
Abstract
Introduction
Farmers have a high risk for depression (MDD). Preventive measures targeting this often remotely living population might reduce depression burden. The study aimed to evaluate the effectiveness of personalized telephone coaching in reducing depressive symptom severity and preventing MDD in farmers compared to enhanced treatment as usual (TAU + ).
Methods
In a two-armed, pragmatic randomized controlled trial (N = 314) with post-treatment at 6 months, farming entrepreneurs, collaborating family members and pensioners with elevated depressive symptoms (PHQ-9 ≥ 5) were randomized to personalized telephone coaching or TAU + . The coaching was provided by psychologists and consists on average of 13 (±7) sessions a 48 min (±15) over 6 months. The primary outcome was depressive symptom severity (QIDS-SR16).
Results
Coaching participants showed a significantly greater reduction in depressive symptom severity compared to TAU + (d = 0.39). Whereas reliable symptom deterioration was significantly lower in the intervention group compared to TAU + , no significant group differences were found for reliable improvement and in depression onset. Further significant effects in favor of the intervention group were found for stress (d = 0.34), anxiety (d = 0.30), somatic symptoms (d = 0.39), burnout risk (d = 0.24–0.40) and quality of life (d = 0.28).
Discussion
Limiting, we did not apply an upper cutoff score for depressive symptom severity or controlled for previous MDD episodes, leaving open whether the coaching was recurrence/relapse prevention or early treatment. Nevertheless, personalized telephone coaching can effectively improve mental health in farmers. It could play an important role in intervening at an early stage of mental health problems and reducing disease burden related to MDD.
Trial registration number and trial register
German Clinical Trial Registration: DRKS00015655
Introduction
Lifetime prevalence rates for major depressive disorder (MDD) are estimated between 2% and 21.0% worldwide. 1 MDD is associated with high individual2,3 and societal burden.4,5 Yet, primary care providers fail to recognize MDD in nearly half of patients 6 and only 20% receive specialized mental health care. 7 But even in a hypothetical scenario of full coverage and compliance to evidence-based treatments, only one-third of MDD-related disease burden could be averted.8,9 Preventive approaches are promising in reducing disease burden. According to recent meta-analyses, psychological interventions could effectively prevent MDD onset when targeting people in risk groups or with subthreshold symptoms.10,11
A recent systematic review including mostly studies from English-speaking countries showed an elevated risk in farmers for mental disorders compared to people in nonfarming occupations. 12 Farming-related risk factors include poor physical health, high workload, exposure to pesticides, financial hardship, and uncertain weather conditions. Farmers also face barriers to accessing mental health services including few providers in rural areas,12,13 preferring help from oneself, family or friends, 14 and anticipated stigma.15,16
Therefore, low-threshold preventive interventions for this vulnerable group are warranted. Telephone coaching could aid by reducing travel time and being easily accessible. One-on-one telephone interventions have been shown to be effective in supporting people with physical long-term conditions 17 and in delivering psychological interventions for depression (e.g. cognitive behavioral therapy, interpersonal psychotherapy). 18 In a recent meta-analysis, cognitive behavioral therapy delivered over phone has shown comparable outcome improvements compared to face-to-face therapy for MDD.19,20 However, for coaching conducted over the telephone, only two studies could be identified that evaluated the effectiveness in reducing depressive symptom severity and revealed moderate effects in mostly white-collar workers.21,22 Yet the overall effectiveness of telephone coaching in farmers as well as its effect on preventing MDD remains unclear.
The present study evaluated the effectiveness of telephone coaching personalized to the individual farmer's needs compared to enhanced treatment as usual in reducing depressive symptom severity and preventing MDD onset at a six-month follow-up. This study is part of a nationwide prevention project by the German social insurance for farmers, foresters, and gardeners (SVLFG), which aims to implement internet- and tele-based interventions into routine care.
Methods
The study was a two-armed pragmatic randomized controlled trial comparing the effectiveness of personalized telephone coaching delivered by a third-party independent healthcare provider “IVPNetworks” to a control group receiving information material in addition to usual care (TAU + ) at post-treatment (six months after randomization).
The trial was approved by the Medical Ethics Committee of the Friedrich-Alexander University Erlangen-Nürnberg (No. 345_18 B) and registered in the German clinical trial register (DRKS00015655). The study protocol can be found elsewhere. 23
Study population
Individuals were included if they were (a) insured by the SVLFG, (b) entrepreneur, assisting family member or pensioned farmer, (c) 18 years or older, (d) showed elevated depressive symptoms (PHQ-9≥5), (e) had internet/telephone access for online assessments/coaching, and (f) provided written informed consent.
Applicants were excluded if they were (a) currently receiving psychotherapy, (b) unwilling to sign a nonsuicide contract in case of suicidal ideation or (c) living in the German Federal States Bavaria or Schleswig-Holstein, as roll-out of the intervention into routine care was ongoing there. 24 Due to the parallel recruitment for two RCTs evaluating online trainings in the same target group,25,26 we (d) excluded participants from these studies. To mimic routine care, no diagnostic interviews were conducted.
Procedure
Participants were recruited and enrolled in the study from December 2018 to April 2019. The main recruitment channel was personal invitation letters to randomly selected insured persons. The study was also advertised in the SVLFG members’ journal and newsletter and associated websites.
