
Abstract
Today, social and healthcare systems at a global level are facing constant challenges dictated by an increasing mismatch between the demand for care services and the supply of human and economic resources. Such a situation has been exacerbated in the past two years by the Covid-19 pandemic. This has led to an increase in the leverage of digitalisation, which has proved to be a crucial tool for the development and application of new organisational models at both hospital and territorial levels, thus addressing the various criticalities already present in the system. In this sense, the Virtual Hospital has emerged as a potential model for increasing effectiveness and efficiency in delivering sociomedical services. Starting from these premises, an EFTE (estimate, feedback, talk, estimate) approach was used to acquire an expert consensus within a multidisciplinary panel of academics and healthcare managers of the Veneto Region in Italy. This article reports the expert opinion on the possible application of the Virtual Hospital model in the national context, starting from the existing international evidence and good practices, highlighting the potential advantages and barriers to its implementation. Furthermore, the article analyses the most relevant areas of investment for the development of intangible assets and the acquisition of tangible assets necessary for its implementation.
Keywords
Introduction
The pressure exerted by global demographic, social and epidemiological changes on national healthcare systems is drastically increasing, putting their sustainability at risk even in the medium term. Seen from the demand side, the causes are to be found, in particular, in the progressive ageing of the population on a global scale, a trend that will lead to an increase in the population over 60 from 1 billion in 2020 to 2.1 billion in 2050 1 as well as in the stable and gradual increase in recent years in the number of people suffering from chronic noncommunicable diseases.2,3 In fact, these latter are responsible for nearly 75% of deaths throughout Europe and 70–80% of world's healthcare resources consumption. In addition, it is the main cause of death in the 54 countries of WHO Europe. 4
The impact of the two aforementioned causes is also reflected in Italy, the country with the second oldest population in the world. In Italy, it is estimated that about 40.9% of the population has a chronic disease, and 20.8% at least two. 5
The changing needs and expressed demand would require new organisational solutions. Still, there appears to be no change or adjustment in the increase in the supply of health services. On the contrary, a significant mismatch between the two is evident throughout Europe. 1 The structural shortage of health professionals, which, according to recent estimates based on pre-pandemic data, is expected to potentially reach 10 million worldwide by 2030 6 as well as the related increase in workload in healthcare facilities, have negatively impacted the staff retention rate and the perceived desirability of health professions. 7 This has initiated a vicious circle that has led to the progressive chronicisation of the shortage of healthcare personnel in both the medical and nursing spheres. In the specific Italian context, the number of doctors per 1000 inhabitants over 75 is lower than the average in Europe. National statistics estimate that more than 17,000 more doctors and 350,000 more nurses should be hired to fill the needs gap. 8 In this regard, as a result of new measures planned in response to the Covid-19 pandemic emergency (2020), the allocation of about 660 million euros, to be distributed among the various Italian regions, has been planned for the recruitment of new healthcare professionals. However, the expected increase remains modest, at around 20,000 in total, distributed as follows: 5000 medical doctors, 10,000 nurses, and 5000 health workers. 9 It will therefore remain up to the implementation of Mission 6 of the National Recovery and Resilience Plan (NRP) to implement a solution to the shortage of personnel, without which the future of the health system and territorial care will be severely penalised. 8
In addition, there is a general increase in the costs of national health services in more developed countries. In fact, between 2013 and 2019, the annual per capita expenditure growth, adjusted for inflation, picked up and reached 3% on average across EU member states. 10 This trend is mainly affected by the price of innovative drugs on the markets and the investment in new technologies. 11
To respond to the critical issues highlighted above, technology and other multiple digital tools – such as smart and wearable medical devices for patients – have been increasingly employed over the last two decades,12,13 which, for instance, makes the remote delivery of various healthcare services possible.14–16 The Covid-19 pandemic has undoubtedly fuelled this trend and led to an acceleration in the adoption of such tools, which also in the Italian National Health Service (NHS) have made it possible to guarantee continuity in outpatient care, limiting waiting and physical contact among people.17–20 The increased confidence in the ability of digital technology to easily deliver services remotely and the acquisition of awareness of the limits of traditional care models 21 have globally stimulated the process of digitisation of health systems, the relevance of which had already been emphasised in 2019 by the World Health Organization within the “Guidelines and Recommendations on Digital Interventions for Health System Strengthening” as well as in the “Thirteenth General Programme of Work 2019–2023.” 22
In fact, the application of innovative technologies in healthcare can provide a real solution to several critical issues of the system, such as increased costs and workload of operators, as well as the shortage of healthcare professionals, while also offering the possibility to efficiently deliver increasingly personalised services 23 and allowing follow-up of patients outside the conventional boundaries of today's care settings, 24 which take the form of so-called ‘waiting medicine’ carried out in family doctors’ or specialists’ surgeries or hospital settings. These advantages, however, are counterbalanced by some non-negligible criticalities emerging from digitisation, which highlight both ethical and legal issues 25 relating to security and full respect for patients’ privacy and data protection, not to mention medico-legal liability profiles concerning the appropriateness of the care provided. 26 These are all issues that would require to be framed within a clear and defined regulatory framework. Moreover, critical organisational issues arise, on the one hand, from the need to redesign care pathways and, on the other hand, to create a single interconnected system. Such a process could, however, be slowed down by the low acceptance of given solutions and by a low – although improved in recent years – digital literacy of the population, as well as by the lack of adequate infrastructures and regulations. 27 Taking these costs and benefits into account, policymakers will have to evaluate solutions that, considering the specificities of the different territories, are able to guarantee the technological-scientific development of the social-health system. Indeed, it is expected that by the year 2040, the radical interoperability of the data produced, technological and scientific developments, and the increase in patient-centredness will represent crucial elements of future healthcare systems. 28
It is with this in mind that, at the international level, over the last decade, professionals have begun to talk about the Virtual Hospital model as a reality capable of providing specialised care at the hospital level within communities to relieve pressure on already overburdened health systems and to achieve equivalent if not better clinical and health outcomes by integrating care models with an initiative medicine approach.
