
Abstract
Introduction
Despite significant investment by governments to boost the uptake of clinical trials, disparity in access to trials continues between metropolitan and regional & rural sectors. 1 This is mainly driven by limited availability of trials closer to home, need for travel and cost and consequences of travel. 2 Even within metropolitan sectors, access to clinical trials for patients with rare cancers is not consistent for all patients due to limits on the number of trial sites which can be opened. For sponsors, setting up clinical trial sites at multiple centres is not cost effective especially when the rate of recruitment can be very low at these sites. Smaller centres that are unlikely to achieve recruitment targets will continue to miss out on opportunities to host trials locally and as a result, their workforce may not enjoy the many benefits of participating in clinical trials including the ability to provide cutting edge medical therapies and partnerships with clinical trial industry. 3
Therefore, a new clinical trial model was required to improve access locally and the solution needed to be underpinned by creating interconnected clusters/networks linked by e-health and telehealth solutions. Telehealth models have been established as feasible, safe, acceptable and cost-effective systems to deliver care remotely and can be extended to the conduct of clinical trials under the concept of the ‘Teletrial model’.4–6 In this model, smaller sites (satellite sites) are connected to larger centres (primary sites) by telehealth so that some or all aspects of clinical trials can be offered to satellite site patients closer to home. Oversight of the trial cluster activities by the primary investigator at the primary site is addressed through supervision plans and regular trial meetings. In Australia, under the auspices of the Clinical Oncology Society of Australia (COSA), a framework for a Teletrial model namely the ‘Australasian Teletrial Model (ATM): National guide for implementation’ was developed and implemented in three states. 4
The national guide outlines several requirements that need to be satisfied to ensure the ethical and safe conduct of clinical trials using ATM. These requirements include: Selection of satellite sites and suitable trials, supervision plans and site visits, Workforce, Good clinical practice, Roles and responsibilities, Training, site initiation meetings and trial updates, Technology and support, Participant screening and recruitment, Obtaining participant consent, Medication handling, Managing and reporting serious adverse events, Patient reported outcomes, Documentation and reporting, Financial, Regulatory and indemnity considerations, and clinical trial agreements.
To guide the project, two implementation science frameworks were chosen, since many of the existing frameworks were not sufficient as a single guide: iPARIHS 7 and Strategic implementation framework (SIF). 8 iPARIHS defines successful implementation as a function of innovation, recipients, context and facilitation. SIF divides the implementation into three stages: setting the stage, active implementation and monitor, sustain and support. It was apparent during the previous implementation of the tele-chemotherapy model that clinicians also needed to identify and apply several clinician levers to overcome barriers. 9 , 10
This paper aims to describe the processes and steps undertaken in the development and implementation of the ATM.
Methods
Project processes and steps are discussed under components of iPARIHS 7 and SIF. 8
Results
