
Abstract
Introduction
COVID-19 necessitated a shift from in-person to virtual care for all patients, particularly older adults. It is unknown how older individuals’ views of telehealth changed during this time and how this may affect their future use of telehealth services.
Methods
We used data from a cross-sectional online survey of a nationally representative sample of 2074 U.S. adults ages 50–80 who were participants in the National Poll on Healthy Aging. We performed a descriptive and multivariable analysis of individuals’ perspectives on past and future telehealth visits, sociodemographics, and health status.
Results
Before March 2020, 5.8% of respondents had used telehealth, compared to 32.0% by June 2020. Of telehealth users, 36.1% indicated their most recent telehealth visit used audio-only (i.e., without video) technology. In multivariable analysis, those who never used video technology compared to those who were “very comfortable” (average marginal effect (AME) 49%, 95% CI: 36–63), identified as Hispanic (AME 19% vs White, non-Hispanic, 95% CI: 5–32), or were female (AME 9%, 95% CI: 1–17) were more likely to report audio-only use. Concerns remained about the inability to conduct physical exams (75%) and telehealth quality of care (67%), though most (64%) older adults indicated an interest in future telehealth visits.
Discussion
Telehealth use increased substantially among older U.S. adults during the early months of the COVID-19 pandemic; however, many reported using audio-only telehealth, an important consideration for policymakers and providers. Addressing older adults’ concerns about and barriers to telehealth visits is needed to ensure telehealth does not exacerbate disparities in their care.
Introduction
The SARS-CoV2 (COVID-19) pandemic necessitated major changes in healthcare delivery, most notably in the rapid shift to telehealth from in-person care in order to minimize exposure to infection while offering access to needed health services.1,2 While this transition may have been easy for some patients, there is concern that some groups, particularly older adults, may have had more difficulty. 3
Older adults, particularly those 65 and older, are likely to have been uniquely affected by this change; traditionally, they have lagged in telehealth and internet usage,4,5 yet they are more likely to have multiple chronic conditions necessitating frequent monitoring and care. 6 Older adults are more likely to have disabilities such as vision-, auditory-, and cognitive-related impairment that may make managing telehealth more difficult.3,7–9 Lack of access to or inexperience with internet-connected devices is another commonly reported barrier.3,10 Although telehealth use among Medicare beneficiaries increased from 13,000 to 1.7 million per week in the early months of the pandemic, the percentage of Medicare users with telehealth services has declined from a peak of 47% in the second quarter of 2020 to 15% in the second quarter of 2022.11,12 Additionally, older adults were much more likely to use audio-only rather than video-based telemedicine. 13 Audio-only telemedicine provides more limited communication and patient assessment, potentially impacting care quality and efficacy.
As we reach the end of the COVID-19 public health emergency, it is vital that policy and reimbursement decisions about the future of telehealth ensure equitable access. Although prior research has examined provider perceptions of barriers to telehealth among older adults and there is a preliminary analysis of telehealth use among Medicare fee-for-service beneficiaries during the pandemic, research on older adults’ perspectives on telehealth is also needed to inform patient-centered care.14,15 Furthermore, future reimbursement for audio-only telemedicine is uncertain as pandemic-associated flexibilities wind down. 16 The extent to which older adults may be disproportionately affected by reduced or eliminated payment for audio-only visits is currently unknown. This study examines telehealth experiences, attitudes, and behaviors of a representative sample of U.S. adults aged 50–80 in the early months of the pandemic to inform future policymaking. Our research questions included (1) identifying and understanding potential barriers to and disparities in telehealth use by older adults and (2) examining differences in audio-only and video-based telehealth users.
Methods
This study was conducted as part of the National Poll on Healthy Aging (NPHA), a recurring, nationally representative survey of adults aged 50–80 in the United States. The NPHA is directed by the University of Michigan Institute for Healthcare Policy and Innovation and sponsored by AARP and Michigan Medicine Communications. The survey measures for this study were fielded in June 2020 and focused on older adults’ experiences with telehealth visits. The questions were adapted from similar measures fielded by the NPHA in May 2019. This study was deemed exempt by the University of Michigan Institutional Review Board.