Inclusion criteria were assessed online and eligible individuals who provided written informed consent and completed the baseline assessment were randomly allocated to the intervention (IG) or control group (CG) (see Figure 1).

CONSORT study flow
Randomization was centrally done at an individual level by an independent researcher not involved in the study. Permuted block randomization with randomly arranged block sizes(4,6,8,12) and an allocation ratio of 1:1 was used based on a web-based program (Sealed Envelope). Study participants and coaches could not be blinded but data collectors were blind to group allocation.
Post-assessment was assessed six months after randomization, regardless of the coaching duration, between June 2019 and December 2019. Completion was rewarded with €15 in both groups. The primary outcome was assessed via telephone if participants did not complete the assessment within two months.
Study arms
All participants had unrestricted access to routine care. Actual health service use was monitored with items of the TiC-P (see secondary outcomes).27,28
Intervention group
The study team registered participants on the management platform (IVPnet). Case managers at IVPNetworks assigned coaches to participants. Coaches were psychologists with a diploma or master's degree in psychology and trained in different psychological methods (e.g. cognitive behavioral, systemic, hypnotherapeutic), while licensed psychotherapists were available for supervision. Coaching is an individual-centered process, which is problem-based and solution-oriented. It aims to reactivate and build individuals’ resources by using psychoeducational and psychological methods to enable participants to cope with stress, acute problems, or general worries.
No fixed procedures or standardized manuals were applied in the coaching. Coaching methods varied depending on the coach's background, while timing and content were permanently adapted to the participants’ needs. As a guideline, a coaching volume of 850 min or six months was set with the possibility of prolonging for an additional 150 min or three months, respectively. If coaches identified clinically relevant symptomatology, they could support participants in finding adequate help (e.g. contact general practitioner or psychiatric clinic). Additionally, participants were supported to find on-site support services (e.g. socioeconomic or agricultural family counseling) or switch to an onsite coaching if indicated.
Control group
Participants in the control group received brief psychoeducation material on stress and depression by email, combined with information about access to regular care.
Outcomes
Primary and secondary outcomes were assessed via online questionnaires (Unipark) at baseline and post-treatment (T1).
Primary outcome
Depressive symptom severity was assessed with the German version of the Quick Inventory Depressive Symptomology (QIDS-SR16) with scores ranging from 0 to 27. Scores between 0 and 5, indicate normal health status, while those between 6–10, 11–15, 16–20, and greater than 20, indicate mild, moderate, severe, or very severe depressive symptom severity, respectively. 29 Reliability in this study was acceptable 30 with αT0 = .72 and αT1 = .78.
Secondary outcomes
Lifetime history and major depressive episodes (MDE) onset within the past year, bipolar disorder (BPD), and general anxiety disorder (GAD) were self-reported with adapted items from the web version of the Composite International Diagnosis Interview version 3.0 (CIDI). 31 For depression onset at post-treatment, both CIDI rating and a score of 13 or greater on the QIDS-SR16 as a cutoff for possible acute cases of clinical depression 32 were applied.
Secondary outcomes further included perceived stress (Perceived Stress Scale, PSS, range 0–40, αT0 = .85 – αT1 = .90), 33 insomnia severity (Insomnia Severity Index, ISI, range 0–28, αT0 = .81 – αT1 = .88), 34 somatic symptom burden (Somatic Symptom Scale, SSS-8, range 0–32, αT0 = .71 – αT1 = .76), 35 severity of GAD (GAD-7, range 0–21, αT0 = .78 – αT1 0.83),36,37 severity of panic and agoraphobic symptoms (Panic and Agoraphobia Scale, PAS, range 0–48, αT0 = .89 – αT0 = .92), 38 alcohol consumption (consumption questions from Alcohol Use Disorder Identification Test, AUDIT-C, range 0–12, αT0/1 = .59) 39 and quality of life (Assessment of Quality of Life-8D, AQoL-8D, range 0–100, αT0 = .92; αT1 = .94). 40
Work-related, the subjective capacity to work (SPE, Guttman scale categories 0–3, repT0/1 = .95) 41 as well as burnout symptomology (Maslach Burnout Inventory, MBI-GS, subscales: “Emotional Exhaustion,” EE, range 0–30; “Cynicism,” CY, range 0–30; “Professional Efficacy,” PE, range 0–36; αT0 = .70 – .89, αT1 = .77 – .91)42,43 was assessed.
A context-adapted version of the cost questionnaire “Trimbos Institute and Institute of Medical Technology Questionnaire for Costs Associated with Psychiatric Illness” (TiC-P)27,28 was used to monitor TAU.
Intervention-related outcomes
Intervention-related outcomes included satisfaction with the coaching or information material (Client Satisfaction Questionnaire for internet interventions, CSQ-I, range 8–32, αCG = .95 – αIG = .96),44–46 working alliance (Working Alliance Inventory, participants: WAI-SR, range 12–60, α = .93; coaches: WAI-SRT, range 10–50, α = .90), 47 and negative effects (Inventory for the Assessment of Negative Effects of Psychotherapy, INEP). 48 Data on the coaching process (e.g. duration, sessions, topics) were retrieved from IVPnet.