The starting point was to establish stakeholder agreement about the need for a new model and framework. ‘Driving action through purpose’ was a useful framework for articulating the difficulties faced by rural patients. 11 Since systematized Teletrial model has not been described before, many stakeholders showed reluctance to accept this model as a safe and feasible model.
Innovation: Translating idea into a framework
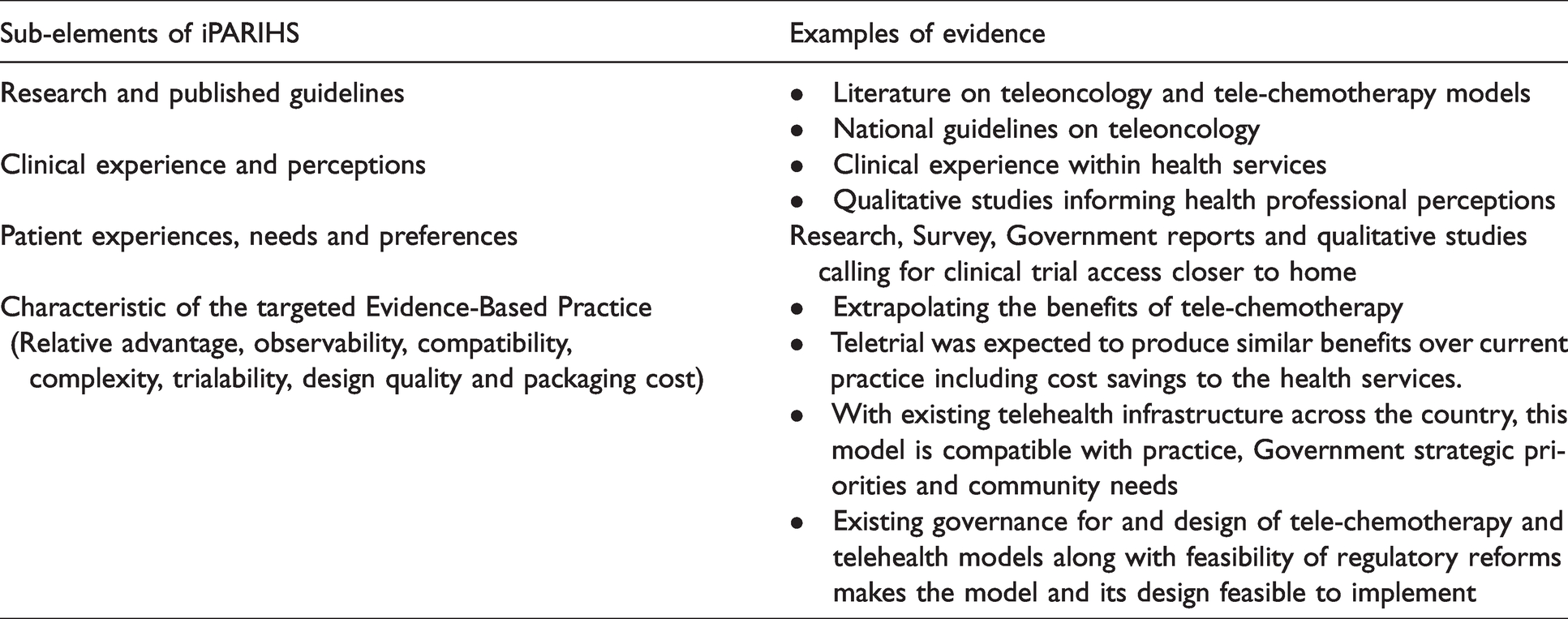
iPARIHS Evidence and Evidence based practice characteristics offered a useful framework to address concerns and to convince the major stakeholders of the validity of this model. These characteristics include: Research and published guidelines, Clinical experience and perceptions, Patient experiences, needs and preferences, Relative advantage, observability, compatibility, complexity, trialability, design quality and packaging cost. In the absence of published research on Teletrial models, several examples that satisfied iPARIHS criteria were used to make the case, as listed in Table 1.
iPARIHS evidence and evidence-based practice characteristics supporting the concept of Teletrial.
Once the concept was accepted by members of the COSA Council based on its merit, the key steps included the development of the national guide and its implementation.
Recipients
Given the complexities associated with clinical trial operations, a co-design approach was taken with the following stakeholders: 12 Consumers (Cancer Voices and Rare Cancer Australia), clinical champions (COSA Council), the trials industry (Cooperative Trial Groups (CCTGs), investigators and the pharmaceutical industry), clinicians (clinician networks and COSA members), regulatory bodies (government Departments of Health, Research Governance Offices, lawyers and Human Research Ethics Committees), funders (Medicines Australia, Cancer Australia, universities, MTP Connect) and power brokers (Governments, Health Service Chief Executives, managers).
Context
The clinical trial environment is regulated and influenced by global, national and statewide policies and, therefore, change needs to occur at multiple levels. Many pharmaceutical companies and trial networks are global entities. In any given country, change needs to occur at least at national and state levels, thus requiring the support of national and statewide stakeholders. Timing for this initiative was opportune since there were calls for cultural and structural reforms at Government, industry and clinical levels to create a patient, sponsor and clinician friendly clinical trial system across Australia. 1
Facilitation
The context of implementation was at state, health service and cancer centre level. Recipients were predominantly the same organizations (who participated in the development of the ATM and national guide) that needed to adopt the ATM as routine business. Each stakeholder group was necessary for their contribution: State Governments for developing policy frameworks, regulatory reforms and standard operating procedures (SOPs); pharmaceutical industry and cooperative clinical trial groups (CCTGs) for incorporating the ATM as a recruitment mechanism within their protocols; and cancer services and clinicians for accepting satellite sites as part of their trial clusters. Additionally, clinical champions were required at local levels to drive the project. This project was facilitated at a national level.
A steering committee consisting of appropriate stakeholders, power brokers and champions (Australian Teletrial Consortium) was established to oversee the operations of the project. Three advisory groups were established to provide expertise – Industry, CCTG and state department of health.
