
Abstract
Introduction
Isolated spaces impair communication and teamwork during tracheal intubation (TI) in suspected coronavirus disease 2019 patients. We thus aimed to evaluate the telemedicine-assisted airway model (TAM) to improve communication and teamwork during the pandemic.
Methods
This two-stage prospective study included adult patients intubated in the emergency department of the National Taiwan University Hospital between 1 August 2020 and 31 July 2021. First, we randomised patients receiving TI in the standard setting into the conventional group (Con-G) and the isolation area into the isolation group (Iso-G). We evaluated the obstacles to communication and teamwork in an isolation scenario. Second, we developed the TAM to facilitate communication and teamwork between staff in separate spaces during TI and assigned patients to the TAM group (TAM-G). Communication and teamwork were evaluated using the Team Emergency Assessment Measure (TEAM). Subjective evaluations were conducted using a questionnaire administered to medical staff.
Results
Eighty-nine patients were enrolled: 17, 34, and 38 in the Con-G, Iso-G, and TAM-G, respectively. The communication frequency (CF) of the Con-G and Iso-G was the highest and lowest, respectively. The CF of the TAM-G increased and approached that of the Con-G. The overall TEAM score was the highest in the Con-G and the lowest in the Iso-G, while the overall score in the TAM-G was comparable to that of the Con-G.
Discussion
The TAM may improve communication and teamwork for TIs without compromising efficacy during the pandemic. This study was registered at ClinicalTrials.gov; registration numbers: NCT04479332 and NCT04591873.
Keywords
Introduction
Since early 2020, coronavirus disease 2019 (COVID-19) has posed significant challenges worldwide. 1 Severe acute respiratory syndrome coronavirus 2 can be transmitted through droplets, aerosols, and close contact, even during the early stages of the disease.2,3 The COVID-19 Treatment Guidelines Panel of the National Health Institute recommends that healthcare workers who perform aerosol-generating procedures (AGPs) on patients with COVID-19 should use an N95 respirator and other personal protective equipment (PPE) to protect themselves from infection. 4 Moreover, it is recommended that AGPs be conducted in a negative pressure room to lower the risk of cross-contamination between rooms and infection of staff and patients outside the room.
Since tracheal intubation (TI) is an AGP that poses a greater risk of infection to healthcare workers, 5 it is challenging to maintain good teamwork and communication when intubating patients in isolation areas. Non-technical skills, such as teamwork and communication, are critical in managing TI and are associated with improved outcomes in emergent airway management. Guidelines have highlighted the role of the airway team, a shared mental model, planning, and communication throughout airway management. 6 However, limited personnel in the negative pressure room makes intubation less efficient than in standard scenarios. Additionally, muffled voices and impaired hearing due to PPE also compromise communication between the team members.
Telemedicine and telehealth have been extensively used in the delivery of medical care,7–10 and emphasised in the COVID-19 pandemic.11,12 Video consultations have been promoted to reduce the risk of disease transmission and improve infection control.13–15 The application of telemedicine by medical personnel as a tool to facilitate communication has also been studied. 15 Innovative applications of telemedicine in TI in rural emergency departments (EDs) have also been reported. 16 However, limited studies have examined the feasibility, safety, and efficacy of teleguidance-facilitated TI, especially during a pandemic. 17
The objective of the current study was to identify the impact of environmental factors (different rooms, separate spaces, and tight PPE) on TI and to evaluate the efficacy, safety, teamwork, and communication of the telemedicine-assisted airway model (TAM) on emergent TI.
Methods
Study design and participants
This two-stage prospective study was conducted from 1 August 2020 to 31 July 2021. The study design was sequential randomisation in Stage 1 and a pre–post-test design in Stage 2. In Stage 1, the enrolled patients were sequentially randomised with a 1:1 allocation into the conventional group (Con-G) or the isolation group (Iso-G). In Stage 2, the patients were assigned into two groups, before and after the TAM started. The National Taiwan University Hospital is a 2700-bed teaching hospital that provides primary and tertiary care. It was designated a COVID-19 response hospital in Taiwan. Before the pandemic outbreak, the average number of emergency visits was approximately 250 per day. Adult patients aged >20 years who were intubated because of acute respiratory failure during the study period were enrolled for the study. Written informed consent was obtained from the participants in Stage 1, and verbal informed consent was obtained from those in Stage 2. Patients with cardiac arrest or trauma were excluded from this study (Figure 1). The study was approved by the Institutional Review Board of the National Taiwan University Hospital (NTUH; REC Nos. 202005094RIND and 202007114RINA).