The first references to virtual healthcare models date back to 2006 when Geraint Lewis first described the model of virtual wards or Virtual Hospitals as a model of care that uses some of the systems, personnel and daily routines of hospital wards to provide multidisciplinary care to patients residing within the community. 29 The term virtual, in this case, refers to the lack of a physical building for the care of the patient, who is cared for at home.
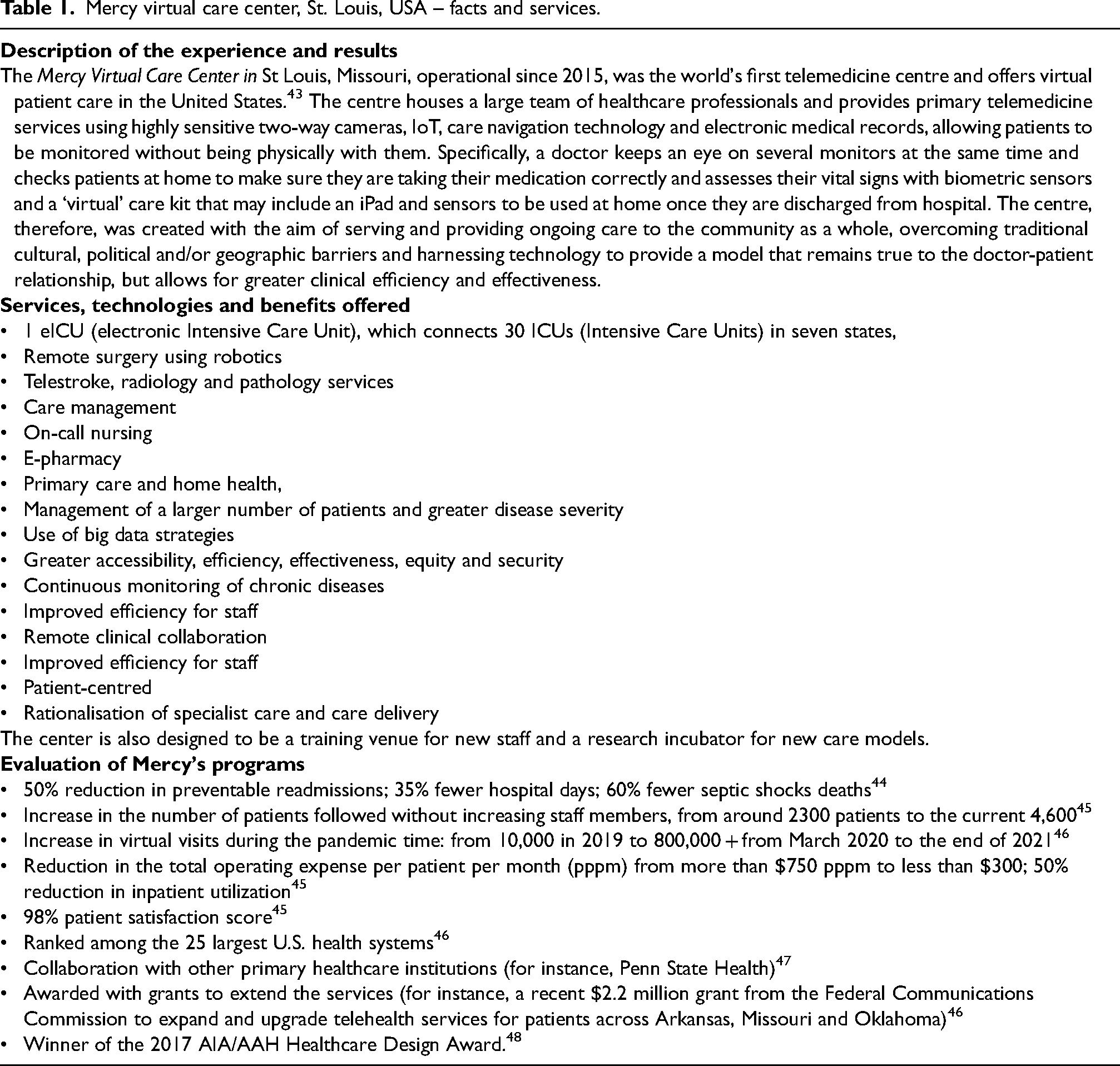
Although this still seems utopian today, it is already a reality in some contexts. The Mercy Hospital in St Louis (USA) represents an example 30 as the world's first telemedicine centre and “hospital with no patients”.31,32 At Mercy, 330 healthcare professionals (doctors and specialist nurses) provide virtual care services to 600,000 patients in seven states (Arkansas, Kansas, Missouri, North Carolina, Oklahoma, Pennsylvania and South Carolina) through 160 workstations. Also Australia stands as a pioneer in delivering virtual care.33,34 For instance, in responding to the Covid-19 crisis, the Sydney Local Health District employed a virtual health service (rpavirtual), to deliver an innovative model of care in a clinically rigorous and safe manner, 35 improving the system's resilience. The rpavirtual initiative allowed to create a 2000 virtual-bed hospital for Covid-infected patients and integrate it with the established 1000 + patient community nursing service.
In the light of the premises set out above, the need to respond to the challenges of the healthcare system by leveraging the opportunities arising from the use of new technologies inspired our study, conducted through the EFTE (estimate, feedback, talk, estimate) methodology among a panel of experts from the Veneto Region, Italy, in order to acquire an expert consensus in a subject of great potential but still little explored by the academic and managerial side. 36 In our research, we, therefore, questioned the possibility of applying a Virtual Hospital model in the Italian reality, investigating what could be the greatest advantages, what the challenges in its implementation and, finally, what investments are necessary to move towards this future scenario.
Methods
Identification of the specific context and reference literature
The study started with a literature review using the Scopus and Pubmed platforms. 37 The Scopus search yielded thousands of contributions. Specifically, 7132 results were obtained, of which 4923 were attributable to the field ‘Medicine’, 1265 to ‘Computer Science’, and 1075 to ‘Engineering’ . However, it was impossible to proceed with a structured, bibliometric, or systematic review, as papers addressing the topic as a whole were absent. In fact, numerous contributions were classified within multiple and varied topics, including ‘Health professions’, ‘Social Sciences’, ‘Nursing’, ‘Biochemistry’ and ‘Mathematics’. The reading of the 92 abstracts of the papers labelled ‘Business Management and Accounting’ led to the identification of some unique (but often marginal) and varied aspects of the problem, including telemedicine, 38 sustainability aspects, 39 logistics management, 40 and issues related to the Covid-19 pandemic.41,42 However, almost all the abstracts were out of context concerning the main topic under investigation, namely the characteristics of a virtual hospital.