Data analyses
Based on a power of 80%, an alpha of 0.05 (two-sided), and an attrition rate of 20%,21,22 312 participants were needed to be able to detect an effect of d = 0.35 49 using an independent t-test (G*Power Version 3.1.9.2).
Results are reported according to the Consolidated Standards of Reporting Trials (CONSORT) 2010 Statement and its extension for reporting pragmatic trials. 50 Analyses were performed in R 51 based on intention-to-treat principles with a two-sided significance level of 0.05. Missing data were imputed using the R-package MICE 52 to apply Multiple Imputation by Chained Equations assuming data to be missing at random. Representing the percentage of incomplete cases at post-treatment, 21 imputed datasets were generated. 53 Intervention-related outcomes and health service use were not imputed. We used analysis of covariance (ANCOVA) to compare primary and secondary outcomes between study groups, adjusting for baseline scores. All analyses were run in each imputed data set and estimates were pooled using Rubin's Rule.54,55 Results were reported as mean within- and between-group differences and as Cohen's d effect sizes with corresponding 95% CIs according to Hedges and Olkin. 56
Treatment response, reliable deterioration, and close-to-symptom-free status
To assess improvements in the primary outcome at an individual level, we examined the number of participants who showed a treatment response as defined by a reliable change from baseline to post-treatment according to the reliable change index (RCI) of Jacobson and Truax. 57 Participants were defined as reliably improved if their QIDS-SR16 score declined from baseline to post-treatment with more than 1.96 standard units corresponding to a point change of at least 6, while taking into account the reliability of the measurement instrument. The same method was used to assess an increase in depressive symptoms to indicate reliable deterioration.
Close-to-symptom-free status was a priori defined as a score of ≤5 on the QIDS-SR16. 29 Individuals below this score at baseline were excluded from this analysis. Differences in treatment response and close-to-symptom-free status between study groups were assessed using χ2 tests. Numbers-needed-to-treat (NNT; with 95% CI) to achieve one treatment response and close-to-symptom-free status, respectively, were calculated as the inverse of the risk difference.58,59
Onset and remission of potential MDD
Group differences in depression onset were assessed with Poisson regression in the subsamples of individuals without self-reported MDE/MDD at baseline based on CIDI and QIDS-SR16 < 13, respectively, estimating incidence rate ratios (IRR) with 95% CIs. For individuals with potential MDD at baseline (QIDS-SR16≥13) group differences in remission were assessed using logistic regression. Odds Ratios (OR) and 95% CIs were reported.
Sensitivity analyses
To test the robustness of the findings, subgroup analyses were conducted with study completers. The influence of intervention (e.g. coaching duration, coaches’ background) and individual characteristics (e.g. treatment preferences) on the primary outcome was analyzed using linear regression.
Results
Participants
A total of 1347 individuals completed the screening. Two individuals who completed the baseline assessment after study N was reached were randomized by coin-flip, resulting in a total sample of 314 participants, with 160 participants in IG and 154 in CG. In IG, 24 participants (15.0%) and in CG 43 participants (27.9%) were lost to follow-up. Study completers and study dropouts did not differ in any sociodemographic or clinical baseline characteristics.
The majority of participants were male (n = 165, 52.5%), lived in partnership (n = 281, 89.5%), had middle education (n = 197, 62.7%), and were entrepreneurs (n = 197, 62.7%) with an average age of 52 (SD = 9.98, range: 25–87). Average depressive symptom severity was mild to moderate (M = 10.03, SD = 4.26), with 88 participants (28.0%) scoring ≥13 on the QIDS-SR16 (Table 1).
Baseline characteristics of the study population (N = 314).

IG: Intervention group; CG: Control group; QIDS-SR16: Quick Inventory of Depressive Symptomatology; CIDI: Composite International Diagnostic Interview; MDE: Major Depressive Episode; BPD: Bipolar Disorder; GAD: Generalized Anxiety Disorder.
Low: no formal education or lower secondary education, middle: finished upper secondary education, high: finished study or master's certificate.
Only applied to spouses and family members of entrepreneur (n = 86).
Only applied to entrepreneurs and spouses/family members with working contract in the company (n = 204).
Intervention-related outcomes
Coaches and intervention use
During the study, 34 coaches (n = 31 female, 91.2%) worked with 1–20 participants (M = 4.71, SD = 2.26). According to IVPNetworks, coaches had a background in systemic counseling (n = 18, 53.0%), cognitive behavioral methods (n = 11, 32.0%), hypnotherapy (n = 8, 24.0%), gestalt- or analytic therapy (n = 7, 20.5%), or other coaching and counseling methods (n = 19, 55.9%). Additional sociodemographic and work-related information were assessed via an online questionnaire from coaches (17/34, 50%; Supplement 1). Analyses of semistructured interviews with eight coaches revealed psychoeducation, conjoint goalsetting, and a three-phase model (“introduction and alliance building”-, “working”-, and “stabilizing”-phase) as common elements for the individualized coaching. Intervention use is displayed in Table 2.
Intervention use in the study period based on IVP Networks reporting (N = 160).
