
Abstract
Introduction
Electronic consultations (eConsults) have been implemented by numerous academic medical centers (AMCs) to improve communication and address access to specialty care. As these models proliferate, we must understand their comparative benefit and use in various settings.
Methods
This retrospective, descriptive analysis compares eConsult utilization trends at an AMC that has deployed an internal effort and an external pivot. Relevant metrics are presented using counts and proportions or median and range where appropriate.
Results
The internal AMC program demonstrated sustained growth from years 1 through 6, while the external pivot demonstrated considerable growth in year 1, followed by a steady decline in subsequent years. Endocrinology generated the highest number of eConsult orders in both programs (AMC 21%, external pivot 16%). Conversion rates to in-person visits were higher in the external pivot (22%) than in the internal AMC program (14%). Median response time across all specialties was faster (17 hours) for the AMC program than the external pivot (23 hours). The median number of eConsults ordered by any single primary care provider was 3 in both programs. The percentage of providers using the eConsult ordering system only once was approximately 30% in both programs. eConsults were primarily ordered by physicians (68%) at the AMC and physician assistants (40%) in the external pivot.
Discussion
The current study highlights similarities and differences between internal and external eConsult programs that can inform future “right-sizing” of care according to patient needs while promoting local care delivery and improving efficiencies at the AMC.
Introduction
Background
Timely access to specialty care is challenging as availability, scheduling, and other issues hinder access. 1 Over the past decade, electronic consultations (eConsults) have emerged as a viable telehealth model. Defined as “directed communication” between primary care and specialty providers over a secure electronic medium, eConsult facilitates the efficient sharing of patient-specific information between primary care providers (PCPs) and academic medical center (AMC)-based specialists. Recent literature supports the eConsult method as a feasible strategy to improve access to specialty care through enhanced collaboration and simplification of the referral process.2,3 eConsults can also reduce the need for patient travel and wait times for specialist care. 4 Additionally, eConsult supports the “right-sizing” of healthcare at the PCP site and the AMC by assuring those who can and should be managed by their PCP receive care locally. This results in less clogging of the AMC specialist system with individuals who do not need to travel for their care, thereby reserving limited AMC specialist appointments for patients whose conditions require an in-person visit. eConsult can effectively manage specialty conditions, with fewer than 10% of ordered eConsults requiring a face-to-face follow up. 5
The University of Colorado's eConsult programs
In 2018, the University of Colorado School of Medicine (CUSOM) launched its eConsult program modeled after the Association of American Medical Colleges (AAMC) Project CORE (Coordinating Optimal Referrals Experiences). The program aims to lead and support health systems and other organizations to improve care coordination and communication at the primary care–specialty care interface. 6 The CORE model provides a standardized eConsult implementation strategy that has been shown to improve access to specialty care and the quality of care provided while reducing costs and promoting patient-centered care and positive provider experience. 6 The CORE eConsult program at CUSOM was rolled out following the AAMC implementation and training model, which had been piloted at dozens of AMCs before the implementation at CUSOM. AAMC offers an implementation resource guide for participating sites, which includes project timelines and checklists, suggested strategies for provider engagement and reimbursement models, communication plans, quality assurance ideas, and basic best-practice suggestions. 7
Participating sites select specialties for an initial rollout in areas deemed the best fit for eConsults. At CUSOM, specialists in endocrinology and rheumatology were chosen as the first service lines to launch. This staged rollout approach allows a small number of providers to pilot the program and offer detailed feedback on barriers and challenges while confirming that all requirements are being met. This ensures that the institution delivers a good product to providers before scaling up to additional specialties.
The CORE model allows relative value unit-based compensation to the specialist provider (or to be credited to their division) as compensation for replacing face-to-face time spent in the clinic. Additionally, Centers for Medicare & Medicaid Services coding allows for PCP compensation but requires a certain time commitment to be met before the code can be used. Given that this time requirement is rarely met, PCPs have thus far rarely submitted for reimbursement.
The Associate Dean of Clinical Affairs initiated the CORE program at CUSOM as a key clinical initiative, and thus, our efforts were supported by internal funds. CUSOM also leveraged access to Medicaid Upper Payment Limit dollars through the Office of the Dean of the School of Medicine for programs intended to expand access to specialty care for patients covered by Colorado Medicaid.