Therefore, an analysis of grey literature was also carried out, including both relevant reporting documents on the subject as well as ministerial acts and significant cases of international trials of particular interest for the present study, such as the Mercy Virtual Care Centre in the United States, the Abu Dhabi Health Services Company (SEHA), and the Fiona Stanley Hospital in Australia.
Given that the Mercy Hospital is the only facility that can be defined as a Virtual Hospital, since it has no beds and patients are not physically hosted inside the centre, we decided to use it as a key case study for starting the expert consensus.
Table 1 below shows the main services, technologies and benefits offered by the Mercy Virtual Care Center, as well as the evaluation of some of their programs.
Mercy virtual care center, St. Louis, USA – facts and services.
Creation of the panel for expert consensus
The expert consensus has been based on the EFTE (estimate, feedback, talk, estimate) approach 36 also known as ‘mini Delphi’, which has already been used in other studies in the healthcare sector.25,49
The Expert consensus is a research method that must be rigorously managed to lead to scientifically valid results. The literature recommends, in particular, the selection of experts characterised by diversity and variety in expertise and independence in considerations and choices. 50 In order to meet these criteria, the experts were selected based on their specific expertise. More specifically, the aim was to gather people with a multidisciplinary background, coming from strategic innovation, public and health policies, social statistics, health and corporate management, medicine and surgery, sociology, psychology, and sustainability. Fourteen experts coming from the Ca’ Foscari University of Venice, the Veneto regional leadership, and two prominent medical scholars from Piedmont (University of Turin) and Lombardy (University of Pavia) were involved in the analysis, to give their opinion about the subject of potential benefits and hurdles in implementing the Virtual Hospital model, in the Italian social health system.
Data collection and analysis
The analysis was conducted in May 2022, following the path described below:
The Ca’Foscari group carried out a preliminary analysis of the topic by analysing the professional and ‘grey’ literature (reports published by consultancy firms, international companies and organisations, websites of leading health and technology institutions, …). In addition, one international case study was considered to define the key points for the subsequent comparison with the multidisciplinary team; Experts were given background information through a presentation to be used in making opinion judgments; Experts gathered face-to-face in an e-conference room. Questions regarding the background information were resolved by an appointed mini-Delphi manager, who also acted as the Principal Investigator of the study. Discussion among the participants was encouraged and facilitated through dedicated translation tools.
51
The results of the dialogue were collected and systematised based on the reflections that emerged and then shared with the entire group; The process ended with a summary report of the results obtained made available to all panel participants.
The process is reported in the following Figure 1.
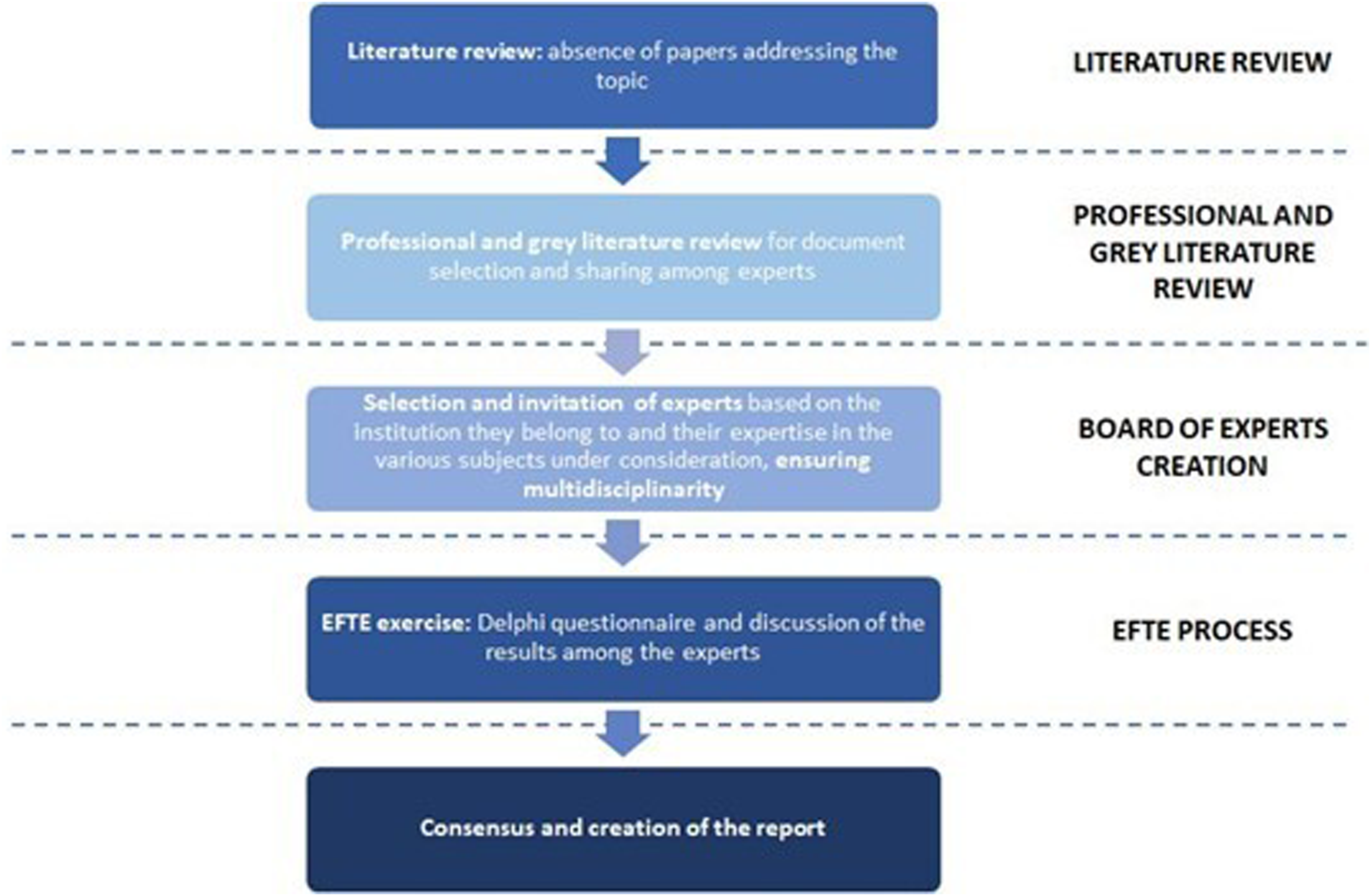
The flow followed (EFTE process).
