
Abstract
This article highlights the benefits of electronic-consultations and outlines steps for a primary care-centered approach to implementation. We include descriptions of traditional and electronic-consultation delivery models from the perspective of referring primary care provider. We describe five best practices for consultations regardless of modality, including clearly defined criteria that are best suited for electronic-consultation. Primary care teams must be equipped to explain the electronic-consultation process to the patient, including when and how results will be communicated. A successful electronic-consultation depends on clear questions and communication, flexibility in available data, a set-up that is easy-to-navigate and the ability to nimbly pivot if an alternative modality is needed. Electronic-consultation implementation may begin small with a single consult service and could include broader healthcare systems considerations including financial implications and service agreements. Based on increasing demand and increasing electronic-consultation familiarity and adoption, electronic-consultation will be a future necessity for primary care.
Keywords
Electronic consultation: A vision for primary care management
As primary care and other services look to the future of healthcare, we need to consider how to meet our increasing healthcare demands with a growing population and ever-increasing limitations. In this article, we explore how electronic consultation or “e-consults” are a potential solution. This asynchronous model may be more cost, resource, and time effective than in-person synchronous care. E-consult allows specialists to reach a more expansive audience through the primary care provider (PCP), and has the potential to lead to increased patient, PCP, and specialist satisfaction. 1 The coronavirus disease 2019 pandemic accelerated telemedicine adoption 2 including the implementation of e-consults during a critical shift to virtual care delivery. 3 Further data on e-consult outcomes is still needed as most studies are small, uncontrolled, and focus on adult patients and a single subspecialty. 4 Despite limitations, patient and clinician enthusiasm is high. 5 In this article, we summarize the benefits of e-consults and suggest primary care-centered methods to expand this consult model.
Standard approach to specialty consults
The typical approach to most outpatient consults includes a PCP visit during which the patient and PCP use shared medical decision-making to decide if a specialist consult is needed. Studies such as labs and imaging are ordered, if necessary, prior to the consult, so that the information is available to the consultant. A consult is then placed with pertinent information for the specialist. Then, the consultant reviews the consult request, and decides if more information is needed prior to scheduling. The patient is typically seen in-person to answer the question and help guide future management. The key part of this process is a question being asked and answered by seeing the patient in clinic.
Adapting to use of electronic specialty consultation
A specialty care request may be entered and answered in many formats other than traditional consultation models. Electronic consultation is an asynchronous model that answers the question through chart review alone, without the patient being seen. Other consult models include clinician-directed ECHO model (where clinicians participate in a virtual community to share support and guidance with peers), asynchronous review of patient or clinic-generated data (tele-retinal image or tele-dermatology pictures) and informal teleconsultation or “curb-siding.” The latter is sometimes through grant-funded community consultation hotline services.