CUSOM's CORE eConsult system is embedded within the Epic electronic health record (eHR) at 50 + community-based primary care practice sites in Colorado, which supports 1000 + individual PCPs across all 64 Colorado counties to connect with specialists in 28 adult clinical practice areas based at CUSOM. Since implementation, the CUSOM CORE eConsult system has provided over 20,000 asynchronous health information exchanges between PCPs and CU-based specialists to provide right-sized care and avoid redundant or unnecessary care. The system is designed to ensure that if the eConsult response is insufficient for the level of care the patient needs, the visit can be converted to a face-to-face or telehealth visit.
As our internal eConsult program began to establish itself, our state Medicaid recognized the potential utility of eConsult to serve a broader range of patients across the state, especially those in rural areas and those receiving their care through Federally qualified health centers (FQHCs). FQHCs form the backbone of the nation's healthcare safety net, providing affordable care to low-income patients, many of whom lack medical insurance or receive coverage through state Medicaid systems. While FQHCs have been shown to improve access to primary care, their patients often struggle to access specialty care. FQHC patients who need to see a specialist frequently must rely on a patchwork of charity care programs and end up foregoing specialty care altogether, which results in significant long-term health consequences for the patient and cost implications for the overall system of care. This disparity is common across most states 8 and is an ongoing concern. Thus, we believed FQHC patients would likely benefit from eConsult-enabled care. To accomplish this, FQHCs would need an electronic interface that allows our internal health record system to communicate with the many separate and distinct eHRS servicing various practice sites within the state.
In 2019, the State of Colorado supported the development of an eHR-agnostic interface that would allow the program to expand its reach to local FQHCs who do not use Epic. To manage the interoperability challenges of communicating across multiple eHRs, we partnered with a third-party eConsult vendor to expand eConsult services to practice sites using any eHR system throughout Colorado. This “external pivot” platform enables a non-Epic-based interface between FQHC providers and CU specialists. The external pivot program now includes 4 FQHCs supporting 50 + primary care clinics outside of the CUSOM system in Colorado. Transcending multiple eHR systems allows us to bridge the gap and increase the reach of access to specialty care in nonacademic practice settings.
Previous eConsult research from CUSOM has focused on the provider experience and program efficiency standards. 9 The current study investigates eConsult utilization trends, highlighting similarities and differences between the internal CUSOM CORE and external pivot programs. As numerous AMCs are beginning to consider the development of eConsult programs, it is crucial to understand the similarities and differences between the platforms to make informed decisions in order to optimize eConsult implementation and uptake. Limited evidence has been presented to thematically describe eConsult barriers and facilitators 10 and specialist-to-specialist eConsult utilization trends. 11 To our knowledge, this is the first analysis comparing PCP-originated, internal eConsult program utilization trends to those of an external platform.
Methods
This retrospective, descriptive analysis compares utilization data from Project CORE eConsult program at CUSOM to data from the vendor-managed external pivot. eConsult volumes and other order data are described across platforms. Project CORE eConsult orders were extracted from the AMC eHR spanning the entire program length from July 2018 through December 2023. Although our AMC-based specialty care is intended for adults, CUSOM specialists will occasionally receive eConsult orders for patients under the age of 18. With such limited frequency, these were removed prior to analysis. External pivot data was extracted from the vendor database, spanning the program's existence from September 2020 through December 2023. The external pivot does not allow eConsult orders for patients less than 18 years of age to be sent to CUSOM. No other data filters were applied prior to analysis.
Key characteristics are reported using counts and proportions or median and range where appropriate. The compound annual growth rate was calculated as (x(t) / x0) ^ (1/t) −1. Response time was calculated as hours between the date and time an eConsult order was placed by the PCP and the date/time of initial response by the specialty provider. Therefore, response time can only be calculated for completed eConsult orders. eConsults are considered “complete” when the specialist returns an electronic response to the ordering PCP. The term “completed,” therefore, does not imply that the ordering PCP or the patient took any particular action but rather simply that a response was sent from the specialist back to the ordering provider. Specialists can easily convert an eConsult order to an in-person visit when appropriate. Conversion rates are presented as the proportion of eConsult requests completed, converted to an in-person visit, or denied and routed back to the ordering provider because they are inappropriate in some way (logistical, administrative, or not the correct subspecialty). Conversion rates to in-person visits may provide insights into the nature of eConsults, the provider's comfort level, and the complexity of questions from the PCP. 12
All analyses for this study were conducted using r studio version 4.3.1. 13
Results
Volume and provider utilization
Between July 2018 and December 2023, the CORE Program at CUSOM managed 21,931 eConsult requests. Of these, 274 eConsult orders for patients less than 18 years of age were removed, leaving 21,657 eConsult orders for this analysis. Across all years, 76% (n = 16,465) of eConsults were completed, 14.2% (n = 3081) were converted to an in-person visit, and 9.8% (n = 2111) were denied as administrative/logistical or outside-of-provider scope. eConsults ordered through the external platform system totaled 1104 between September 2020 through December 2023. Among these, 73.3% (n = 809) were completed, 21.8% (n = 241) converted, 1.5% (n = 17) denied, and 3.4% (n = 37) resulted in an unknown outcome. See Figure 1 for eConsult conversion rates by calendar year and platform.