Results
In the introduction, it was noted that the healthcare sector had already begun to adopt solutions involving the frequent use of telemedicine 52 and remote monitoring systems long before the advent of the Covid-19 pandemic. Undoubtedly, the pandemic has helped speed up this digitisation process, thanks also to new technological tools that enable doctors to treat patients from anywhere, the increased digital skills of the population, and the availability of smart devices and sensors, with this becoming the post-pandemic “new normal.” 13
The Virtual Hospital model has progressively developed within these premises. Although we do not find a unique definition of Virtual Hospital, the literature has provided several inputs,2,28,53–55 as follows:
A centralized facility, also called ‘hub’, in which multidisciplinary teams of physicians and nurses remotely monitor the patients under treatment through the use of high-tech tools, e.g., Internet of Things (IoT) and Artificial Intelligence (AI):
IoT tools are needed to interconnect physical and analogue devices with sensors to collect patient health data and transmit it to a network database, without human intervention. Sensors are embedded within devices such as ‘wearable’ bracelets, wristwatches, and other wearable accessories, which track patients’ movements and activities, automatically activating an alarm if the intervention of medical personnel is required. Online application programmes that can interact with patients and provide them with information and answers about diagnostic and therapeutic procedures carried out in a hospital, or other useful healthcare information. A medical center that has optimised the bi-directional and/or interactive flow of data from the patient to the different wards where he/she will interface with the center's healthcare professionals during the stay; the heavy use of information technologies allows the collection of large amounts of data, reducing hospitalisation length and medical errors, thus improving clinical outcomes.
The existence of very different definitions is probably attributable to the infancy of the Virtual Hospital model. The panel chose, therefore, to use the first definition of the above-mentioned list as the most representative one, based both on what emerged within the discussion and on the contributions of the analysed literature.
Virtual hospital features and target audience
The panel was asked to highlight the differences between the concepts of telemedicine and digitisation on the one hand (vital but not exhaustive aspects of the Virtual Hospital model) and the concept of Virtual Hospital on the other hand.
It emerged from the debate that telemedicine is intended as the provision of healthcare services through the use of innovative technologies, such as Information and Communication Technologies (ICT), in situations where the health professional and the patient (or two professionals) are not in the same location. 56 However, this approach involves a one-off intervention, which is activated following a patient's request.
In contrast, the Virtual Hospital offers continuous assistance to the patient, carried out remotely, similar to that provided in a physical hospital. The center, in fact, does not have any beds. Still, instead, it holds only the healthcare professionals who are able to monitor the patients remotely and offer them virtual care. The success of such an initiative can only be achieved through the development of an adequate degree of interoperability between both different devices used and the information systems. 57
Since these virtual hospital care models aim to provide the same level of care that would be provided in hospitals, they will operate in an interconnected manner while preserving a certain degree of autonomy. In this sense, the discussion group questioned which services should be provided by these facilities and which segment of the population is most interested in the development of such a model.
With reference to the first question, what emerged as pre-eminent services were those aimed at providing patients with continuous, quality care 24 h a day, 7 days a week, while allowing the patient to remain at home or at any other remote destination. This implies the need to provide direct and rehabilitative treatments through integrated multidisciplinary approaches and the development of individualised care plans involving the direct involvement of the patient and the family or caregiver in-home treatment and care. 24 In addition, the collection of data allows the center's physicians not only the preventive identification of patients at high risk of hospitalisation but also to access the patient's history and monitor his or her vital signs. Moreover, it permits access to the patient's medical devices, such as a glucometer, pulse oximeter, and blood pressure measuring instruments, as well as to access laboratory reports and assess readiness for discharge based on predictive risk reduction. 58 Finally, the use of video-conferencing or video consultations, usually delivered by telemonitoring, allows for remote visits and proves to be an effective way to increase access to screening and care, conduct medical consultations and supervise treatment and rehabilitation. 24 This allows, on the one hand, better quality and faster service provision and, on the other hand, a significant reduction in the time taken for visits and, consequently, an equally significant reduction in costs compared to hospital-based visits.
Regarding the second question, the Virtual Hospital model and its services seem to be more efficient if it is aimed at a specific target group of patients, i.e., those who are in follow-up. These include, for example, frail, elderly patients and/or those who have one or more chronic conditions, such as heart disease, stroke, diabetes, some chronic respiratory disorders, etc.
Advantages
The panel questioned the advantages deriving from using a Virtual Hospital model on the main stakeholders, namely patients, operators, health facilities involved, and public bodies / national health systems. Table 2 below illustrates the benefits as defined by the literature and emerged during the multidisciplinary discussion.
Impact and potential value of a Virtual Hospital model on patients, operators, health facilities involved, and public bodies / national health systems.