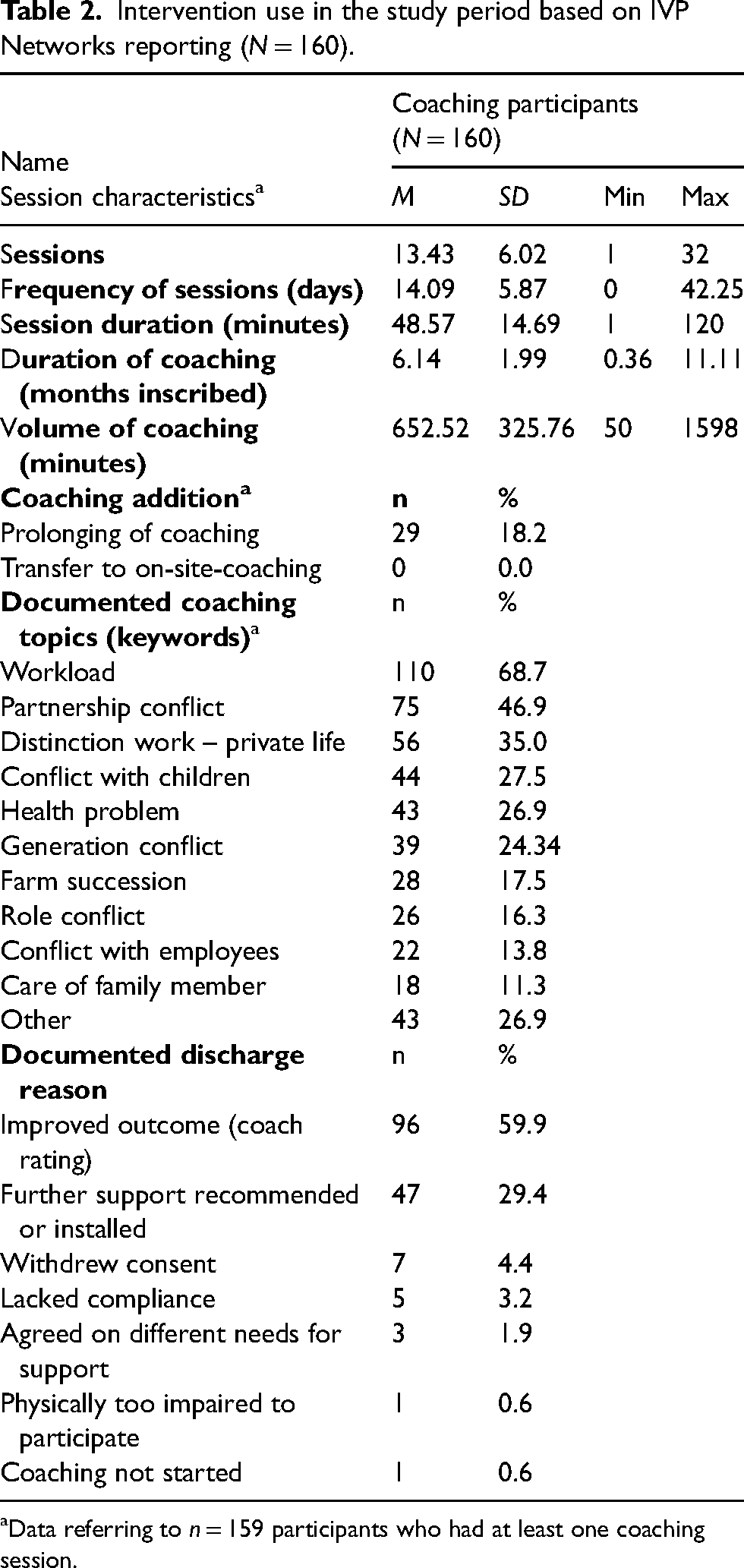
Data referring to n = 159 participants who had at least one coaching session.
Satisfaction and working alliance
Satisfaction in IG was higher (n = 135; M = 28.17, SD = 5.58) compared to CG (n = 109; M = 16.11, SD = 6.46, t(214.64) = −15.39, p < 0.001). Working alliance between coach and participant was rated as good by participants (n = 135, 84.9%, M = 4.05, SD = 0.66) and by the 17 coaches who rated a total of 86/159 (54.1%) coachings (M = 3.94, SD = 0.68).
Primary outcome
Both groups showed statistically significant reductions in depressive symptom severity indicated by changes in baseline to post-treatment scores on the QIDS-SR16 (IG: 3.37 points, SD = 4.21, t(3597) = −7.17, p < 0.001, d = −0.92 [95% CI: −0.67 to −1.17]; CG: 2.10 points, SD = 5.01, t(1793) = −3.86, p < 0.001, d = −0.50 [95% CI: −0.25 to −0.77]). Depressive symptom severity was statistically significantly reduced in IG compared to CG while adjusting for baseline symptoms (F1,306.54 = 12.78, p < 0.001) corresponding to a small to medium between-group effect size of Cohen's d = −0.39 [95% CI: −0.15 to −0.64].