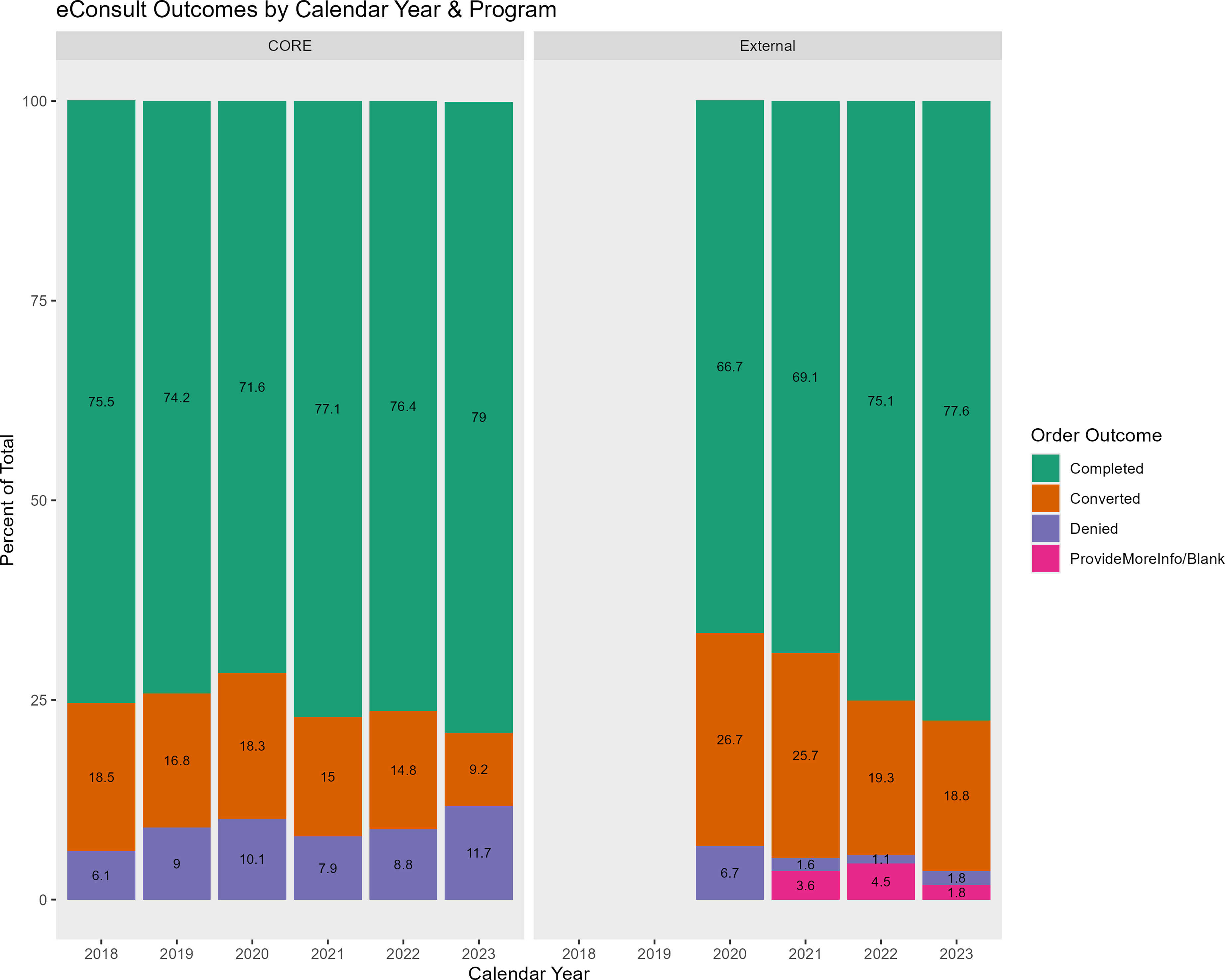
Percent of eConsults completed, converted, and denied by calendar year & program.