The referring provider and the consultant share responsibilities in the process. 6 Some healthcare systems or sites use service agreements to define the roles of consultant and requesting provider. 7 Periodic review of these agreements is vital as the roles may evolve, necessitating service agreement and workflow amendments. Diagram 1 provides an example of a workflow that details how a consult may be processed from a PCP to a specialist.
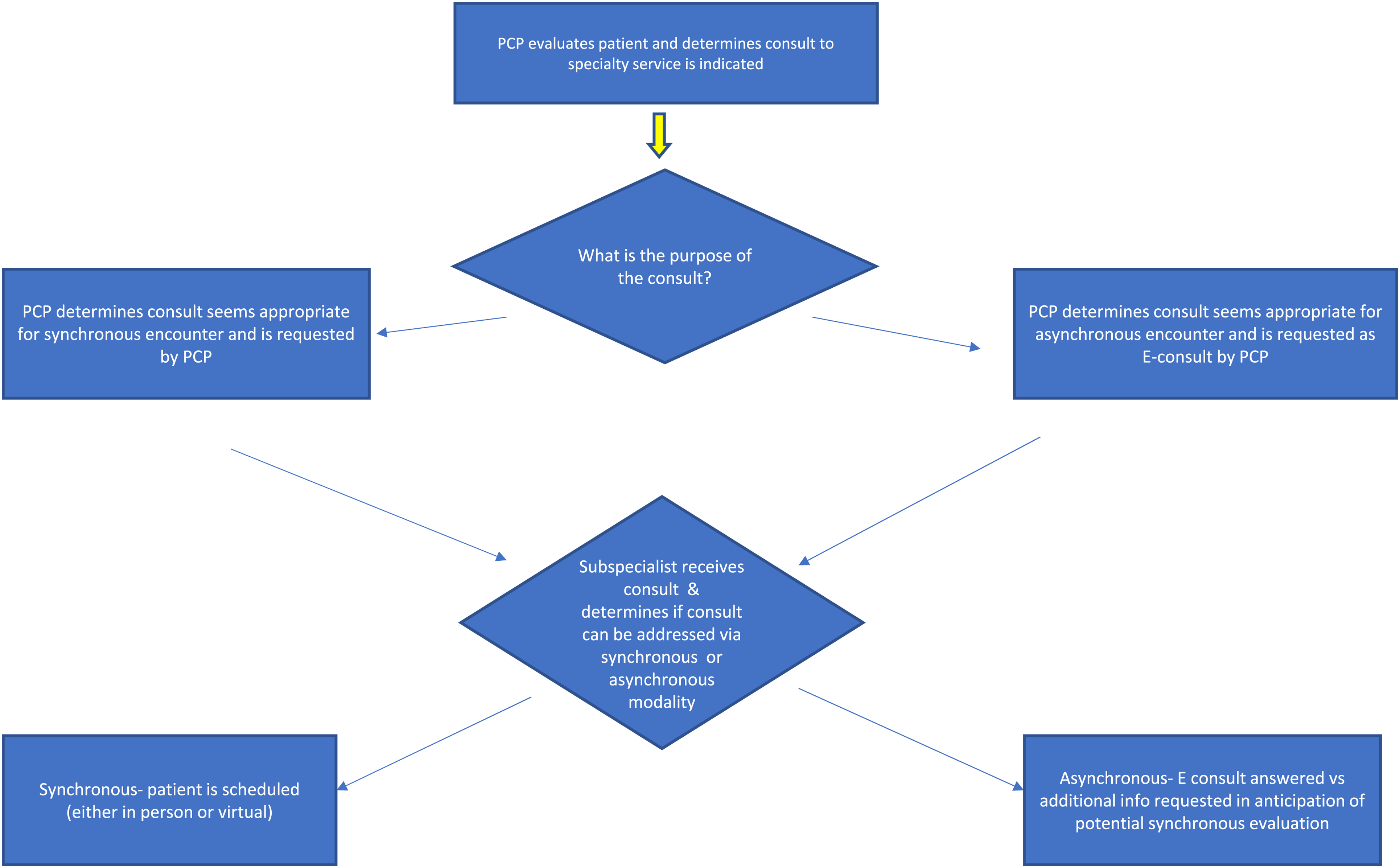
Workflow of how a consult may be processed from a PCP to a specialist.
The switch from face-to-face visits to increased telemedicine evaluation has led to distinct changes in the information available to referring providers (lack of or limited physical exam data or lab data) when placing a consult. The receiving consultant needs to be flexible as some data may be absent.
Benefits of e-consult visits
Despite the challenges telemedicine poses, e-consults and consults facilitated with telephone or video interactions expedite care. Electronic consults increase the availability and flexibility of specialist consults. 8 According to an analysis of electronic consultations at a major academic medical center, a majority (71%) of PCP consults contained diagnosis-related questions with 53% pertaining to diagnostic work-up questions, thereby assisting PCPs to more confidently and expediently diagnose and treat patients. 9 Consultants typically complete an asynchronous e-consult more rapidly than a face to face encounter would occur. This expert chart review can assist the PCP to provide more comprehensive care to patients that live in rural environments or have other barriers to face-to-face visits. Many systems require e-consults to be completed within 48–72 h. 1 A qualitative study of 34 primary care clinicians across 27 Veteran Health Administration sites revealed that e-consults were perceived as valuable although there was an increased work load to shift follow-up responsibility from specialist to PCP. 10 Another qualitative survey among 221 PCPs in a large California health network found overwhelmingly positive perceptions of educational value, with highest value being placed by trainees, nurse practitioners, physician assistants, and less experienced PCPs. 11
A referring PCP may need input from a specialist prior to follow up with a patient and may place an e-consult to expedite care. Specialist e-consults can aid the PCP in preparing a more comprehensive plan which then reduces the need for multiple subsequent appointments to manage patient care. For example, for a patient with suspected auto-immune disease, e-consult may guide additional radiology, lab tests, vaccination, and tuberculosis testing to maximize PCP visit in order to better prepare the patient to be ready for immunosuppressive treatment if applicable. In a retrospective study analyzing 3872 e-consults, PCPs reported more than half of consults were educational with an improved care plan that avoided unnecessary orders and/or visits. 12 E-Consults yield cost-saving potential thus are easier to adopt when consultants are working within the same healthcare system (as each other and as the PCP) and share electronic health record data. 8
The management of e-consults is typically done within a healthcare organization although there are options contracting outside organizations with PCPs. Adopting use of e-consults requires buy-in from organizational leadership. Likewise, the greatest systemic incentives for e-consults exist when clinics and healthcare systems share population-based payment models such as large academic medical centers, clinically integrated networks, government-funded health systems, etc.