Treatment response, symptom deterioration, and close-to-symptom-free status
Treatment response was observed in more participants in IG (58/160 = 36.3%) than in CG (44/154 = 28.6%) but without statistical significance (χ2 = 2.11, p = 0.16; NNT = 13.02, 95% CI: −38.71 to 5.57). In IG, statistically significantly more participants achieved a close-to-symptom-free status (61/140 = 43.6%) compared to CG (37/133 = 27.8%; χ2 = 7.35, p = 0.007; NTT = 6.35, 95% CI: 3.72–21.70). A significant difference was observed in reliable deterioration with one case (0.6%) in IG and nine cases (5.8%) in CG (χ2 = 6.4, p = 0.02).
Secondary outcomes
Onset and remission of depression
Based on CIDI (n = 260), 15 cases (6.6%) of possible MDE onset were observed in CG compared to six cases (2.7%) in IG (IRR = 0.39, 95% CI: 0.14–1.09, p = 0.07). Likewise, no group difference was observed in potential MDD cases based on QIDS-SR16 (n = 226) with eight (3.5%) and four (1.8%) new cases of potential MDD in CG and IG, respectively (IRR = 0.36, 95% CI: 0.10–1.36, p = 0.13).
No statistically significant difference between groups in remission (IG: nbaseline = 40, npost = 11, 27.5% remission, CG: nbaseline = 48, npost = 22, 45.8% remission; OR = 1.84, 95% CI: 0.66–5.42, p = 0.27) was observed.
Other mental health outcomes
Analyses yielded significant differences in favor of IG for perceived stress (d = −0.34, 95% CI: −0.08 to −0.59), generalized anxiety (d = −0.30, 95% CI: −0.07 to −0.53), somatic symptoms (d = −0.39, 95% CI: −0.16 to −0.63), dimensions of the Maslach burnout inventory (EE: d = −0.28, 95% CI: −0.05 to −0.51; PE: d = 0.4, 95% CI: 0.64–0.16; CY: d = −0.24, 95% CI: 0 to −0.47), and quality of life (d = 0.29, 95% CI: 0.52–0.06) (Table 3).
Primary and secondary outcomes at 6-month post-treatment (N = 314).
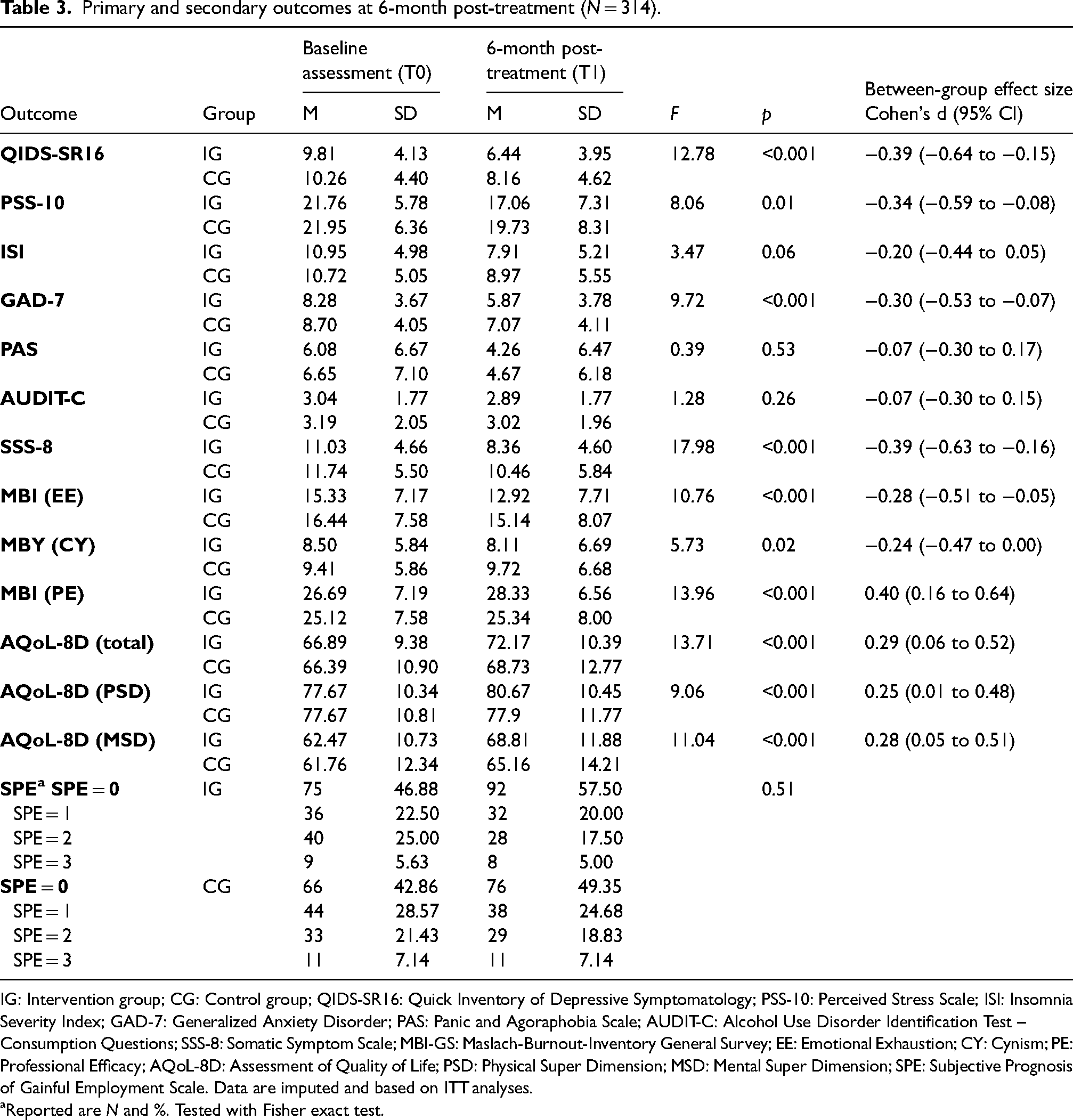
IG: Intervention group; CG: Control group; QIDS-SR16: Quick Inventory of Depressive Symptomatology; PSS-10: Perceived Stress Scale; ISI: Insomnia Severity Index; GAD-7: Generalized Anxiety Disorder; PAS: Panic and Agoraphobia Scale; AUDIT-C: Alcohol Use Disorder Identification Test – Consumption Questions; SSS-8: Somatic Symptom Scale; MBI-GS: Maslach-Burnout-Inventory General Survey; EE: Emotional Exhaustion; CY: Cynism; PE: Professional Efficacy; AQoL-8D: Assessment of Quality of Life; PSD: Physical Super Dimension; MSD: Mental Super Dimension; SPE: Subjective Prognosis of Gainful Employment Scale. Data are imputed and based on ITT analyses.