Within Project CORE, 1069 unique PCPs requested eConsults. Of the requesting providers, 68% (n = 722) were physicians, 16% (n = 169) were nurse practitioners, and 13% (n = 143) (13%) were physician assistants. Other provider types comprised the remaining 3%. The number of eConsults ordered by any provider ranged from 1 to 355, with a median of 3. Approximately one-third (n = 363) of providers used the eConsult ordering system once. Within the external platform, 164 unique providers ordered eConsults. Provider credentials were missing from 32% (n = 353) of orders. Of the remaining eConsult orders, 39.8% (n = 439) were from physician assistants, 17% (n = 188) from physicians, and 7% (n = 77) from nurse practitioners. Other or unspecified medical providers ordered the remaining 4.2% (n = 47) of eConsults. The number of eConsults ordered by any provider ranged from 1 to 60, with a median of 3. Approximately one-third of requesting providers (n = 53) used the eConsult system a single time.
Within the CORE program, eConsults were ordered by providers from 166 clinics at 49 practice sites in Colorado. eConsults were responded to by specialists from all 28 specialty care areas. External platform eConsults were ordered from 39 clinics at 4 FQHCs and were responded to by specialists across 21 specialty care areas. Endocrinology had the highest proportion of eConsults ordered in both programs (21.6%, n = 4671 CORE and 16.3%, n = 180 external pivot). See Figure 2(a) and (b) for the top 10 specialty volumes by program.

(a) CORE eConsults ordered by specialty with percent of total, top 10. (b) External pivot eConsults ordered by specialty with percent of total, top 10.
Across all specialties in the CORE program, the top eConsult order template used was “Other” (n = 9,498, 43.9%), followed by the template for “Rash/Dermatitis/Eczema/Psoriasis/Skin Discoloration” (n = 1,101, 5.1%). Chief complaint documented in the external platform was most often described as “Other” (n = 543, 49%) followed by joint pain (n = 31, 2.8%). The “Other” order template is available for all specialties. It is intended to provide an option for consulting on patient conditions not otherwise covered by a specific order template.
Within the CORE program, the median response time for completed eConsults across all specialties was 17 hours. The median response time for individual specialties ranged from 2 to 72 hours. Most specialties (n = 24, 86%) had an average response time of less than 48 hours. Data from the external platform demonstrated a median response time across all specialties of 23 hours. Four of the 21 specialties had no completed eConsults and thus, were excluded from response time analysis. Of the remaining 17 specialties, 12 (71%) had a median response time less than or equal to 48 hours. See Figure 3(a) and (b) for a percentage of specialties by median response time category and platform.

(a) CORE eConsult percent of specialties by median response time category. (b) External pivot percent of specialties by median response time category.
Program growth
The CORE program at CUSOM demonstrated a compound annual growth rate of 56% from 2018 through the end of 2023, with sustained increases year over year, except for calendar year 2021. By comparison, the external pivot demonstrated substantial initial growth from 2020 to 2021, followed by a decline in numbers from 2021 through 2023. The compound annual growth rate for the external pivot was 74%. See Figure 4 for a year-over-year comparison of growth by platform.

Total eConsult volumes by calendar year and program labeled with percent change from previous year.
Limitations
Data from the current study reflects utilization trends of an eConsult management system within a single healthcare system in Colorado and may not reflect comparative use at academic medical centers based in other states. As much of the CUSOM care network is housed in urban/suburban areas, these results may not generalize to rural populations. This investigation does not allow us to understand primary care uptake of specialist recommendations or whether there are differences in implementation by provider type or provider distribution in practices. Furthermore, the current study does not allow us to account for differences between the internal and external systems, such as provider turnover rate, training differences, payment policy, etc., which may affect utilization patterns. Thus, we cannot yet understand the reasons for differences between the two systems and how these factors impact eConsult implementation, uptake, and use. In addition, we cannot discuss potential differences in clinical impact between the systems.
Discussion
eConsults are a promising innovation that many AMCs nationwide have increasingly adopted. However, implementing an external pivot remains limited to relatively few. Determining whether important differences exist between internal and external eConsult use cases is imperative for clinical and policy reasons. A more nuanced understanding of external eConsult systems can inform future efforts for successful engagement, implementation, and evaluation of eConsult programs. This analysis represents the first comparison between two eConsult systems implemented by the same healthcare organization. Tangible examples of the operational differences and similarities presented here can be used to align strategic efforts and opportunities for improving statewide access to care.