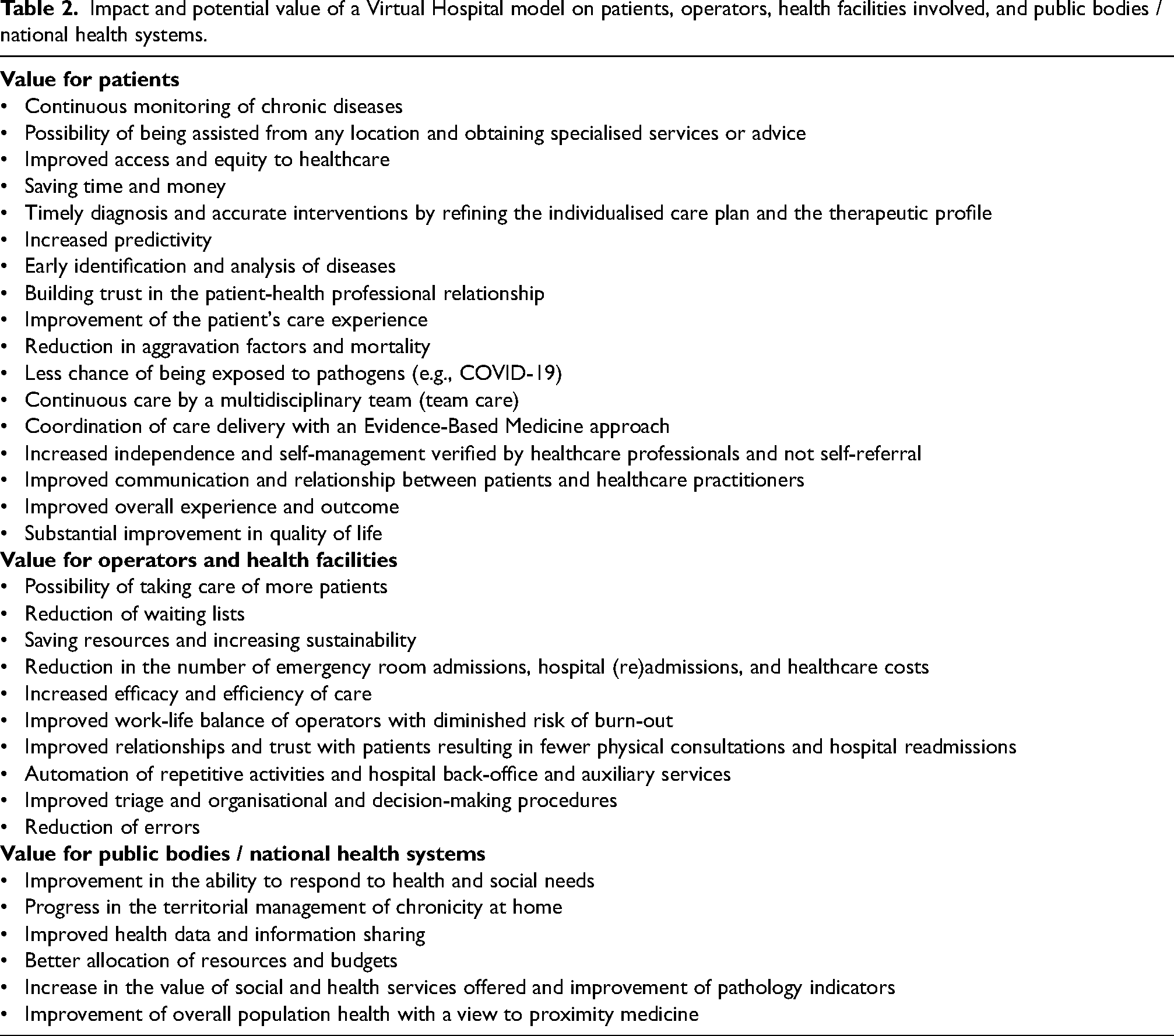
The panel observed that virtual hospitals are able to offer numerous advantages due to their unique and high-tech environment, both for patients and healthcare providers, as well as for the public authority itself. Indeed, they exploit technology to provide a model that remains faithful to the doctor-patient relationship but allows for greater clinical efficiency and effectiveness and provides access to care for all. 28
With reference to the former, i.e., the patients, it is observed that this model can be defined as “patient-centric,” due to the continuous assistance of a team (team care), 59 the coordination of care delivery, and the utilization of the entire set of skills available within the health care system continuum, thus providing more patient-centred care, which is able to acquire greater independence and self-management. 29 Indeed, such a system provides the appropriate tools to help people understand, monitor, and manage their health conditions with greater autonomy, involvement, and responsibility. Furthermore, digital health monitoring enables patient empowerment and stimulates co-production dynamics,60–62 improved communication and relationship between patients and health professionals, more timely diagnoses and accurate interventions, and a better overall experience and outcomes for the patient. 11 The use of big data, in addition, would allow the development of treatments that are, to a greater extent, based on predictive analytics, thus intervening in a preventive and timely manner and developing solutions that are more personalised and participatory but also more efficient and effective. 28 The Virtual Hospital model, therefore, thanks to its high level of digitalisation, permits early identification and analysis of diseases, enabling proactive intervention (defined as initiative medicine) and thus improving understanding of disease progression, resulting in a significant reduction in mortality and a substantial improvement in quality of life. Moreover, in virtual hospitals, the number of patients who can be cared for remotely increases more than in physical hospitals, and this is because patients can be cared for from anywhere (their own home, residences for the elderly, nursing homes or hospices or other care facilities), without the need for outpatient clinics or hospitals.56,63 This frequent mobility, especially for the elderly with chronic illnesses, has undoubtedly been a critical issue that elevated the risk factors of Covid-19 infection and generated outbreaks in care environments and hospitals. Through the Virtual Hospital, one can thus obtain some of the specialized services of hub hospitals without having to physically arrive there, saving time and money and remaining in a more familiar, welcoming and safe environment with less chance of being exposed to pathogens or, on the contrary, spreading them. What is more, this model ensures better accessibility and equity of care and healthcare by providing access to services not otherwise available (thus reducing inequalities in access to healthcare services) and offers greater efficiency, especially with regard to monitoring elderly or chronically ill patients who require follow-up care.34,64 Moreover, teleconsultation allows the involvement of expert or top clinical professionals specialised in some diseases besides those already caring for the patient.