Reported are N and %. Tested with Fisher exact test.
Negative effects
Based on the INEP, one-third of IG participants (47/135, 34.8%) reported at least one negative effect attributed to the intervention. In total, 82 negative effects were reported of which most were “intrapersonal changes” (n = 33, 40.2%, Supplement 2).
Use of TAU
Overall, more participants in IG (n = 97, 71.3%) reported use of at least one health service (Table 4) during the last three months compared to CG participants (n = 63, 56.8%, χ2(1) = 5.06, p = 0.02).
Use of psychosocial and (mental) health services in the study population according to corresponding items of Tic-P (study-completer only, n = 247 at post-assessment).
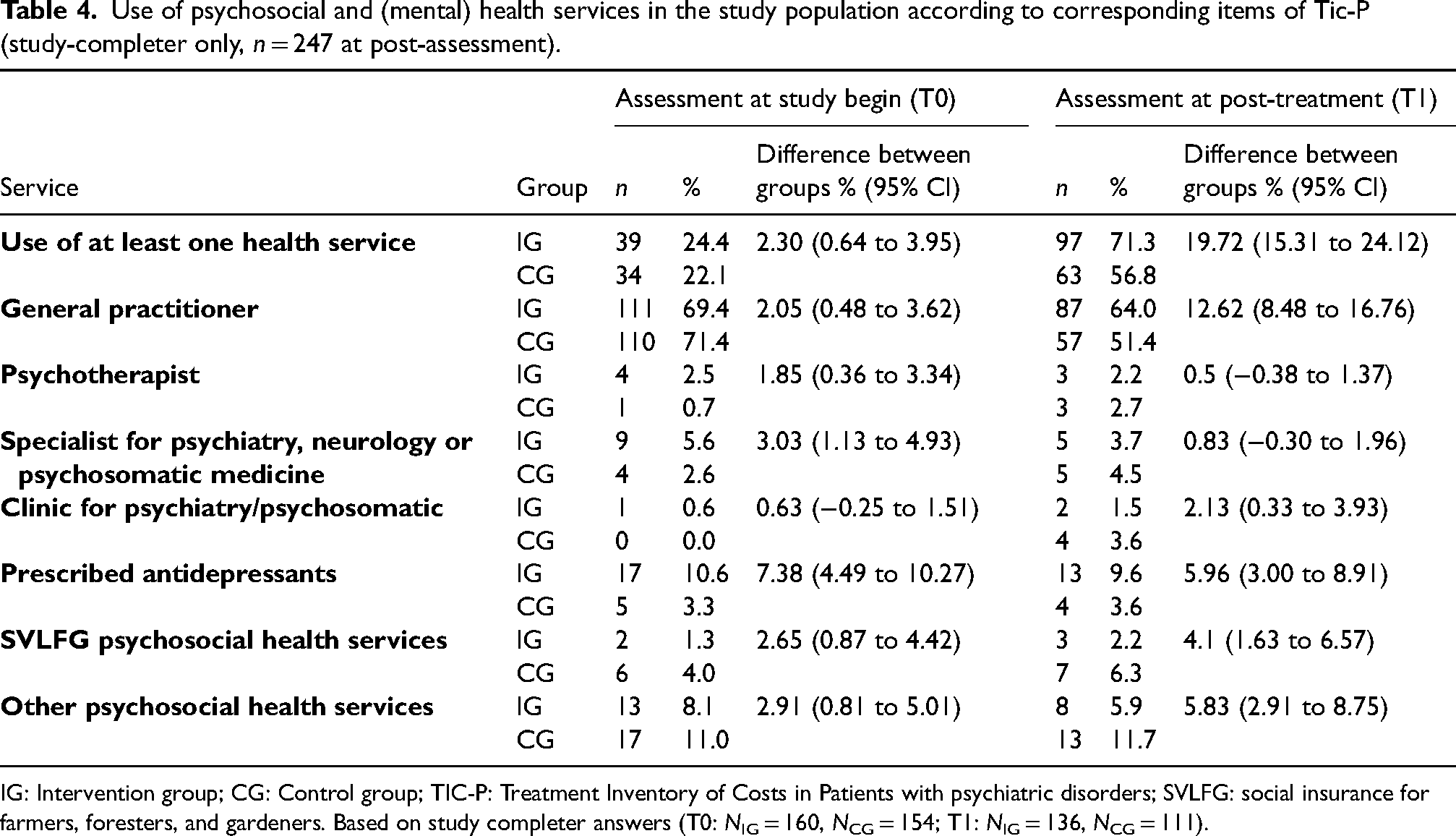
IG: Intervention group; CG: Control group; TIC-P: Treatment Inventory of Costs in Patients with psychiatric disorders; SVLFG: social insurance for farmers, foresters, and gardeners. Based on study completer answers (T0: NIG = 160, NCG = 154; T1: NIG = 136, NCG = 111).