Implementation
In terms of implementation itself, the Strategic Implementation Framework by Mitchell and Chambers (2017) provided a practical checklist to ensure the necessary components were put in place. 8 SIF sets out three stages of implementation namely Setting the stage, Active Implementation and Monitor, Support and Sustain.
Setting the stage
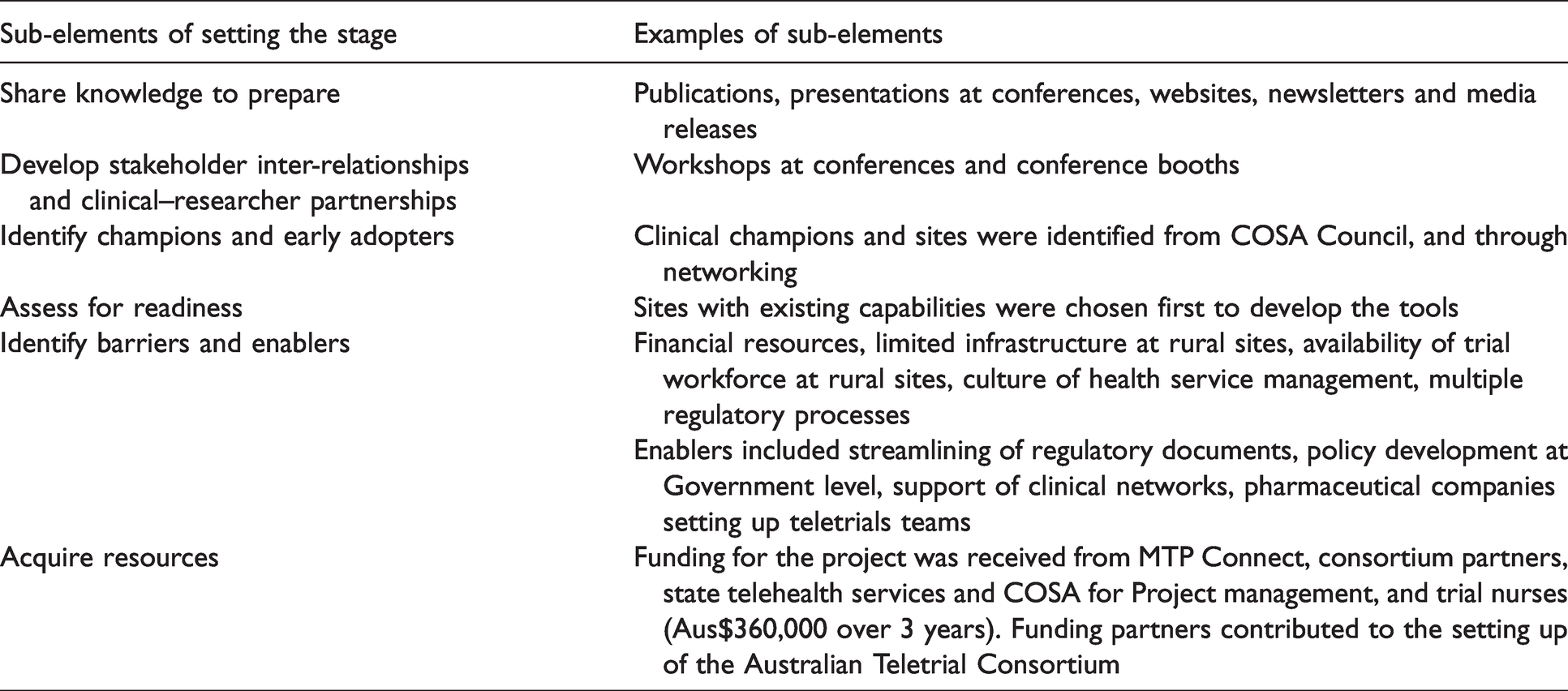
Setting the stage is a complex stage where the foundation for implementation is laid. A key step in our project was the development of the national guide, in partnership with key stakeholders who needed to change their internal processes to adopt the model. At this stage of implementation, the context is national, statewide, health service wide and departmental level. National and statewide adoption usually requires policy mandates and funding. At clinical levels, this requires leadership and leadership support within health services and departments. Other sub-elements of this stage included sharing of knowledge, development of stakeholder relationships, identification of early adopters and champions, assessing for readiness, identification of barriers and enablers, and acquiring of resources. Table 2 summarizes the examples of sub-elements we put in place to prepare for this stage of our project.
Setting the stage of Strategic implementation framework and Australian Teletrial Model implementation process.