In those contexts where telemedicine and digital monitoring solutions have been implemented, they have been found to establish better relationships and trust with patients while reducing physical consultations and hospital readmissions. 65 Moreover, the use of virtual solutions and robotics can lead to a downsizing of the administrative workload, potentially reducing the risk of burn-out, increasing staff efficiency and reliability and optimising the time of the operators (workflow efficiency) by automating repetitive tasks and hospital back-office and auxiliary service.2,54 In fact, by simply touching a screen, nurses and other medical staff can call up robots for specific tasks, such as the supply of drugs, transporting blood samples, collecting diagnostic results and scheduled delivery of laundry and food, either as a pre-programmed task or as a real-time request. 2 Furthermore, within virtual hospitals, it may be expected an improvement in triage/intake, which can be performed remotely via a video conference with a nurse and/or general practitioner, thus improving access to healthcare and reducing the costs of emergency room visits.2,53
Virtual hospitals allow reducing healthcare costs by decreasing the number of hospital (re)admissions, saving expensive resources such as hospital stays while ensuring the most appropriate care while the patient is at home – see the section Description of the experience and results of Table 1.28,66 In fact, health system managers are often faced with issues related to insufficient budgets, increasing financial pressures and citizens’ expectations. The use of e-health can play an essential role in reducing these pressures by making healthcare institutions more productive and less wasteful through lower service costs, better prevention, de-hospitalisation and optimisation of the hospital network. 66 It should be borne in mind that the organisation of transport, especially for fragile patients involving the use of equipped vehicles and personnel, is one of the most complex and costly elements to manage. 67 At the same time, information technology procedures would allow health authorities to optimise processes by speeding up organisational procedures, increasing efficiency and effectiveness in the management of work phases, distributing responsibilities and reducing errors and deaths, 68 and this is thanks to the continuous and multilevel availability of patient data. Overall, therefore, the Virtual Hospital model is able, on the one hand, to identify and support the well-being needs of the operators, improving the job satisfaction of individual staff members and thus enabling them to have a better work-life balance. 42 Moreover, such a new model is likely able to promote considerable savings in human and financial capital and an increase in sustainability, both from an environmental and economic point of view.
Finally, from the public bodies / national health systems perspective, governments, by using this model of care, can allocate resources more appropriately, increasing the value of social and health services and improving the overall health of the population. 68 It is for this reason that they are increasingly adapting to and facilitating digital transformation in the health sector. Therefore, in order to achieve healthcare systems that are increasingly focused on creating and maximising value (pay for value), governments must play an active role in creating a guiding framework for the healthcare sector to overcome these challenges and support change in the ecosystem, bringing value not only to patients but to society at large. 68