Sensitivity analyses
Analyses of the study completer (n = 247, 78.7%) showed that outcomes remained comparable with greater effect sizes compared to the main analyses (Supplement 3). Additionally, small effects of an increased reduction in insomnia (d = −0.22 [95% CI: −0.47 to 0.03]) and panic and agoraphobic symptoms (d = −0.3 [95% CI: −0.6 to 0.01]) were found in IG compared to CG.
Baseline depressive symptom severity and coaching duration were uncorrelated (r = 0.12, p = 0.11) but baseline symptom severity predicted depressive symptoms at post-treatment (β = 0.51, t(111) = 7.35, p < 0.0001, R2 = 0.29 [95% CI: 0.17–0.42]; Supplement 3).
Discussion
We reported the post-treatment results from a pragmatic randomized controlled trial comparing a personalized telephone coaching to a control group receiving brief psychoeducational material. Coaching participants showed a significantly greater reduction in depressive symptom severity (d = −0.39, 95% CI: −0.64 to −0.15) compared to CG. No significant differences in reliable symptom improvement and depression onset were observed, but coaching led to fewer reliable deteriorations compared to CG. Positive effects in favor of IG were also shown for stress, anxiety, somatic symptoms, burnout risk, and quality of life.
To our knowledge, this is the first trial for personalized preventive telephone coaching targeting depressive symptoms in farmers. The observed reduction in depressive symptoms is comparable to previous findings for indicated depression prevention with effect sizes reported at post-treatment as d = 0.35 (95% CI: −0.23 to −0.47) for face-to-face interventions, 49 d = −0.39 (95% CI: −0.25 to −0.53) for general online interventions, 60 and d = −0.28 (95% CI: −0.50 to −0.07) for guided online-interventions for farmers. 61 The average intervention duration of 13 sessions over six months in this study is higher compared to most online trainings (6–12 sessions, 3–12 weeks) 60 but similar to preventive health coaching (1–20 sessions, 1–24 weeks) 62 and face-to-face interventions in subthreshold (5–16 session) 10 and major depression (3–24 sessions, 3–36 weeks). 63 Studies on telephone coaching based on cognitive behavioral therapy or motivational interviewing for adults with MDD reported slightly higher effect sizes for symptom reduction with d = −0.76 (95% CI: −0.40 to −0.80) at four months 21 and d = −0.45 (95% CI: −0.14 to −0.75) at 12 months. 22
Regarding the nonsignificant group differences in MDE onset, three potential reasons should be considered. First, overall onset rates at post-treatment were low in both groups (CG: 12.0%, IG: 4.4% based on CIDI). Onset rates for nonactive control groups are reported with incidence rates of 25%–30% in (indicated) prevention over 12 months.10,60 As shown by Reins et al. 60 depression onset in subclinical control conditions occurred on average eight months after study enrolment. Thus, our follow-up period might have been too short to observe group differences in depression onset. Second, our control group was not completely inactive but received psychoeducational material about stress, depression, and healthcare services. Yet, brief psychoeducational interventions can result in depressive symptom reduction. 64 Third, the study was powered to detect statistically significant differences in depressive symptom severity, which might not have been sufficient to detect differences in MDD onset.
The recent Covid-19 pandemic has increased the demand and use of telehealth services rapidly.65–67 Although the increased exposure to telehealth options might have positively influenced the attitudes of practitioners an users,68,69 it also revealed that telehealth is still considered a more niche intervention option in many countries resulting in a lack of training of heath care professionals and reimbursement opportunities.70–72 In line with other (pre-)pandemic studies, our results show that telephone coaching can effectively promote mental health, not only as a necessity in a global health crisis but also in easing access for remotely living communities, 73 lowering socioeconomic costs,74,75 and offering alternatives for people with restricted (broadband) internet access.75–77 Implementing a structure for telehealth in routine care can further strengthen and enable the health care system to spontaneously and flexibly react to future large-scale health crisis.67,71,72
Limitations
We neither applied a cutoff on self-reported depression nor conducted diagnostic interviews at baseline in order to mimic routine care. Thus, around a third of included individuals were potential MDD cases and about a quarter of participants reported lifetime MDE. The telephone coaching might therefore have functioned as recurrence/relapse prevention or (early) treatment. Future studies should clarify whether telephone coaching is equally effective in the prevention of first depression onset, prevention of recurrence/relapse, and early treatment, respectively.