Active implementation
Monitor, support and sustain
Implementation was monitored through regular meetings with sites and steering committee meetings. Ongoing education and guidance to sites were provided using workshops and webinars. New sites were given hands-on support and mentoring to set up Teletrial clusters. Project progress was promoted through presentations at the annual scientific meetings of stakeholder organizations.
Clinical trial uptake using ATM
At the time of writing, satellite sites were added to nine existing trials. Of the 10 satellite sites (distance from primary sites ranging from 150 to 1000 km), four sites had never conducted clinical trials before. Twelve new health professionals acquired Good Clinical Practices training. Details of the studies are summarized in Table 3.
Details of clinical trials that incorporated Australasian Teletrial Model as recruitment method.
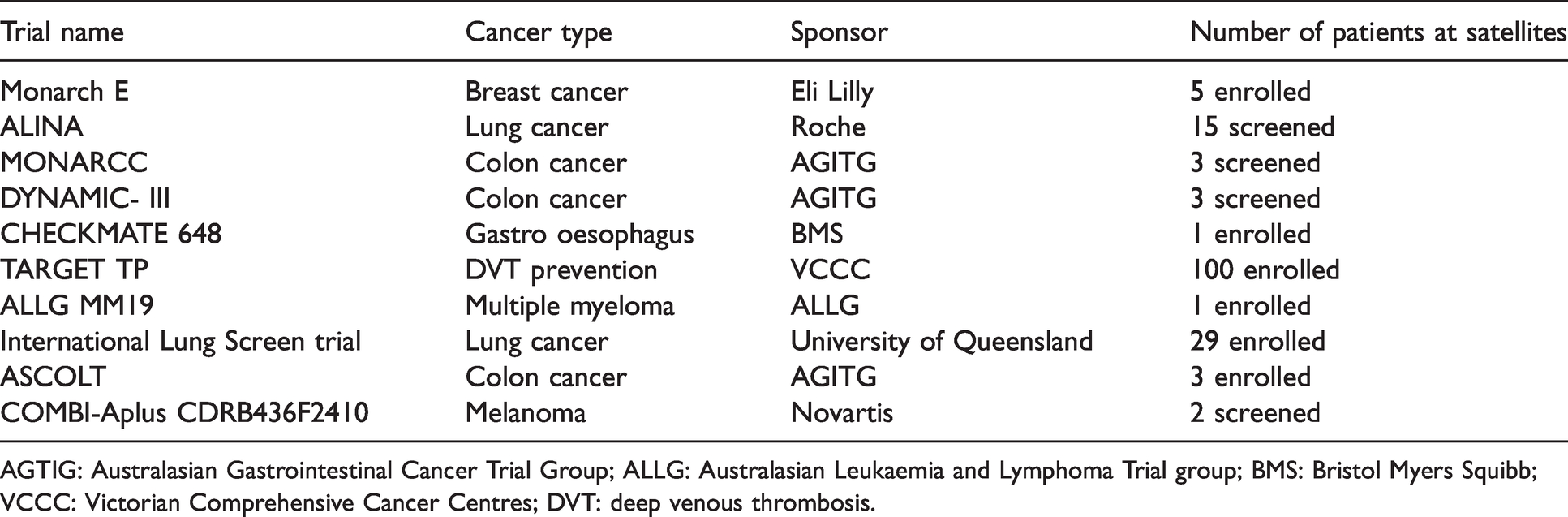
AGTIG: Australasian Gastrointestinal Cancer Trial Group; ALLG: Australasian Leukaemia and Lymphoma Trial group; BMS: Bristol Myers Squibb; VCCC: Victorian Comprehensive Cancer Centres; DVT: deep venous thrombosis.
Development of supervision plans
The supervision plan allowed some primary sites to delegate all responsibilities to selected satellites based on their capabilities. Some primary sites cared for patients at satellites solely via telehealth in partnership with satellite site physicians or medical oncologists.13–15 At sites that had never conducted clinical trials before, primary sites were able to delegate some trial activities to the satellite site staff after they gained confidence and expertise with the trial model over several months.
Timelines for site activation
It took nearly 6 months to activate the first satellite due to the need to develop new processes and to support system adaptation; subsequent satellite sites were activated within 3 months. In a recent trial, when a patient was identified at a site, that site was activated as a satellite within 2 weeks.
Feedback from health professionals
Primary site Clinical Trial Coordinators reported an additional workload setting up satellite sites, coordinating regulatory documents, organizing cluster meetings and managing documentation. Some satellite sites required hands-on support for running the trials and managing trial-related paperwork. Despite this, many health professionals welcomed the new collaboration with other sites.