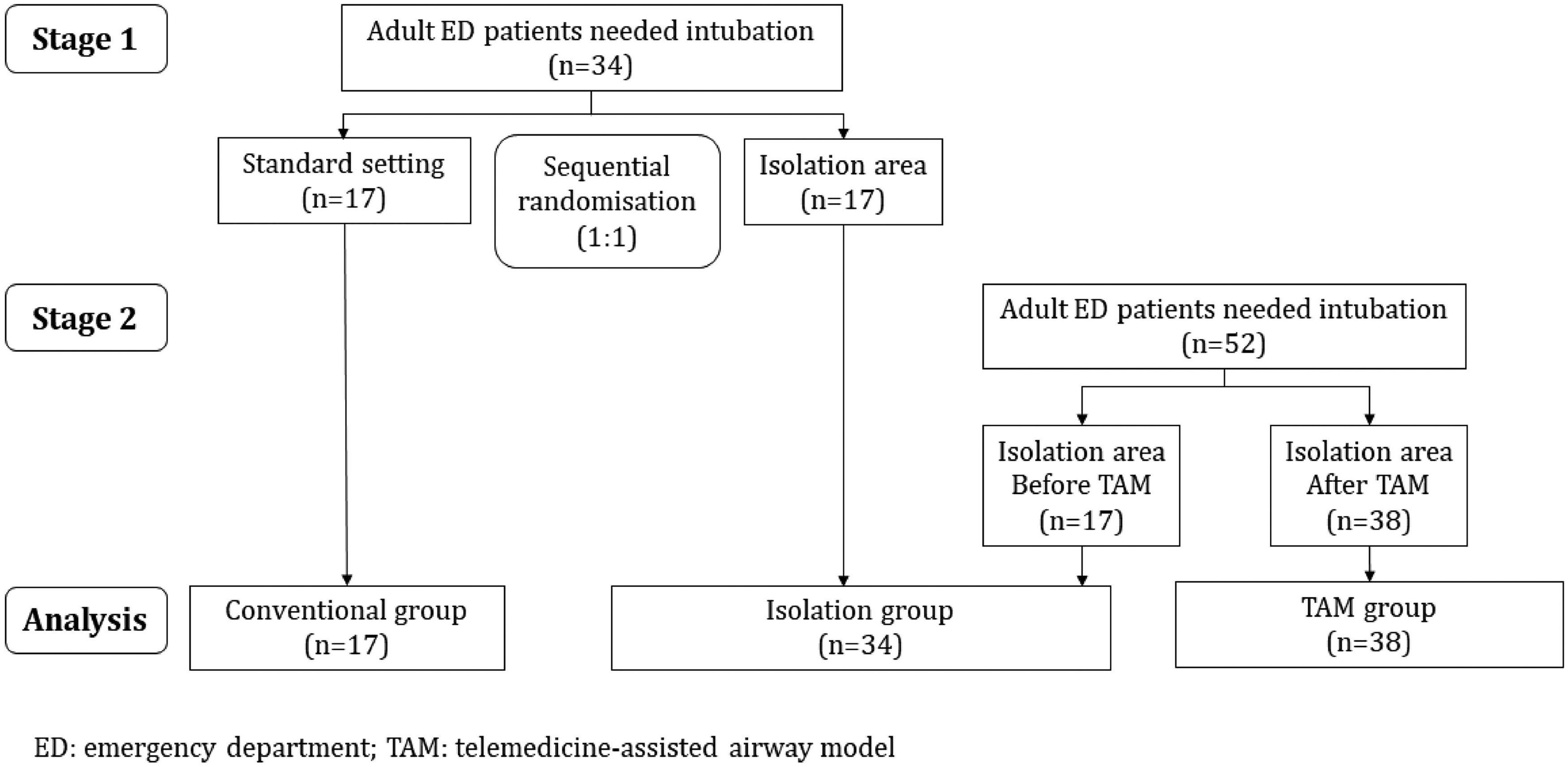
Flowchart of patient disposition.
Procedures: TI in the standard setting and isolation area
In Stage 1, we enrolled patients who required TI because of acute respiratory failure and sequentially randomised them into the Con-G or the Iso-G (Figure 1). The patients in the Con-G were intubated in one room with all TI team members working in the same (Figure 2A). Intubators and assistants (airway team) donned full AGP PPE (including an N95 face mask, waterproof gown, non-disposable face shield, hair cap, shoe sleeves, and two layers of gloves) to perform intubation. Other team members donned surgical masks, gloves, and gowns. The patients in the Iso-G were intubated in the isolation area, which had an anteroom and a negative pressure room. The TI team members were separated into different spaces: two airway team members in the negative pressure room, one support team member in the anteroom, and a leader with the rest of the team in the central station (Figure 2B). The airway and support team members were requested to don full AGP PPE, while other team members took the usual universal precautions. Communication between the different spaces was facilitated by an intercom. The TI procedures were the same in both groups.