Survey methods
This module of the NPHA was conducted by Ipsos Public Affairs, LLC from June 13–18, 2020, on behalf of the University of Michigan. Ipsos recruits panel participants to the Ipsos KnowledgePanel®, the largest national, probability-based survey panel in the United States, via addressed-based sampling, contacting potential panel members by mail and then by phone for consent and enrollment. 17 To ensure the representation of lower-income households among panel participants, households without Internet access are given a web-enabled device and free Internet service. For this survey, Ipsos randomly selected and stratified 2666 individuals by age group (age 50–80) from its KnowledgePanel® and invited them via email to complete surveys online. Potential participants who had not yet responded received email reminders on days 3, 6, 9, and 12 of the field period.
Measures
Telehealth-specific questions and response options from the survey instrument are publicly available. 18 Respondents were first asked whether their healthcare providers offered telehealth visits, defined as “when patients and healthcare professionals have healthcare visits by video using smartphones or computers.” Those who indicated yes were then asked about telehealth use prior to and after March 2020 for primary care, mental health, subspecialty care, or other care. They were also asked about the modality (phone or video) of their most recent telehealth visit, their reason(s) for having a telehealth visit, the ease or difficulty of completing a telehealth visit, and how they thought a telehealth visit compared to an office visit. Those who indicated they had not had a telehealth visit were asked to choose from a multiple-choice list of reasons why. All respondents were asked about their interest in a future telehealth visit in a variety of scenarios, concerns about telehealth visits, comfort with video chat technology, and use of video chat to stay in touch with friends and family. Additional survey questions asked about respondents’ employment status, insurance coverage, and physical and mental health status. Sociodemographic data were collected by Ipsos.
Analysis
Chi-square tests were used to identify differences in survey responses between groups. We additionally used bivariate and multivariable logistic regression analyses to estimate telehealth use and modality using individual factors such as age, sex, race, insurance coverage, income, health status, and comfort with video chat technology. These results are reported as average marginal effects (AME)—the incremental effect of each covariate on the likelihood of telehealth use and modality. We performed a sensitivity analysis excluding comfort with video chat technology as a covariate to ensure that adjusting for this did not substantially alter the effects of other covariates. We also examined the association between older adults’ concerns about telehealth and interest in future telehealth visits after adjusting for potential confounders. Two-sided P < 0.05 was considered statistically significant. Analyses were conducted with Stata statistical software version 16 (StataCorp). All analyses applied survey weights provided by Ipsos to yield nationally representative estimates. 12
Results
Sample characteristics
The overall survey completion rate among panel members contacted to participate was 78% (n = 2074). Nonresponse rate for each survey item was less than 1%, and more than 99% of respondents missed two or fewer survey items. Weighted respondent demographics and self-reported health status are shown in Table 1. Most respondents (64%) felt comfortable using video chat technology such as FaceTime, Zoom, or Skype; however, 18% were not comfortable, and 17% reported they had never used video chat technology as of June 2020.
Survey respondent demographics and health status

*Totals exceed 100% as respondents could indicate more than one source of insurance coverage.
Telehealth use patterns
Only 6% of respondents reported ever having a video telehealth visit prior to March 2020, increasing to 32% by the time of survey administration in June 2020. This included 24% who used telehealth to see a primary care provider, 12% to see a specialist provider, and 10% to see a mental health provider.