Overcoming barriers (using clinician levers)
Clinician levers are mechanisms or tools that arise from clinicians’ role as patient advocates and can be used to overcome roadblocks or barriers to broader implementation of patient-centred programmes especially initiated and driven by clinicians. 9 , 12 Several clinician levers were used to overcome roadblocks: partnerships with consumer agencies, connections with media, reference to Government and other organizational strategic plans to address equity and disparity, and escalation to senior leaders and politicians and peak organizations.
Lessons learned
Coordination between sites for multiple trials, monitoring of capabilities of sites and education and upskilling of new staff is likely to be more efficient if a central resource is established within each state. For many larger centres, this model created additional workload and for many smaller centres, ATM was a new activity. Therefore, to scale this model, additional human resources are needed at both primary and satellite sites for clinical trial coordination and cluster coordination. Apart from the champions who provided in-kind contribution, many clinicians and management professionals felt that there was nothing in it for them. To overcome this mindset, incentives are required to drive large-scale adoption. Regulatory processes need to be reformed to facilitate rapid approvals when patients are identified at satellites Large scale adoption and incorporation into business as usual requires government ownership at policy level.
Discussion
This paper illustrates the steps taken to translate the idea of a Teletrial model into a national model through a two-step process: development of a national guide and its implementation. The idea of teletrials had merit because of its potential benefits for patients and the clinical trial industry and by meeting the criteria outlined in the iPARIHS framework it qualified as a worthwhile innovation. 4 In terms of context, the project needed the involvement of stakeholders from multiple levels and jurisdictions: from national level to clinical level. This allowed stakeholders to be chosen to represent all the different layers and perspectives. The facilitation aspect was an important one since it required influence at government and industry levels as well as clinical levels. Without holding positional levers, COSA needed the involvement and support of governments and industry at least at advisory capacity. Operating under the auspices of COSA was necessary for success since it is the peak clinical body in Australia for cancer care professionals and has cemented its status as an advocacy agency for reforms in cancer care.
One of the main reasons for the project success was that the national guide was co-designed by the same stakeholders who were going to implement it. Since multiple perspectives were already covered by the relevant experts, some of the important ethical and legal considerations have already been addressed. Ideally, uniform processes across all three jurisdictions would have made this project even more efficient. However, it was unrealistic to expect COSA and the project partners who do not hold authoritative roles within government to harmonize the long-standing clinical trial processes and regulations of multiple state governments.
The project successfully demonstrated the strategic vision that an interconnected clinical trial system could be created through the Teletrial model and as a result, more regional and rural sites could acquire clinical trial capabilities; more patients access clinical trials closer to home without disrupting continuity of care and that the rate of recruitment could be expedited. This is particularly important for rare cancer trials, since a networked approach facilitates access to more patients. As described in previous research, it was also observed that many rural sites that are unable to acquire capabilities as standalone sites because of low patient volume can participate in clinical trials through this model. 3
While this pilot project was a success and adopted by stakeholders, we regard this as a work of champions. Future scaling up and sustainability would require Government ownership to ensure the policy, funding, legal and regulatory levers are used to implement within health services and the resources are available to sustain these programmes. Ongoing regulatory reforms and digital trial management systems informed by end users will help minimize regulatory and administrative burden on clinicians and trialists. In the Australian setting, a national system can be designed by incorporating feedback provided by stakeholders who participated in this pilot project. Fortunately, based on this pilot’s implementation results, the Australian Government has recently adopted the Teletrial model 16 and allocated nearly Aus$125M for national roll-out.
Conclusion
The Teletrial model offers an opportunity to create an interconnected and networked clinical trial system that affords access to patients closer to home. Scaling up of this model as routine practice of health services requires Government ownership in terms of policy and process changes, resource allocation and regulatory reform. The clinical trials industry can contribute by incorporating the ATM as a recruitment mechanism within their protocols. Implementation science frameworks offer a logical guide to successful implementation.
Footnotes
Acknowledgements
We are grateful for the support of state governments, MTP Connect, Medicines Australia and its members, Cancer Cooperative Clinical Trial Groups, Australian Teletrial Consortium partners including Rare Cancer and Cancer Voices Australia, COSA Council, and many clinical, regulatory and management colleagues and cancer centres in Australia in developing the COSA ATM and national guide and its pilot implementation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MTP connect, COSA and Teletrial Consortium Partners provided Aus$350,000 for the pilot implementation project. No funding received for authorship or publication of this article.