Implementation of eConsult programs can be complex, costly, and time-consuming. This is especially true for intrasystem development, where there may be a great deal of provider turnover, resulting in challenges with generating “buy-in” from providers. In addition, there may be difficulty in assuring adequate training, streamlining technical support, and consistent quality improvement, problems with workflow, or other complications and barriers that may exist when two or more systems attempt to collaborate on something as complicated as change in healthcare delivery. While it is difficult to ascertain the exact cost of such an initiative, this is a subject of interest for numerous AMCs using the CORE model and we recommend this for future investigation.
The AMC-based CORE program has continued to demonstrate growth. This may indicate increased support from an AMC that has previously struggled with a specialist burden as eConsults augment the workload of managing patients who may not need AMC-based, face-to-face care. The external platform experienced declining volumes, perhaps related to concerns about the sustainability of a new model of care. These efforts exist in an atmosphere of uncertainty about reimbursement, lack of sufficient and/or ongoing training, program and FQHC turnover, and worries about increased workload, all of which can adversely affect eConsult adoption and continued use.
Previous literature reports substantial differences in eConsult subspecialty volumes, outcomes, and primary care clinician types. 14 Our data suggests that endocrinology is consistently the most frequently ordered subspecialty in both the internal CORE system and the external pivot. This is consistent with earlier findings 15 and may suggest that some common endocrine conditions are particularly well-suited for management via eConsult.
The median number of eConsults ordered by unique providers is similar across platforms, which may suggest that PCPs are open to trialing the novel eConsult technology for diverse patients independent of eConsult model. However, the percentage of ordering providers who used the eConsult system only once was high (∼1 in 3 providers) both internally and externally, which may indicate barriers to use or that providers need more consistent promotion of eConsult methodology to integrate the ordering process into their existing workflows truly. The seamless integration of eConsults into workflow and day-to-day operations remains essential and challenging. To foster routine adoption, we suggest supporting local eConsult “champions” within targeted primary care clinics to provide support and help troubleshoot issues for providers. This is an area for further investigation.
While the rate of eConsults converted or denied differed between platforms, the completion rates internally and externally were comparable and similar to those found in other specialty care eConsult studies.16,17 To maintain high completion rates, eConsult programs must provide ongoing training and support for providers on the best strategies to optimize their use. The qualitative factors facilitating or hindering eConsult use remain an area for further investigation.
Future research should focus on in-depth data analysis and qualitative data on contextual factors, provider preferences, response to challenges, and motivators for usage. Understanding the operational integration of eConsult systems into health systems and practices is essential for improving programs and designing effective policies. As states and payers promote eConsults to enhance access to care, it is crucial to focus on implementing them in safety net practices and among vulnerable patient populations, such as those receiving care at FQHCs, to maximize their benefits and align with broader healthcare accessibility objectives as the landscape evolves.
We must take on the challenge of identifying eConsult outcomes and benefits to providers, patients, organizations, and policymakers. We have previously identified the time, cost, and environmental savings attributable to eConsults. 18 Indeed, using eConsults holds promise for delivering more patient-centered care, reducing unnecessary and redundant care, and reducing patient costs by minimizing travel and time off work. The next steps for both programs must focus on evaluating the effort's practice, patient, and financial impacts. While our results are not definitive, this article illustrates the potential and viability of eConsult programs. It provides a better understanding of two types of frequently used models in many academic medical centers across the United States.
Conclusion
Healthcare systems and payors are adopting eConsults as a healthcare delivery model, and the volume of usage continues to increase. Such efforts are consistent with the national direction of primary care being the locus of patient care management. It is vital to understand utilization trends and differences between various models of eConsult care delivery. This is the first evaluation of the implementation of two unique eConsult platforms. As additional AMCs have initiated external platforms, further investigation across these other systems is warranted to identify best practices and compare and contrast use patterns and implementation differences across systems and/or states, given different dynamics. eConsult benefits patients, providers, health systems, and payers by allowing primary care providers to provide comprehensive care locally. The results of this study are a preliminary step in determining whether eConsults can be deployed by AMCs in every state trying to build better partnerships with PCPs across the state, especially those not affiliated with an AMC, like FQHCs, leading to the overall improvement in an overarching goal of enhancing access to specialty care, improving quality, reducing costs, and promoting patient-centered care and positive provider experience.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The datasets analyzed during the current study are not publicly available due to privacy restrictions but may be available from the corresponding author on reasonable request.