The illustration of the airway team, support team, and the other tracheal intubation team members in three study groups. (a) Conventional group. All the team members were in the same space. (b) Isolation group. The airway team members were in the negative pressure room; the support team member was in the anteroom; the leader and the other tracheal intubation team members were in the nonnegative pressure central station. (c) Telemedicine-assisted airway model group. The location of each member was the same as that in the isolation group.
Procedures: TI in the TAM
In Stage 2, we set up a teleconferencing system in the isolation area and developed the TAM to improve communication and teamwork among the TI team members (Figure 2C). Our TAM used Cisco Webex® software (Cisco Systems Inc., San Jose, CA, USA). The teleconferencing system protects the privacy and security of patient data using end-to-end encryption and data transmission through an intranet governed by the firewall of the hospital information system. The system complied with government telemedicine regulations. All team members in the TAM remained in individual spaces in the isolation area and were virtually connected through the teleconferencing system. They share information, give orders, and instantly respond to each other via the teleconferencing system. They also hear the sounds and see the images of each space, particularly the process of TI. Additionally, the leader could share the patient's information on the screen from the central station. Before implementing the TAM, we recruited 13 senior emergency physicians, 26 ED residents, and 75 nurses in charge of the critical care station to join the Stage 2 study as the TAM team. The participants were trained on the TAM. The PPE requirement for the TAM was the same as that for the Iso-G. The TAM started in May 2021 (the greatest surge of COVID-19 in Taiwan), and patients who had been intubated since then were enrolled in the TAM group (TAM-G; Figure 1). The entire TI process of the enrolled patients was video recorded. All patients in our study were intubated with a video laryngoscope.
Outcomes
The primary outcome was the intubation time (IT), indicating the efficacy of emergent TI. IT was measured from the start of intubation to the confirmation of the correct position of the endotracheal tube with continuous waveform capnography. The number of intubation attempts (IAs) was also analysed to assess efficacy. The secondary outcomes were safety, communication, and teamwork during emergent TI. AGP exposure time, defined as the time from the start of preoxygenation to the confirmation of endotracheal tube position, was calculated to assess safety. The number of conversations during the procedure divided by the AGP exposure time was used to indicate communication frequency (CF). Three emergency physicians experienced in resuscitation teamwork independently reviewed the video recordings to assess teamwork. They used the Team Emergency Assessment Measure (TEAM), a valid, reliable, and feasible tool for assessing emergency resuscitation teams’ performance and objectively grading their non-technical skills.18,19 The TEAM score has 12 items and uses a 5-point Likert scale (0 = never or hardly ever to 4 = always/nearly always).
Subjective perceptions of communication and teamwork between the groups were also evaluated. A survey was conducted after each intubation task for each medical staff member, using a 16-item questionnaire to assess the subjective perception of communication and teamwork during TI (Supplemental Material Table S1). The questionnaire was modified to evaluate telemedicine communication satisfaction. 20 The level of agreement was assessed using a 5-point Likert scale ranging from 1 (strongly agree) to 5 (strongly disagree). The questionnaire was validated by four emergency physicians and one senior ED nurse.
Statistical analysis
We did the power analysis and sample size calculation according to the previous observation of TIs in our ED. In Stage 1, we assumed that the mean and standard deviation (SD) of IT was 5 ± 1.5 min in the Con-G and 7 min in the Iso-G, the α-value was 0.05, and the power was 0.8, the estimated sample size was 17 in each group. In Stage 2, we assumed that the mean and SD of AGP exposure time was 12 ± 3 min in the Iso-G and 10 min in the TAM-G, the α-value was 0.05, the power was 0.8, and the estimated sample size was 35 in the Iso-G and TAM-G, respectively. Descriptive statistics were presented using numbers and percentages for categorical variables and medians with interquartile ranges for continuous variables. The teamwork evaluations and questionnaires were presented as the mean and SD. For group comparisons, Fisher's exact test or Pearson's chi-square test was used for categorical variables, and a one-way analysis of variance was used for continuous variables. Statistical significance was defined as a two-sided p-value <0.05. Inter-rater reliability was evaluated using intra-class correlation coefficient estimates, and 95% confidence intervals were based on average measures from the absolute agreement two-way mixed-effects model. Values <0.5 indicate poor reliability, those between 0.5 and 0.75 indicate moderate reliability, those between 0.75 and 0.9 indicate good reliability and those >0.90 indicate excellent reliability. 21 All statistical analyses were performed using SPSS Statistics for Windows, version 16.0 (SPSS Inc., Chicago, IL, USA). This study was registered at ClinicalTrials.gov, Registration nos. NCT04479332 and NCT04591873.
