
Abstract
Introduction
Telehealth use expanded rapidly in oncology during the COVID-19 pandemic, but determinants for ongoing use in metropolitan cancer care after the pandemic remain unclear.
Methods
A multi-centre retrospective cohort study of 271,889 oncology outpatient consultations (face-to-face, telephone, video) from 1 January 2019 to 30 June 2024 across four cancer centres in Sydney, Australia was conducted. Consultations were divided into pre-COVID, during-COVID restrictions and post-COVID restriction time periods. Multivariable generalised estimating equations modelled the odds of telehealth use in the during and post-restriction periods, testing interactions between time periods and key covariates.
Results
Across 271,889 consultations with 21,125 patients the proportion of telehealth consultations was negligible pre-pandemic (0.4%), peaked during restrictions (24.7%) then reduced but was sustained post-restrictions (11.4%). Post-restrictions, telehealth use was more likely for follow-up consultations (vs new, p < .001), medical oncology consultations (vs radiation, p < .001), patients enrolled on a clinical trial (p < .001) and primary tumours including brain and genitourinary (vs breast, p < .001). Patients from the most socioeconomically disadvantaged quintiles (vs highest, p < .001), those who required an interpreter (p < .001), those receiving active treatment in the cancer centre (vs not on treatment, p < .001) and with primary tumours including head and neck or skin (vs breast, p < .001) were less likely to undergo telehealth consultations.
Conclusions
There is modest but sustained use of telehealth in oncology post-pandemic restrictions particularly for follow-up consultations, with less utilisation in populations experiencing disadvantage. Strategic, equity-focused policies are needed to ensure that telehealth use enhances, rather than exacerbates, disparities in access to cancer care.
This is a visual representation of the abstract.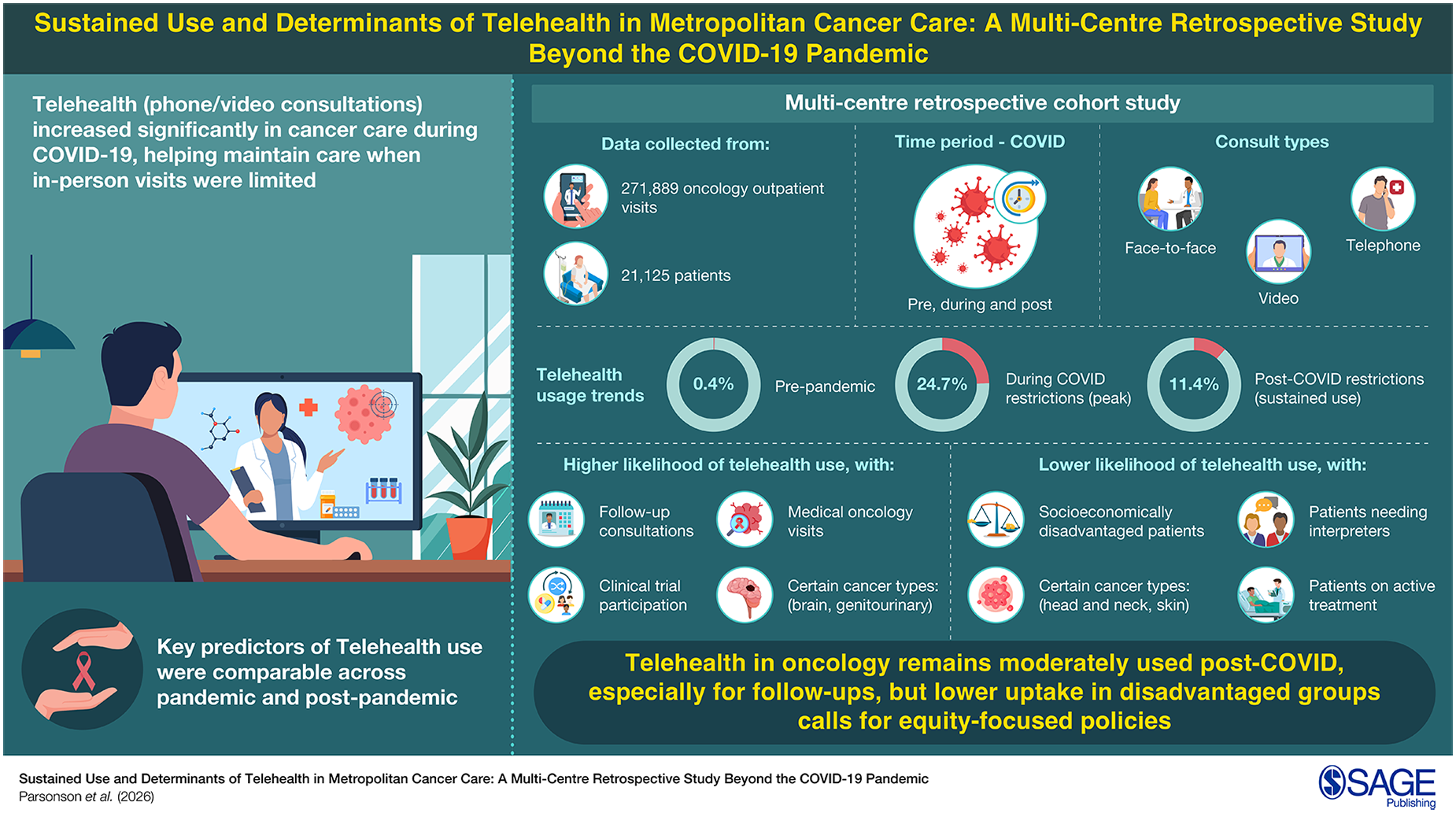
Introduction
Telehealth is defined as the delivery and facilitation of health and health-related services including medical care, provider and patient education and self-care via telecommunications and digital communication technologies. 1 Uptake of telehealth has historically been in rural populations to facilitate access to specialists, reduce time and travel expenses for patients and allow access to multiple remote sites in one session.2–4 The use of telehealth and remote supervision models, such as telechemotherapy in oncology has traditionally increased capacity at rural sites to safely manage complex treatments, that could not otherwise be provided.5–9
The recent COVID-19 pandemic presented new challenges in the management of people with cancer who are often immunosuppressed and are at a higher risk of developing complications including pneumonia, respiratory failure and even death. 10 To reduce the risk of exposure to the coronavirus to both patients and doctors, there was a rapid shift away from traditional face-to-face appointments and uptake of telehealth in cancer care delivery in both metropolitan and rural settings. 11 This approach was widely adopted by physicians and cancer societies worldwide that released guidelines supporting bolstering telemedicine services and reducing in-person clinic visits. 12