Barriers
The process of implementing the Virtual Hospital model inevitably encounters several barriers, 69 which can be mainly attributed to 4 macro areas, such as: infrastructure and technology, digital skills, organisation and culture, as shown in Table 3 below.
Major barriers to implementing the Virtual Hospital model by macro-area.
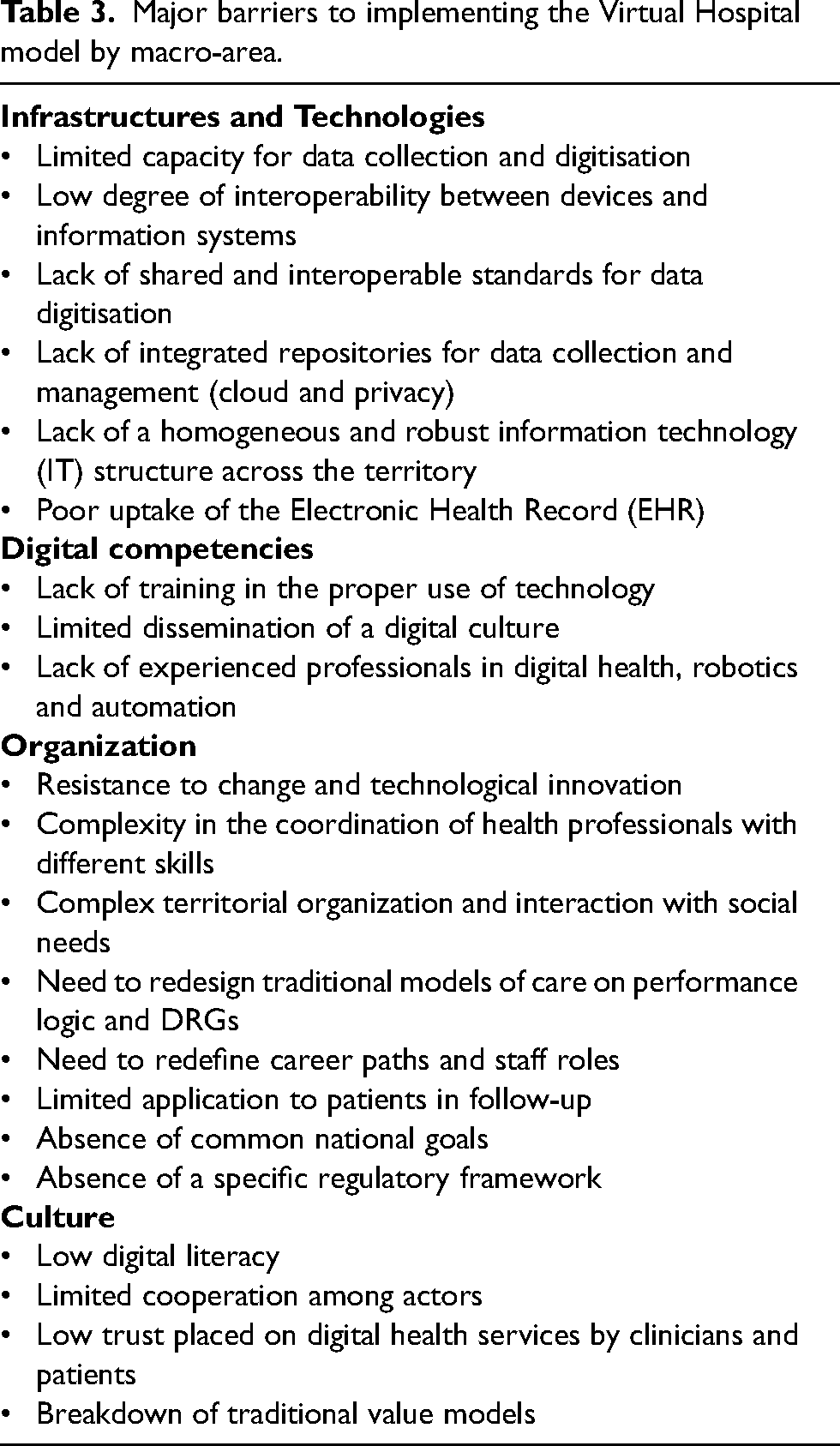
The use of state-of-the-art technology and the uniform and robust presence of IT infrastructure (Wi-Fi, fibre optics, broadband, data center, etc.) throughout the territory, are essential for the proper functioning of the system, which relies mainly on the collection, processing, and exchange of large amounts of data. These need to be collected and digitised, following precise shared and interoperable standards that ensure their quality and interchangeability among different operators, a challenge that can only be addressed through cooperation among multiple actors at local and national levels. 59 The lack of shared standards, on the contrary, hinders the homogeneous distribution of data between different areas, consequently making it impossible to compare medical, health and epidemiological data, as well as preventing the proper functioning of algorithms typical of artificial intelligence. 70
Nowadays, at the national level, it emerges a quantitative and qualitative deficiency of collected and digitised data, as well as low interoperability between existing devices and operating systems, the cause of which is mainly identified in the delay of the sector's digitisation due to the low diffusion of basic tools such as electronic medical records. 71 The management and exchange of data at the digital level may also raise privacy concerns, for which reason it is necessary to develop a specific regulatory framework that allows the clear identification of the data owner and the definition of specific conditions under which a secure and ethical use of the data can be ensured.25,27,72
Investments
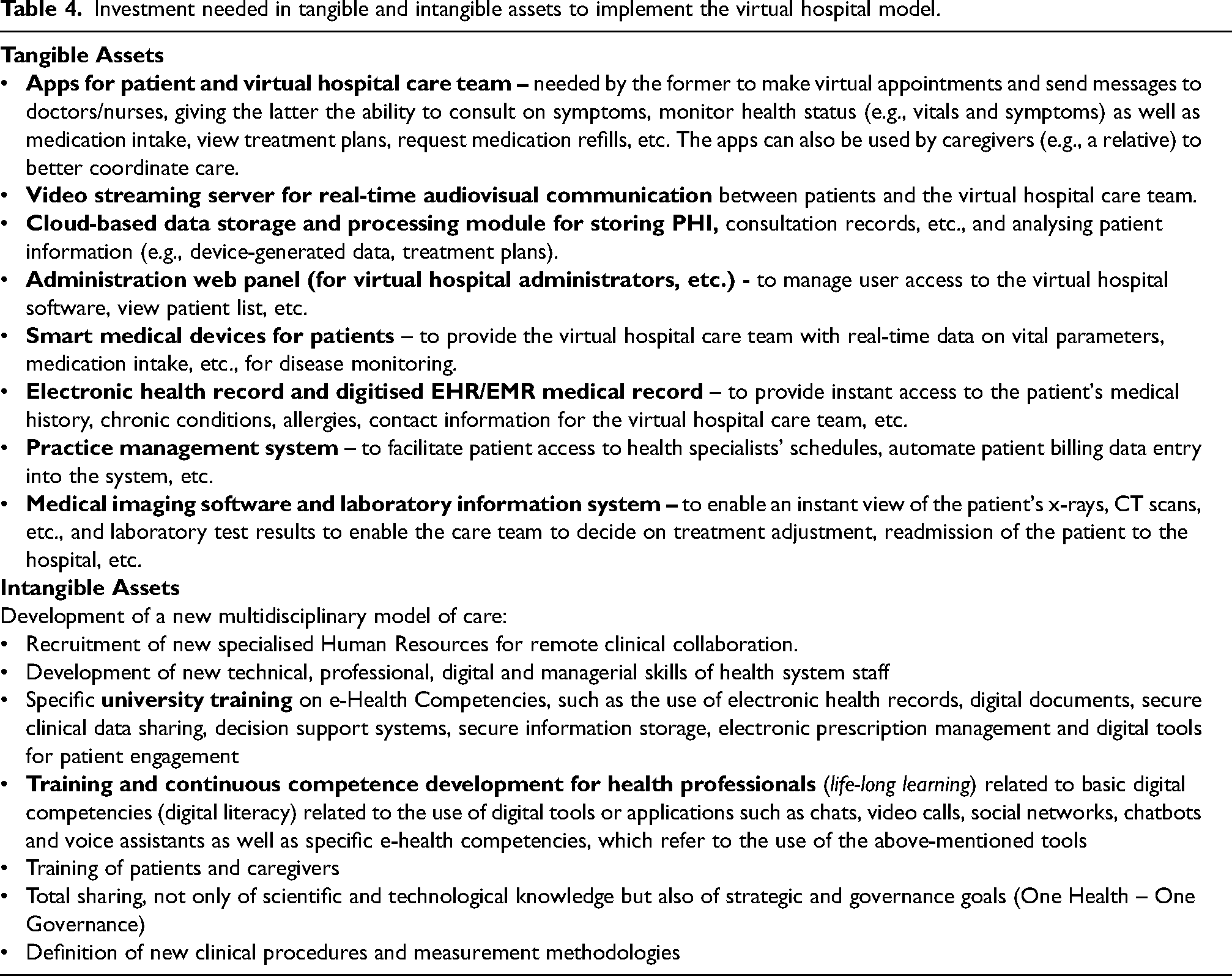
For the implementation of the system, a further aspect is to be considered, namely the needed investments. This latter, on the one hand, shall be directed to the purchase of tangible assets, such as technological tools and cutting-edge information systems, and on the other hand to the development of intangible assets such as digital skills for the use and the fruition of digital services, as shown in Table 4 below.
Investment needed in tangible and intangible assets to implement the virtual hospital model.
Currently, digital literacy is scarcely widespread. Still, it proves to be crucial among clinicians and patients, for the first group to use new tools to deliver care services, and for the second one to take an active part in the healthcare process, given the fact that patients may be located in remote destinations and not in a central facility. 8 This last aspect is crucial because, if poorly implemented, it can limit access to health services to that part of the population that is more fragile. The two categories which are most at risk are the elderly, 67 as they constitute one of the largest groups targeted by the healthcare system, and the low-income citizens who, due to economic and cultural constraints or because of structural reasons, do not have the necessary tools to benefit from the services provided by this model.