Among those with a telehealth visit after March 2020, 50% reported that an in-person appointment was canceled or rescheduled by their healthcare provider, while 32% indicated it was the only option available when scheduling their appointment. A minority reported fear of COVID-19 (15%), convenience (14%), or other (5%) as reasons for their telehealth visit. See Buis et al., 2020 for additional changes in telehealth visits before and after March 2020. 19
The association between individual covariates and telehealth use is shown in Supplemental Table 1. Respondents who had never used video chat technology were much less likely to have had a telehealth visit (AME: −27%, 95% CI: −33 to −20) compared to those who were very comfortable with the technology. Fair or poor self-reported physical health (AME: 13%, 95% CI: 7–20), Medicare insurance coverage (AME: 10%, 95% CI: 16–19), Black racial identity (AME: 10%, 95% CI: 2–18), and living in a metropolitan area (AME: 9%, 95% CI: 3–14) were associated with a greater likelihood of telehealth use (Figure 1). The model excluding comfort with video chat technology as a covariate was not substantively different (Supplemental Table 1).

Average marginal effect of respondent characteristics on the probability of telehealth use as predicted using multivariable logistic regression.
Differences in telehealth modality
Among the 30% of respondents who reported a telehealth visit between March and June 2020, 64% said their most recent visit used video, while 36% used phone (audio-only). In multivariable analysis (Figure 2), those who had never used video chat technology (AME: 49%, 95% CI: 36–63), were Hispanic as compared to White, non-Hispanic (AME: 18.5%, 95% CI: 5–32), were female (AME: 9%, 95% CI: 1–17), and had at least some college education (AME: 12%, 95% CI: 2–21) were more likely to report audio-only use. Other covariates were nonsignificant. Holding other factors constant, 29% of older adults who were very comfortable with video chat technology were predicted to have an audio-only visit, compared to 78% of those who had never used video chat technology. The odds ratios for univariate and multivariable models with regard to telehealth modality are available in Supplemental Table 2.

Average marginal effect of respondent characteristics on probability of recent audio-only telehealth use as predicted using multivariable logistic regression.
Potential barriers to telehealth visits
The most common reason for not having a telehealth visit was having no recent need for any type of visit, in-person or telehealth (65%). Among those who had a recent non-telehealth visit, the most common reason was a preference for seeing their provider in-person (60%). Fewer indicated it was because their doctor required an in-person visit (19%), they thought telehealth was ineffective (14%), they were not offered telehealth or did not consider it (14%), or they were uncomfortable with or lacked the technology (13%). Only 1% indicated privacy concerns as a barrier, though 24% of all respondents reported having concerns about privacy. Reasons for not having a telehealth visit did not differ significantly by sociodemographic group or health status in bivariate analyses.
Most older adults who had had a telehealth visit (64%) found using the technology to complete a telehealth visit was very easy, while 9% indicated it was somewhat or very difficult. This did not differ significantly by most demographic and socioeconomic measures. However, only 56% of those with a high school education or less reported telehealth was very easy to use, compared with 73% of those with a college degree or higher (P = 0.014). In addition, fewer individuals (59%) who were retired or not working indicated telehealth technology was very easy to use, compared to 73% of currently employed respondents (P = 0.007).
