year of intervention and at the end of the trial were 1.31 (95% CI 1.21–1.43) and 1.07 (95% CI 0.99–1.15), respectively (Table 3). All participants in the intervention arm, regardless of their stage at baseline, advanced in stage of change towards healthy eating; however, this was not the case for the participants in the control arm. Among participants in the intervention arm, decreased body weight was observed in participants in the contemplation and preparation stage and decreased FPG level and DBP in participants in the contemplation stage (Table 4). There was no difference in incident diabetes after one year intervention between groups (Supplementary table 1). The proportions of participants who ate nutritionally balanced meals, practised restrained eating, avoided sugar-sweetened beverages and consumed more vegetables in the intervention arm after the one year intervention were higher than those in the control arm, but the proportion of participants who ate breakfast was lower (Table 2). We adjusted for baseline age and sex in the analysis. There were no significant predictive values at baseline for changes from precontemplation to contemplation using logistic regression analysis (Supplementary table 2). The proportion of eating breakfast, nutritional balance, restrained eating and vegetable consumption, except for no sugar-sweetened beverage intake, significantly increased according to advanced stages in participants with contemplation stage at baseline (Supplementary table 3).
Adjusted odds ratio of being in the action/maintenance stage after the one year intervention in the intervention and control arms by baseline stage (n = 2574).
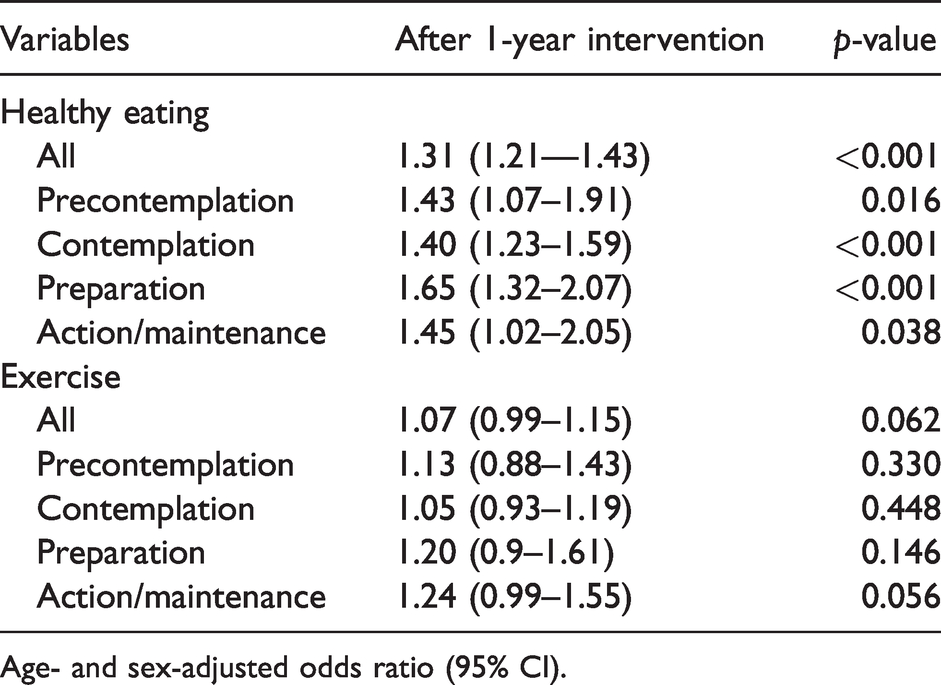
Age- and sex-adjusted odds ratio (95% CI).
Characteristics of the participants at baseline and after one year intervention according to the baseline stage of changes (n = 2574).