Moreover, the implementation of the model, from an operational point of view, requires putting in place several organizational changes, both internally and externally, such as the redesigning of care models, career paths and staff roles to efficiently provide care to patients. 53
Finally, to successfully implement this model is crucial to encourage the adoption, among clinicians and patients, of a totally new digital mindset. A great percentage of CEOs (chief executive officers) and CIOs (chief information officers) of healthcare organizations still consider today virtual-health and telehealth as mere “second class” options to adopt when the traditional model is not available, 53 while many patients do not trust digital health services, which are considered to be of low quality and more prone to medical errors.
Adopting new technological solutions will also lead to creating new relational and value models, where delicate aspects concerning the personal identity and the sense of belonging to a professional community are called into question. 68 One of the risks, for example, is that the introduction of artificial intelligence can be perceived as a de-qualification and delegitimization by healthcare personnel, 25 while old patients, who are not used to technology, may not accept the new digital model of service delivery. 53
Discussion
The discussion among the experts on the panel allowed us to highlight some relevant aspects regarding the potential implementation of the Virtual Hospital model in the international context, thus analyzing the major critical factors.
Among the latter, those that emerged most prominently were those concerning the ageing of the population, the strong and progressive spread of chronic diseases, the underfunding of current healthcare systems, the structural shortage of socio-healthcare personnel, the limited digitalization of infrastructure, and the low rate of digital literacy among both clinical staff and patients.
In particular, adopting the new Virtual Hospital model can help address the above-mentioned issues, allowing the health system to take care of a more significant number of patients and enabling continuous remote care for patients in follow-up, who gain greater independence. In addition, the use of e-health would make it possible to invest economic and human resources more efficiently while contributing to diminishing inequalities in the territory and closing the gap in access to care services. These latter are often linked to economic variables such as the lack of disposable income or geographically determined a significant percentage of the population lives in remote areas in which healthcare services are not accessible.
In the last two years, it has been observed that the Covid-19 pandemic has accelerated the digitisation process and simultaneously increased the confidence rate in these new solutions among clinicians and patients. Furthermore, it has raised awareness about the limitations of traditional care models, demonstrating how remote service delivery can be efficient and reduce exposure to potential pathogens and mortality. Specifically, at both the national and regional levels, Covid-19 has led healthcare providers to consolidate and implement digital projects started in the recent past, as well as to start the first trials of remotely delivered services. Additionally, at the overall level, it emerges how the application of the virtual care model allows, especially at the regional level, a more efficient allocation of human and financial resources, enabling an increase in the value of the offered social and health services and an improvement in the general health of the population.
To reap the benefits of the virtual model implementation, the panel of experts stressed that it is necessary to intervene in different fields quickly: first of all, on the technological-infrastructural gap, investing in the implementation of a digitalized information system, which needs to be adequate for data collection, digitisation, and exchange. Currently, the accumulated delay in the digitization of the health care system and the absence of integrated databases and common standards result in limited availability and usability of clinical data, which prevent the proper use of big data strategies for the development of descriptive, prescriptive, and predictive analyses. 73 In the national context, with specific reference to regional realities, a further challenge is to implement the integration between hospitals and territorial services since the logic of decentralization of social and health services has impacted negatively on the system's communication.
In addition, with reference to intangible assets, it was pointed out that one of the major criticalities is the poor level of digital literacy, which affects not only the population (potential patients), but also the health personnel themselves. While the acquisition of new digital skills may be easy for the younger segment of the population, and for clinicians – for whom competencies may be implemented during undergraduate or postgraduate modules or in their lifelong learning education – in other cases, training and accompaniment in the use of these tools may be necessary, both among patients and caregivers. In some cases, it can also be required the accompaniment of the patient by a third-party figure (for example, for seniors).
To conclude, the experts highlighted the crucial role of different sources of investments currently available to address these challenges, emphasizing, on the one hand, the financial resources made available by the EU4Health program, 74 in particular, in the digital field. Investments, in fact, are needed to induce significant organizational and management changes while allowing for a better allocation of human resources. Overall, substantial medium and long-term investments will be required to develop intangible resources, which will be much more complex than investing in tangible resources, given that they are deeply connected with the sociocultural, human resources, and skills spheres.
Conclusion
Our study has highlighted the multiple aspects of the Virtual Hospital model, from its structural characteristics to its potential benefits, which can be obtained if the different technological, infrastructural, organizational and cultural barriers are overcome. This will lead to relevant changes and trigger solid innovations and a re-evaluation of the traditional healthcare system, which will certainly not be replaced by the virtual healthcare model but strengthened by the new possibility offered by the latter. The traditional healthcare model will constitute the general framework in which the Virtual Hospital reality will be implemented and with which it will inevitably interact for its proper functioning. The increased complexity of the system will have to be wisely managed by policymakers, who shall map and understand the constituent elements of the system by identifying the most critical ones, recognise potential paradoxes and conflicting trends, and rethink strategic choices by weighing the opposing needs and interests of the system's various stakeholders.
To date, however, the data and information to make these assessments are still limited due to the scarcity of studies that have been conducted in recent years, specifically on the Virtual Hospital model as well as the limited literature that can be found on the topic. For this reason, in the coming years, it will be necessary to deepen the knowledge and keep monitoring the context, both nationally and internationally, as well as conducting specific surveys and sharing projects and successful practices. This will allow a better understanding of the costs and benefits of this reality, developing optimal strategies for its implementation and thus ensuring an overall improvement in the health of citizens.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Consent for publication
All the authors declare that they grant their consent for publication
Authors’ contributions
MB, CC, CP conceived the idea of the study; ChBi, VP, FD, CaBa, SC, MZ, GM wrote the research protocol; ChBi, VP, FD, CaBa, SC, MZ, MB, CC, CP, PS, GM, FB, LC, GB were involved in data collection; ChBi, VP were involved in data analysis; ChBi, VP, FD wrote the first draft of the manuscript; CaBa, SC, MZ, MB, CC, CP, PS, GM, FB, LC, GB reviewed the article and made substantial changes. All the authors approved the final version of the article.