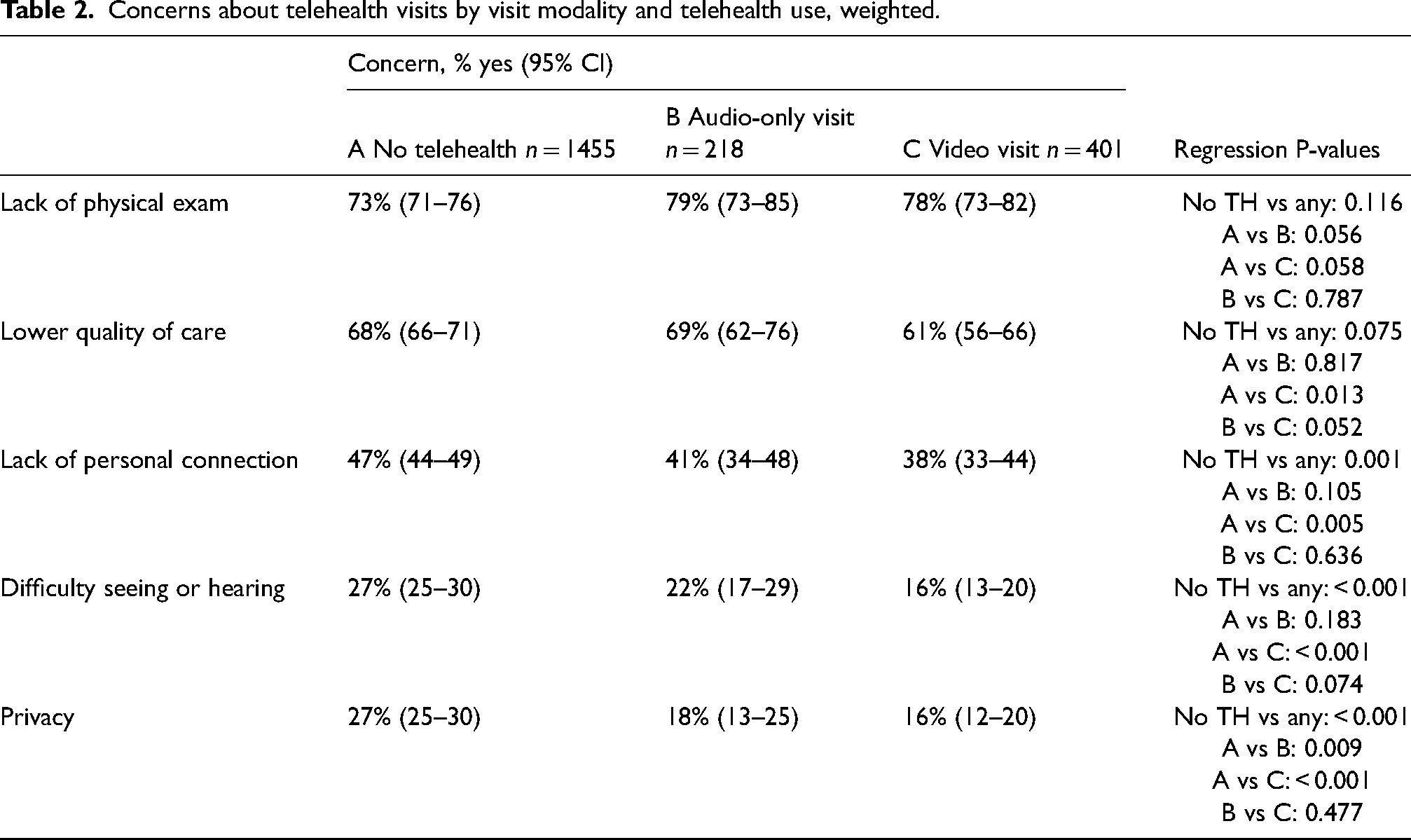
Concerns about telehealth differed somewhat among respondents who most recently had a video visit, audio-only visit, or had never had a telehealth visit (Table 2). Overall, the video visit group had fewer concerns regarding telehealth. A majority of all respondents were concerned about lower quality of care in a telehealth visit, though a smaller proportion of those who had a recent video visit (61%) expressed this concern compared to those with a recent audio-only or no telehealth visit (69% and 68%, respectively, P = 0.028). Older adults who had never had a telehealth visit were more likely to report a concern about lack of personal connection (47% and 39%, respectively, P = 0.001), difficulty seeing or hearing their provider (27% vs 18%, P < 0.001), and privacy (27% vs 17%, P < 0.001) than those who had any type of telehealth visit.
Concerns about telehealth visits by visit modality and telehealth use, weighted.