Results
In Stage 1, 34 patients were randomised, including 17 patients in the Con-G and 17 in the Iso-G. In Stage 2, 17 patients were enrolled in the Iso-G before implementing the TAM. A total of 34 patients were enrolled in the Iso-G for analysis. After the launch of the TAM, 38 patients were enrolled in the TAM-G. Overall, 89 patients were included in the analysis, with 17 in the Con-G, 34 in the Iso-G, and 38 in the TAM-G (Figure 1). The clinical characteristics of the enrolled patients are presented in Table 1. The enrolled patients’ age, sex, and comorbidities (except malignancy) were not significantly different between the groups. The percentage of patients triaged as Taiwan Triage and Acuity Scale Level I was higher in the TAM-G than in the Con-G and Iso-G (Con-G: 41.2% vs. Iso-G: 41.2% vs. TAM-G: 73.7%; p = 0.01), which may have been caused by a change in the triage policy during the COVID-19 outbreak in May 2021 in Taiwan. If a patient with suspected COVID-19 required oxygen therapy, the patient would be triaged as Level I and treated in the isolation area. Meanwhile, no significant discrepancies were observed in the ED diagnosis, use of premedication and paralytic agents for intubation, severity of the patients assessed by inotropes before intubation, and Sequential Organ Failure Assessment scores. For the TI team members, the ages of all participants and intubators were not significantly different between the groups. Neither the clinical experience of the participants nor that of the intubators differed between the groups.
Characteristics of the patients and the intubation team between groups.
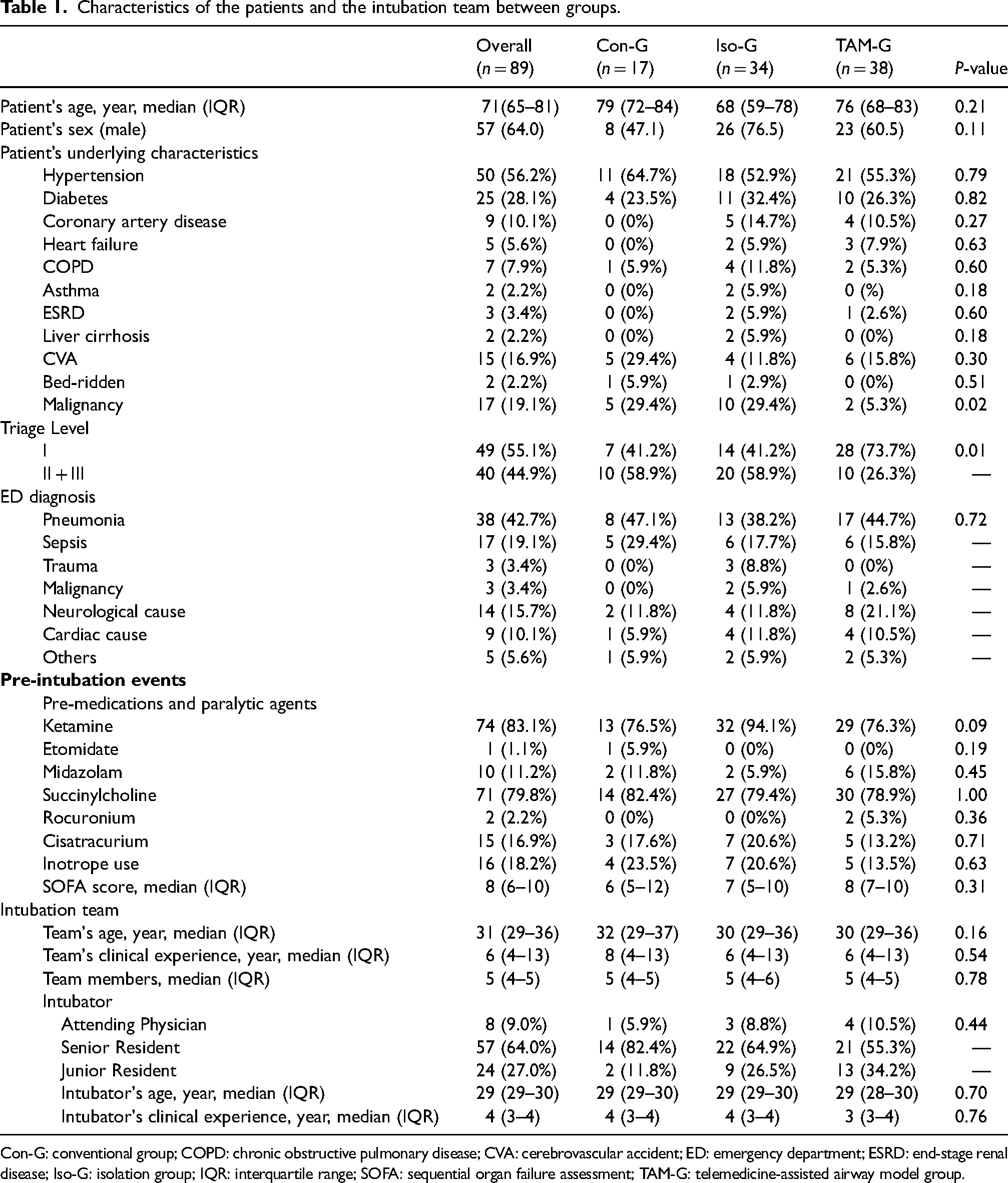
Con-G: conventional group; COPD: chronic obstructive pulmonary disease; CVA: cerebrovascular accident; ED: emergency department; ESRD: end-stage renal disease; Iso-G: isolation group; IQR: interquartile range; SOFA: sequential organ failure assessment; TAM-G: telemedicine-assisted airway model group.