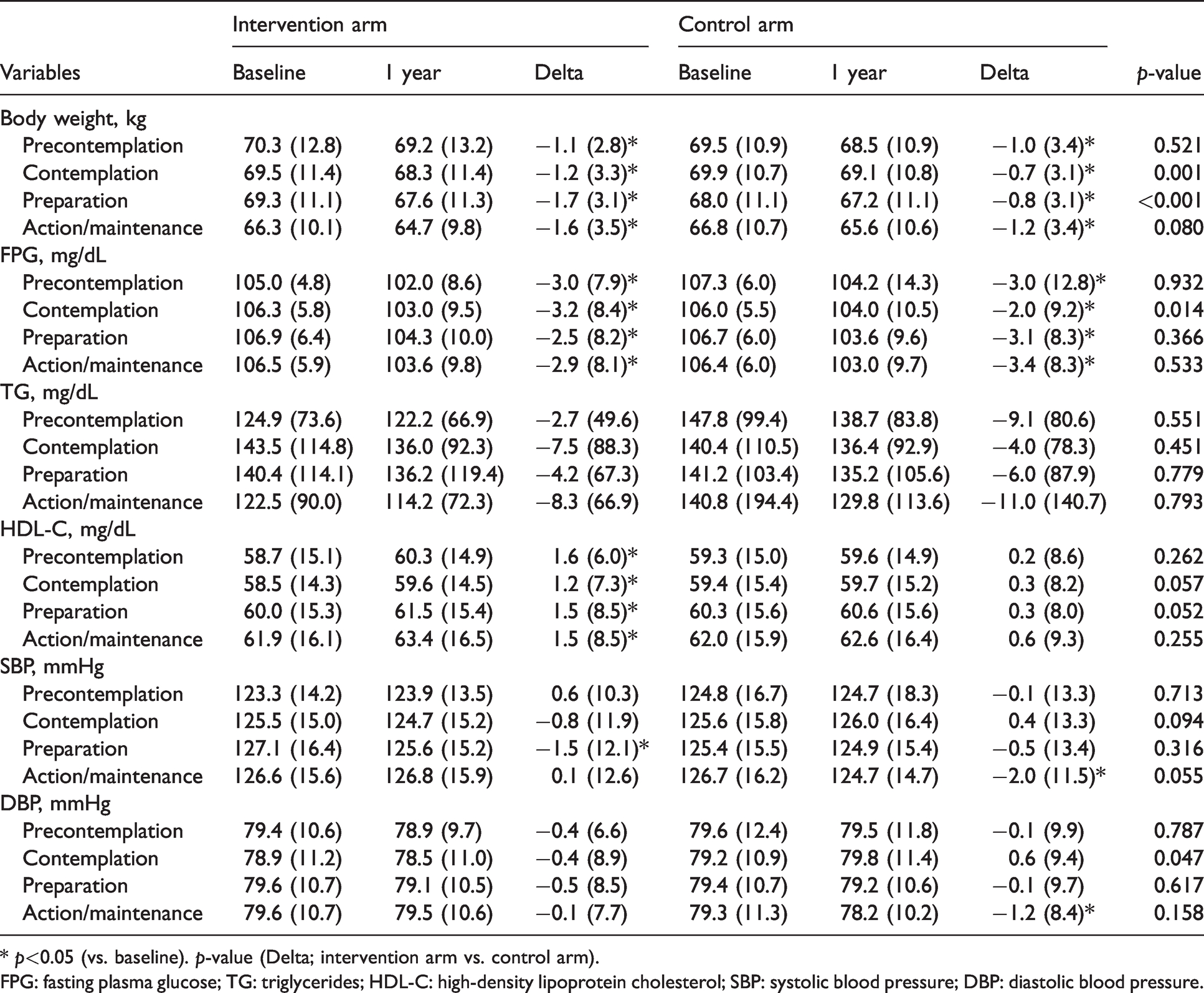
* p<0.05 (vs. baseline). p-value (Delta; intervention arm vs. control arm).
FPG: fasting plasma glucose; TG: triglycerides; HDL-C: high-density lipoprotein cholesterol; SBP: systolic blood pressure; DBP: diastolic blood pressure.
Discussion
This study showed that a telephone support programme with telemonitoring and healthcare provider coaching progressed the stage of change for healthy eating but not for active exercise among individuals with prediabetes. There are two possible reasons why the intervention did not progress the stage of change for active exercise: (1) the participants in the control arm received a pedometer and periodically received newsletters, which contained health-related information, and (2) the dietician or public health nurse was presumably not good at exercise education. Thus, the impact of the intervention on exercise engagement was likely to be small.