Interest in future telehealth visits
Respondents who had a prior telehealth visit were more likely to be interested in a future telehealth visit (76% vs 58%), P < 0.001. In multivariable regression, higher education (AME: 4%, 95% CI: 1–6 for each level increase in education), Black race/ethnicity (AME: 8%, 95% CI: 1–16), living in a metropolitan area (AME: 6%, 95% CI: 0–13), and poor mental health (AME: 9%, 95% CI: 1–17) were associated with greater interest in future telehealth (Figure 3). Furthermore, respondents who had never used video technology were predicted to be 36% (95% CI: 29–43) less likely to be interested in a future telehealth visit compared to those who were very comfortable (43% vs 78% interested).

Average marginal effect of respondent characteristics on interest in having a future telehealth visit as predicted using multivariable logistic regression.
In multivariable analysis examining concerns about telehealth and interest in future telehealth visits, concerns about quality of care and not feeling personally connected to the healthcare professional were associated with a lower likelihood of interest in a future telehealth visit (AME [95% CI]: −14%[−18% to −9%] and −16% [−21% to −12%], respectively). Concerns about lack of physical exam, difficulty seeing or hearing the provider, and privacy had minimal effect on interest in future telehealth after adjusting for other factors.
Discussion
The COVID-19 pandemic forced society, including many older adults, to adopt telehealth within a short time frame. This rapid expansion has brought to light both the benefits and continued challenges of providing care via telehealth. 20 As in-person visits resumed, telehealth visits have declined from their peak but continue to play an important role in care delivery. 12 Multiple studies have reported on this rapid adoption and potential age-related disparities in telehealth use as examined through electronic health records or claims data.13,15,21 Our study builds on this existing literature by exploring the individual perspectives of older adults on recent and future telehealth use to shed light on persistent barriers to and future interest in telehealth visits.
Our results show that, within the first few months of the pandemic, the transition to telehealth was primarily driven by changes in the healthcare system rather than by personal fears about COVID-19. Of those who had used telehealth, over one-third reported their most recent visit used audio-only modality. Comfort with video chat technology was strongly associated with both telehealth use and specifically video visits, however more than one in three surveyed were uncomfortable with or had never used it. Although many expressed concerns about the inability to do a physical exam and the quality of care provided, most older adults indicated an interest in future telehealth visits.
Our finding that a majority of respondents were comfortable with video chat technology challenges common misconceptions that older adults, as a whole, are on one side of the “digital divide” between technology users and non-users. 22 However, despite respondents’ prior experience with video chat technology, audio-only telehealth visits were common. This is consistent with other literature on the prevalence of audio-only visits by older adults during the COVID-19 pandemic. Schifeling et al. found that over half of telehealth visits at two geriatric primary care clinics during April and May 2020 were audio-only. 23 Similarly, increases in telephone visits also far outpaced increases in video visits at Veterans’ Affairs hospitals during the COVID-19 pandemic, and those who had video chat visits tended to also have audio-only visits, but few who used audio-only visits also used video chat visits.24,25 Taken together, these findings highlight the degree to which older adults depended on audio-only visits to access care when in-person care was limited. Additionally, even after adjusting for many socioeconomic factors, the fact that comfort with video chat technology was such a strong predictor of telehealth visits—and video visits in particular—suggests that other confounders may exist.
However, continued insurance reimbursement for audio-only visits is uncertain, as much of the expanded coverage was intended to be temporary. Without legislative action, Medicare coverage of most audio-only telehealth visits will end soon after the end of the public health emergency. 26 If providers subsequently limit the use of audio-only visits, our results suggest that the 36% of adults aged 50–80 who are less comfortable with video technology, as well as Hispanic and female older adults, may have more limited options for access to care, which could exacerbate care disparities. Additionally, since participants with worse self-reported physical health were more likely to have used telehealth and similarly likely to have had a recent audio-only visit, limiting access to audio-only visits may further disadvantage this at-risk population.
It should be noted that in introducing the survey, telehealth visits were specified as using video technology. Because we did not include audio-only visits in this definition, our findings likely underestimate telehealth use more broadly, and particularly audio-only care, in older adults. Additional work is needed to fully assess the impact of audio-only care.