For the assessment of TI efficacy and safety, neither the IA (Con-G: 1 [1–2] vs. Iso-G: 1 [1–2] vs. TAM-G: 1 [1–1]; p = 0.53) nor the IT (Con-G: 70 s [50–113] vs. Iso-G: 64 s [39–240] vs. TAM-G: 51 s [38–80]; p = 0.27) were significantly different between the groups (Table 2). The AGP exposure time, a surrogate indicator of infection risk, showed no difference between the groups (Con-G: 279 s [192–436] vs. Iso-G: 308 s [187–586] vs. TAM-G: 276 s [176–412]; p = 0.62). However, the CF differed significantly between the groups. While the CF decreased significantly in the Iso-G when compared with the Con-G, the CF of the TAM-G increased to a level close to that of the Con-G (Con-G: 1.7 [1.3–1.8] times/min vs. Iso-G: 0.4 times/min [0.5–0.9] vs. TAM-G: 1.4 times/min [1.1–1.8]; p < 0.001; Table 2).
The intubation events between groups.

AGP: aerosol-generating procedure; Con-G: conventional group; Iso-G: isolation group; IQR: interquartile range; TAM-G: telemedicine-assisted airway model group.
The TEAM scores for each group are presented in Table 3. The inter-rater reliability was 0.91. The ratings of leadership items were highest in the Con-G and lowest in the Iso-G; furthermore, they were nearly comparable between the Con-G and TAM-G. Similar trends were observed in teamwork. The ratings of item 3 (The team communicated effectively), item 4 (The team worked together to complete the tasks in a timely manner), item 8 (The team monitored and reassessed the situation), and item 9 (The team anticipated potential action) were highest in the Con-G, lowest in the Iso-G, and improved in the TAM-G compared to the Iso-G. The Con-G had the highest overall teamwork rating, whereas the Iso-G had the lowest. The TAM-G had a significantly improved rating compared to that of the Iso-G.
The TEAM score between groups.