The intervention decreased FPG level and DBP only in participants in the contemplation stage. The stages of change theory explains behaviour change as a series of levels of readiness to change.12,13 Contemplation is the stage in which individuals intend to change in the next 6 months. They are more aware of the pros of changing but are also acutely aware of the cons. 14 The intervention was most effective in participants in the contemplation stage.
Several healthy eating behaviours were improved by the intervention. Clinical and epidemiological studies have indicated that sugar-sweetened beverage intake is associated with obesity and T2D.15,16 One previous study reported that restrained eating was associated with weight gain in middle-aged adults. 17 Two servings per day of vegetables was associated with an increased risk of T2D. 18 Healthy eating may reduce the incidence of T2D. Although healthy eating is important in preventing T2D, dietary adaptations are often challenging. Further studies, including those on mindfulness eating, 19 are needed to confirm these findings.
Strengths and limitations
The strengths of this study include its large sample size and long follow-up duration. However, this study has several limitations. The data are presented in terms of self-reported stages of change, which may lead to bias and error. The study was conducted in health examination centres in Japan, and the results may not be applicable to other settings. The meta-analysis showed that a reduction in fat consumption and an increase in the consumption of fruits and vegetables are progressions in the stages of change and weight loss identified by the TTM. 20 In this study, restrained eating was treated as a healthy eating habit. In previous studies, fat consumption and salt restriction were also considered. HbA1c levels were not routinely measured in specific health checkups. At present, we are developing a smartphone-based application combined with a weight scale and pedometer for diabetes prevention. To improve the programme, real-time monitoring and immediate feedback via chatbots are required.

Telephone support using telemonitoring.
Conclusion
Telephone support programmes with telemonitoring coached by dieticians and public health nurses advanced the stage of changes towards healthy eating but not towards active exercise in prediabetic individuals in this study. In the current COVID-19 pandemic, weight gain, inadequate sleep, unhealthy eating habits such as snacking after dinner, lack of dietary restraint and eating in response to stress are common because of self-quarantine. 21 Non-face-to-face telephone support can be easily and safely used for lifestyle intervention in place of face-to-face intervention. With the mobile phone, many functions such as pedometers and software applications for self-weighing can be used to help individuals achieve healthier living. Evidence of telemedicine technologies in diabetes prevention is scarce compared to diabetes care and the screening for diabetic retinopathy.22,23 The results of this study provide new useful information on the psychological aspects of diabetes prevention using telemedicine technologies.
Supplemental Material
sj-pdf-1-jtt-10.1177_1357633X211010981 - Supplemental material for Impact of telephone support programme using telemonitoring on stage of change towards healthy eating and active exercise in people with prediabetes
Supplemental material, sj-pdf-1-jtt-10.1177_1357633X211010981 for Impact of telephone support programme using telemonitoring on stage of change towards healthy eating and active exercise in people with prediabetes by Naoki Sakane, Yoshitake Oshima, Kazuhiko Kotani, Akiko Suganuma, Kaoru Takahashi, Juichi Sato, Sadao Suzuki, Kazuo Izumi, Masayuki Kato, Mitsuhiko Noda and Hideshi Kuzuya in Journal of Telemedicine and Telecare
Footnotes
Acknowledgements
NS, KI, MK, MN and HK conceived the idea. JS and SS curated the data. YO, AS, KT, JS and SS analyzed the data. NS and HK acquired the funding. KK, SS, KI, MK and MN collected the data. NS wrote the original draft. YO and HK reviewed and wrote the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Health and Labour Sciences Research Grant (Strategic Outcomes Research Programme for Research on Diabetes and Comprehensive Research on Diabetes/Cardiovascular and Lifestyle Related Diseases) from the Ministry of Health, Labour and Welfare of Japan. This work was also partly supported by JSPS KAKENHI (Grant Number 18K01988).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.