Looking beyond prior telehealth experiences, we found that the majority of older adults were interested in future telehealth visits despite indicating concerns about quality of care and lack of personal connection with providers. This correlates with trends in Medicare beneficiary telehealth use, which have plateaued at 15–18% per quarter even as pandemic restrictions on in-person care have lifted, suggesting that many older adults continue to derive value from virtual visits. 12 We anticipate this trend will continue unless restrictions such as the geographic and originating site requirements are re-enforced.
While our study offers a nationally representative view of U.S. older adults’ telehealth use, concerns, and future attitudes during the rapid telehealth expansion caused by the COVID-19 pandemic, it has limitations. Our sample was limited to community-dwelling older adults ages 50–80; thus our results are not generalizable to older adults over age 80 or those living in other settings such as long-term care facilities. Although this was a national sample that used weighting to be nationally representative, our sample was slightly more affluent than the national average, which may have skewed results. As this survey was fielded online, respondents may also have more experience with technology than other adults in this age group. We were also unable to control for personal comfort with and trust in technology, which may have skewed our results, though we did adjust for individuals’ comfort with video chat technology outside of telemedicine. Finally, this study is cross-sectional and was fielded in June 2020, after the first COVID-19 wave in the United States, which may limit generalizability given that metropolitan areas were most affected during the initial wave. Telehealth use peaked in April 2020 and subsequently gradually declined.12,15 Nonetheless, telehealth has remained and is likely to remain an important modality of care delivery for older adults beyond the pandemic.
Telehealth use among older adults increased substantially because of the COVID-19 pandemic. Although permanent policy changes are lagging, telehealth is likely to remain a vital way to access care going forward. Careful consideration of how to continue to integrate telehealth within care delivery is needed to sustain the benefits while addressing ongoing challenges.16,20 We anticipate our findings will provide useful guidance for research and policy moving forward. Our findings demonstrate the prevalence of audio-only visits and suggest there will be a need for ongoing support for audio-only visits. At the same time, given the additional diagnostic value of video-based compared to audio-only telehealth, it will be important to address barriers to video visits. Future work should build on these findings by iteratively assessing telehealth access and barriers to use as policies evolve. Further evidence addressing concerns about telehealth care quality is also needed as telehealth will continue to play a prominent role in the future of ambulatory care for older adults.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X231166031 - Supplemental material for Perceptions of telehealth among older U.S. adults during the COVID-19 pandemic: A national survey
Supplemental material, sj-docx-1-jtt-10.1177_1357633X231166031 for Perceptions of telehealth among older U.S. adults during the COVID-19 pandemic: A national survey by Kathleen Y Li, Liz B Marquis, Preeti N Malani, Erica Solway, Matthias Kirch, Dianne Singer, Jeffrey T Kullgren, Melissa A Plegue and Lorraine R Buis in Journal of Telemedicine and Telecare
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Kullgren has received grant funding from the US National Institutes of Health, US Department of Veterans Affairs, Robert Wood Johnson Foundation, Donaghue Foundation, Healthwell Foundation, and State of Michigan Department of Military and Veterans Affairs; consulting fees from SeeChange Health, HealthMine, Kaiser Permanente Washington Health Research Institute, and Washington State Office of the Attorney General; and honoraria from the Robert Wood Johnson Foundation, AbilTo, Inc., Kansas City Area Life Sciences Institute, American Diabetes Association, Luxembourg National Research Fund, and Donaghue Foundation. All other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The National Poll on Healthy Aging is conducted by the University of Michigan Institute for Healthcare Policy and Innovation and sponsored by AARP and Michigan Medicine, the University of Michigan's academic medical center. Support was also provided by the Department of Veterans' Affairs and the Veterans' Health Administration Health Services Research and Development Service. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government. Dr. Li was supported by NIH/NHLBI T32HL129974.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.