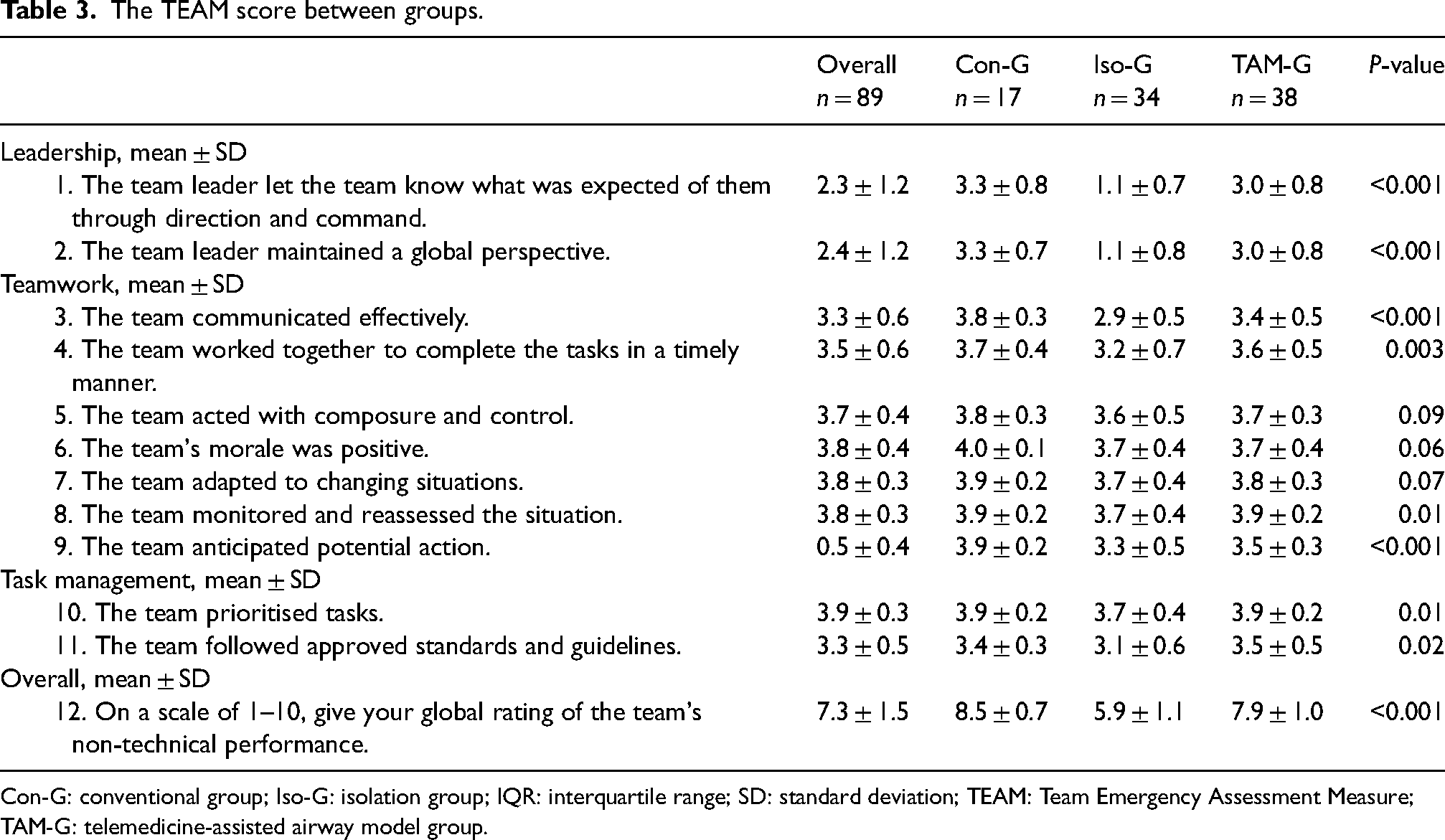
Con-G: conventional group; Iso-G: isolation group; IQR: interquartile range; SD: standard deviation; TEAM: Team Emergency Assessment Measure; TAM-G: telemedicine-assisted airway model group.
For the subjective evaluation of communication and teamwork using the questionnaire, a total of 412 persons were involved in the TI process of 89 patients, and 406 (98.5%) responded to the survey. A comparison of the survey of different roles of the TI team between the groups is shown in Supplemental Material Table S1. The percentage of participants who agreed or strongly agreed that they could hear one another clearly (Question 1) was higher in the Con-G and TAM-G than in the Iso-G, regardless of the leaders, airway team members, or other members (Figure 3A). More participants in the Iso-G agreed or strongly agreed that they had to speak loudly to be heard in different spaces (Question 4) than those in the Con-G and TAM-G did (Figure 3B). The satisfaction with communication tools (Question 6) rated by all participants was highest in the TAM-G, followed by the Con-G and Iso-G (Figure 3C). Regarding teamwork, a higher percentage of participants in the Con-G and TAM-G than in the Iso-G agreed or strongly agreed that they could easily monitor the patient's clinical status (Question 12) and receive support from other spaces when needed. This was higher in the Con-G and TAM-G than in the Iso-G, regardless of the leaders, airway team members, or other members (Figure 3D and E). The overall teamwork ratings (Question 16) by the leaders showed the highest score in the Con-G, followed by the TAM-G and Iso-G (mean ± SD, Con-G: 4.4 ± 0.7 vs. Iso-G: 2.7 ± 1.2 vs. TAM-G: 4.0 ± 0.8; p = 0.001). The ratings for the same question by the airway team and other team members showed nearly comparable scores in the Con-G and TAM-G, which were higher than those in the Iso-G (Figure 3F).