Choice of modality of care delivery
Referring clinicians must educate patients about what to expect from an e-consult and have shared medical decision making prior to placing the consult. Clinicians and support staff need to be able to discuss benefits of e-consults including expedited and accessible care and cost-savings (including time, travel, and co-pays). The patient should receive anticipatory guidance regarding when and how the consultant's advice will be communicated. In cases where a scheduled visit or follow-up is deemed necessary by the consultant, it is important to note what modality of care delivery (face-to-face or virtual) is preferred by the patient.
Some evaluations may not be appropriate for e-consultation and may necessitate a face-to-face visit. In an analysis of 200 electronic consults at a major academic medical center, only 14% of electronic consults went on to require an in-person visit. 9 Ideally, the service scheduling the appointment should screen the consults to make sure the modality chosen is appropriate for the clinical question being asked.
Five best practices for consults regardless of care modality
#1 Ask a specific question and provide data
The requesting provider should ask a clear question and provide all necessary supporting data at the time the consult is placed. 13 For example: Placing a consult stating “manage diabetes” provides less context than: “75 y female with diabetes and Hgb A1C of 10 despite two oral agents and insulin titration-what is the next step for management?”. With this example, A1C trend, renal function, medical history, and medication/ allergy lists should be included. Shared data is easiest within use of the same medical record system, although this may not be possible.
#2 Develop consult template requests in concert with clinical stakeholders (PCPs, nursing or support staff service, etc)
Working with stakeholders will ensure that the request collects critical information needed by the specialist while balancing time for completion by the referring provider. Ideally, consult orders or templates within the same system should be standardized and simple to complete. Use of auto-populated fields and quick text when applicable is helpful for the clinicians placing and acting on the consult. Requiring information on the consult that necessitates exiting the consult to review the chart can lead to unnecessary frustration and delays in care. We recommend including the patient's preferred synchronous care modality if e-consult is deemed not appropriate, as well as documenting the patient was informed and agreed to the e-consult process.
#3 Determine when e-consult is appropriate
E-consults are best used when the following criteria are considered: (a) The question posed does not require a physical examination by the specialty service (b) The patient is not critically ill and does not require immediate medical attention (c) The question posed is focused (d) The plan suggested by the consultant does not involve the PCP completing numerous additional steps or ordering tests/studies that they may not be familiar with and (e) All information and data for consultants is available by chart review and is up to date.
#4 Provide a clear assessment and plan in every completed consult
Documentation regarding the plan for treatment and follow up as well as clear direction regarding which team member will be executing the steps is essential. The specialty team should minimize the use of abbreviations or jargon that are not familiar to individuals outside of the specialty. Further, if labs or other diagnostic studies are to be ordered by the referring PCP, directions on how to order additional diagnostic tests should be provided. If the PCP is going to order additional tests, information on when and how to share these back with the consultant is also helpful.
#5 Document the modality used and if the findings were discussed with the patient
For e-consults, it is typically the responsibility of the person who requested the consult to communicate the consultant's recommendations to the patient and to take action. If the provider reading the consult response does not know if the consultant communicated the proposed plan to the patient, it can create confusion and has the potential to delay patient care. It is helpful for the PCP to establish expectations with the patient ahead of time regarding when and how to anticipate learning the recommendations from the consultant.
Future steps in the incorporation of e-consults and telemedicine
We provide below some specific steps when evaluating the use of e-consults and telemedicine.
Consider measuring patient satisfaction, and referring provider and consulting provider satisfaction with the process. Analyze changes in workflow and time. How much time is spent by the primary team to follow up on the recommendations in the e-consult and to notify the patient? Evaluate if recommendations in the e-consult are carried out by the provider placing the consult. If they are not, is the reason documented? Partner with consulting services to develop standardized approaches to consult creation, management, completion and follow up including how to contact the consulting service if patient management questions arise. Determine if there are any patient quality metrics that can be analyzed or trended, which are impacted by the type of consult used.
Health care systems have faced and will continue to face challenges in care delivery, access and patient and provider satisfaction. Innovative strategies like e-consult offer an opportunity to remove barriers to care, improve access and enhance satisfaction. As cost-effective and timely care is prioritized in the coming decades, we anticipate e-consult implementation will not only expand but become a necessity for PCPs and specialty services. We encourage sites to consider developing site-specific e-consult processes, perhaps starting with a single high-yield consult service such as endocrinology, cardiology, clinical pharmacy, gastroenterology, rheumatology, or dermatology. Next, begin implementation of e-consults by considering existing service agreements, system incentives, population-specific needs, and local access to consultants. Finally, work with clinical stake-holders to develop an efficient and clear consult processes as detailed in the five best practices discussed above.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.