Although we evaluated the coaching as a depression prevention intervention and included participants with at least mild depressive symptoms, we did not exclude participants with comorbid symptoms. Due to the personalized approach, coaches and participants might have agreed to focus on other symptoms. This might partly explain why only 36% (n = 113) of participants showed a treatment response, a finding similar to other studies on online indicated prevention 60 and preventive face-to-face interventions. 49 Treatment response might be especially critical for this target group in order to avoid an even greater reluctance to seek professional help. 78 Nonresponse can lead to (early) dropout. 79 However, early termination of telephone coaching was low in this study (n = 17/160, 10.6%), which might be due to the low-threshold telephone delivery 80 or because of the personalized approach.
Nevertheless, the highly personalized intervention and diverse coaches’ backgrounds restrict the generalizability of the intervention effects. More research on preventive (telephone) coaching on mental health outcomes is needed, especially to determine effective methods and effects of personalization. 81
Finally, the assumed advantage of telephone coaching making health care more accessible might have been limited due to study-specific inclusion criteria (e.g. internet access). The multistage inclusion procedure for study participation might have resulted in the inclusion of highly motivated participants.
Conclusion
Personalized telephone coaching can effectively reduce depression symptoms and improve mental health in farmers. It could play an important role in intervening at an early stage of mental health problems and if needed facilitating access to further support (e.g. psychotherapy, farming specific offers) which is especially crucial in rural areas and populations with low help-seeking behavior. Long-term (cost)-effectiveness analyses and the evaluation of the implementation into routine care will gain more insight into the potential of telephone coaching in this population.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X221106027 - Supplemental material for Telephone coaching for the prevention of depression in depression in farmers: Results from a pragmatic randomized controlled trial
Supplemental material, sj-docx-1-jtt-10.1177_1357633X221106027 for Janika Thielecke, Claudia Buntrock, Ingrid Titzler, Lina Braun, Johanna Freund, Matthias Berking, Harald Baumeister and David D. Ebert by Telephone coaching for the prevention of depression in depression in farmers: Results from a pragmatic randomized controlled trial in Journal of Telemedicine and Telecare
Footnotes
Acknowledgements
The authors would like to thank Friederike Dietz and Annika Montag for programming the online surveys. Further, the authors thank Sarah Banellis, Merle Bloom, Hanna Böckeler, Albina Chafisuf, Doro Dressel, Johanna Finitzer and Tomris Ohloff for their engagement in enrolling and supporting participants throughout the study. Lukas Fuhrmann and Marvin Franke are thanked for carrying out the randomization and Mathias Harrer for statistical advice. The authors thank the IVPNetworks staff who provided details on their intervention and Madison Ehmann for proofreading the manuscript as well.
Authors’ contributions
Janika Thielecke: Conceptualization, Methodology, Project administration, Investigation, Data Curation, Formal analysis, Visualization, Writing – Original Draft; Claudia Buntrock: Supervision, Conceptualization, Methodology, Writing – Original Draft; Ingrid Titzler: Project administration, Conceptualization, Methodology, Writing – Review & Editing; Lina Braun: Resources, Writing – Review & Editing; Johanna Freund: Resources, Writing – Review & Editing; Harald Baumeister: Resources, Conceptualization, Funding acquisition, Writing – Review & Editing; Matthias Berking: Funding acquisition, Writing – Review & Editing; David Daniel Ebert: Funding acquisition, Conceptualization, Methodology, Writing – Review & Editing. All authors provided critical revision of the article and approved the final manuscript.
Data availability
Access to the final pseudonomized trial dataset can be provided to fellow researchers upon request, depending on to be specified data security and data exchange regulation agreements.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DDE has served as a consultant to/on the scientific advisory boards of Sanofi, Novartis, Minddistrict, Lantern, Schoen Kliniken, Ideamed, and German health insurance companies (BARMER, Techniker Krankenkasse) and a number of federal chambers for psychotherapy. DDE and MB are stakeholders of the Institute for health training online (GET.ON/HelloBetter), which aims to implement scientific findings related to digital health interventions into routine care. MB is scientific advisor of mentalis GmbH, a provider for digital aftercare. HB reports having received consultancy fees and fees for lectures/workshops from chambers of psychotherapists and training institutes for psychotherapists in the e-mental-health context. IT reports having received fees for lectures/workshops in the e-mental-health context from training institutes for psychotherapists. She was the research and implementation project lead of the trial site Institute for health training online (GET.ON) for the European implementation research project ImpleMentAll (11/2017-03/2021) funded by the European Commission.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The German insurance company SVLFG provided a financial contribution to the Friedrich-Alexander Universität Erlangen-Nürnberg and Ulm University as expense allowance. SVLFG had no role in study design, data collection, analyses, interpretation or writing the manuscript and the decision to publish it.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.