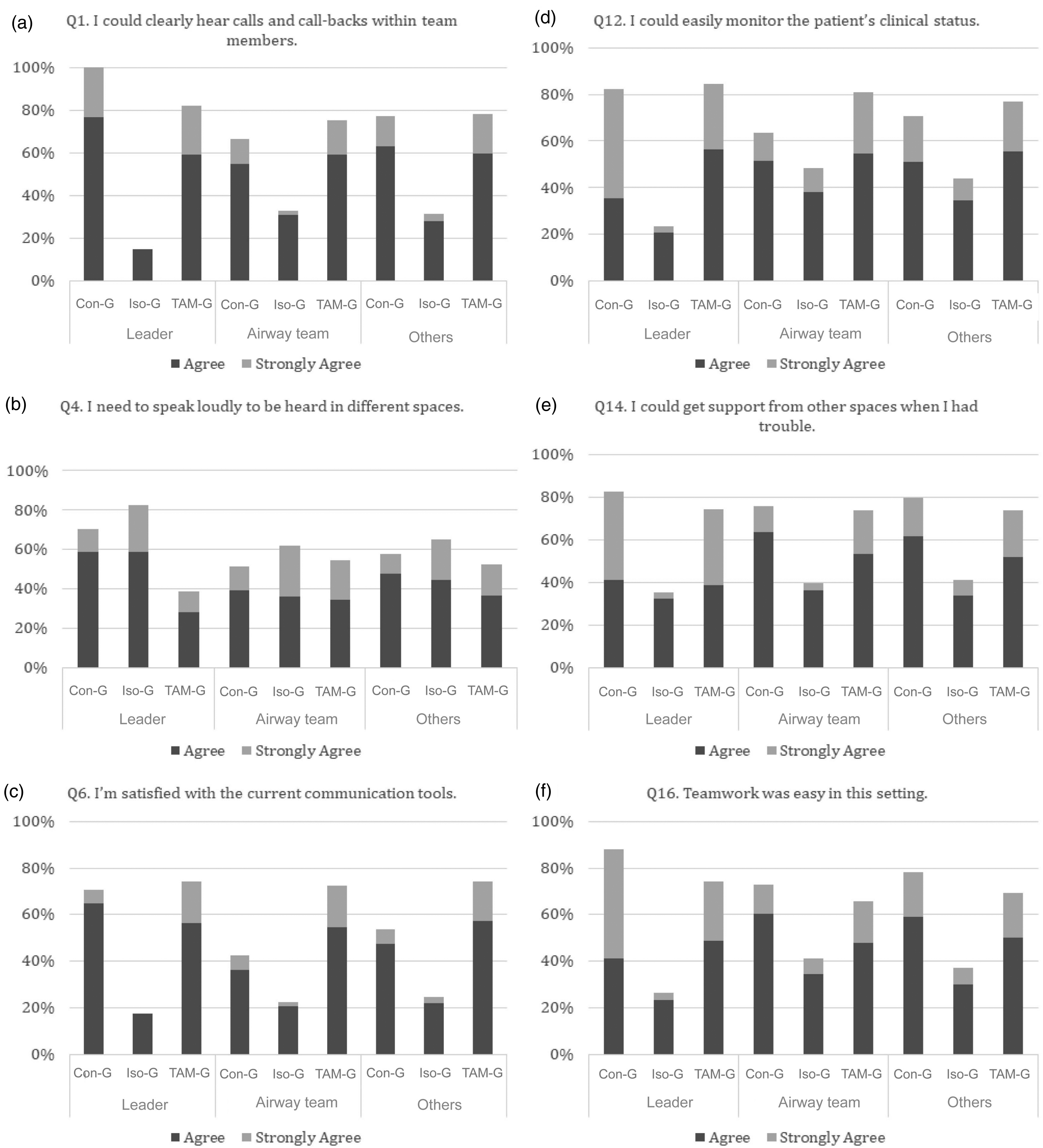
The results of the subjective evaluation of communication and teamwork using the questionnaire. The percentages of ‘agreed’ and ‘strongly agreed’ of questions 1, 4, 6, 12, 14, and 16 are shown. (a) I could clearly hear calls and call-backs within team members. (b) I need to speak loudly to be heard in different spaces. (c) I’m satisfied with the current communication tools. (d) I could easily monitor the patient's clinical status. (e) I could get support from other spaces when I had trouble. (f) Teamwork was easy in this setting.
Discussion
The current study showed that environmental changes for infection control during the COVID-19 pandemic could impair communication and teamwork during emergent TIs. For patients who need emergent TI, the healthcare workers had to struggle with PPE-related restricted mobility and vision and fragmented teamwork and communication resulting from poor coordination between team members in separate spaces while performing TI. 22 However, implementing the TAM may ameliorate interference to communication and teamwork during TI and preserve the efficacy of the life-saving procedure.
The guidelines for the management of TI in critically ill adults proposed by the Difficult Airway Society in the UK mention that human factors, such as environmental influences, team behaviours, and individual performance, are critical in TI. 6 The isolation area is not designed primarily for airway management. During the pandemic, the airway trolley was placed near the entry of the anteroom instead of inside the negative pressure room for infection control. Only limited devices were prepared in the isolation area; therefore, salvage plans were not immediately ready. Additionally, it is difficult for the leader to identify or communicate key points easily in the isolation area, such as verbalising ‘failed intubation’, which creates a shared mental model. 23 Our results demonstrate the negative impact of infection control measures on communication and teamwork in both objective and subjective evaluations, especially where communication, leadership, and situational awareness were concerned.
The use of telemedicine to facilitate TI has been reported in previous studies. 13 However, only a few studies have been conducted in the clinical environment. Cho et al. 24 reported a randomised controlled study in the ED that demonstrated the feasibility of the Tele-Airway Management System as an alternative to on-scene directed TI. However, this was limited by the small sample size and narrow scope of the data. Moreover, most studies did not demonstrate the disadvantages of separate spaces and the potential benefits of telemedicine on communication and teamwork, which have clinically significant implications for infection control and improving the quality of critical care. As of February 2022, to the best of our knowledge, there has not yet been any primary study that accounts for the investigation of emergent TI in isolation settings and the role of telemedicine to improve communication and teamwork.
During the pandemic, the TAM helped reduce the number of medical staff in highly exposed areas of AGPs from five to two. This may alleviate the workload and stress of healthcare workers and facilitate communication and teamwork during high-risk AGPs. Additionally, the TAM did not increase IA or prolong IT and provided a comparable level of teamwork assessed by the TEAM score. In the TAM, a teleconferencing system was used to improve teamwork and communication for TI, which shared all team members’ real-time images and voices in separate spaces. With the microphone, camera, and speaker, the participants could perform their work without limitations of wires or equipment, and could effectively communicate among spaces. In addition, airway difficulties could not only be communicated via voice messages but also through body language. Thus, all participants not only maintained good leadership and teamwork, but also expressed positive perceptions when applying the model.
This study had some limitations. First, the infection control policies of hospitals dynamically changed during the pandemic. Confounding factors during this period, including policy changes, patient characteristics, medical resources, and laboratory examinations, may have affected the study results. However, the three groups were observed for at least three months and the patient characteristics were relatively comparable. Thus, confounding effects may be minimised. Second, the teleconferencing system was a challenge for the staff during the pandemic. Although the use of telemedicine and related software increased drastically during the pandemic, the staff still needed time to familiarise themselves with the teleconferencing system. Staff confidence in using the new system to communicate and perform teamwork was not evaluated in this study and should be addressed in future studies. Third, for the relatively small sample size, type 2 errors could not be completely excluded from our study.
In summary, the TAM application may ameliorate interference of infection control measures and preserve the efficacy of communication and teamwork during TI. It may be a feasible and beneficial alternative for TI in isolation settings for patients with suspected aerosol-transmitted infectious diseases.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X221124175 - Supplemental material for Using a telemedicine-assisted airway model to improve the communication and teamwork of tracheal intubation during the coronavirus disease 2019 pandemic
Supplemental material, sj-docx-1-jtt-10.1177_1357633X221124175 for Using a telemedicine-assisted airway model to improve the communication and teamwork of tracheal intubation during the coronavirus disease 2019 pandemic by Chien-Hao Lin, Hao-Yang Lin, Shih-Ni Wu, Wen-Pin Tseng, Wei-Ting Chen, Yu-Tzu Tien, Cheng-Yi Wu, Chien-Hua Huang, and Min-Shan Tsai in Journal of Telemedicine and Telecare
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Taiwan University Hospital (grant number NTUH109-P12).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.