The COVID-19 pandemic has provided the opportunity to consider ongoing adaptations and changes which can be incorporated into future models of cancer care. After the extemporaneous, large-scale and time-pressured implementation of telehealth in cancer care, there is now a call to continue its use in appropriate clinical settings beyond the COVID-19 pandemic restrictions. 13
However, despite the advantages of telehealth to reduce travel burden and enhance access to care, the impact of the COVID-19 pandemic has also led to the uncovering of inequities in its use, with reduced uptake in patients from lower socio-economic backgrounds, in those with limited digital literacy or those who require the use of an interpreter. 14 Telehealth may also not be appropriate for all consultations such as initial consultations or when physical examination is required for diagnosis or follow-up. 15
The purpose of this study was to quantify the proportion of in-person and telehealth consultations for oncology outpatient attendances across four cancer centres before, during and after the COVID-19 pandemic restrictions and further explore sociodemographic, cancer and treatment factors associated with use of telehealth beyond the COVID-19 pandemic.
Methods
Participants included in the study were 18 years or older at the time of their consultation, had a histologically or cytologically confirmed malignancy, and had at least one consultation (telephone, video or face-to-face) with a radiation oncologist at a cancer centre in South Western Sydney Local Health District (SWSLHD): Liverpool Hospital, Bankstown-Lidcombe Hospital, Campbelltown Hospital or Bowral District Hospital. Patients who had additional consultations with other cancer care specialists (i.e. medical oncologists or haematologists) were also captured. SWSLHD spans an area of 6243 square kilometres and is a rapidly growing area in Sydney, Australia, with an estimated population of 1,038,534 in 2021 projected to increase to 1,317,503 by 2031. 16
De-identified patient data was extracted from the SWSLHD Radiation Oncology Virtual Clinical Quality Data Registry through the MOSAIQ electronic medical record. Information extracted included modality of outpatient appointment (face-to-face, telephone or video consultation), patient age, country of birth (including if the country is an English language-proficient country), gender, age, nature of appointment (initial or follow-up consultation), specialty service (radiation oncology, medical oncology, haematology), use of an interpreter, primary tumour group, tumour stage (In-situ, Stage I–III, Stage IV/metastatic), and whether the patient was on active treatment.
For time periods of the appointments, these were divided into the pre-COVID-19 restriction period (1st of January 2019 until 30th of January 2020), the COVID-19 restriction period (1st of February 2020 until the 30th of November 2021) and the post-COVID-19 restriction period (1st of December 2021 to 30th of June 2024) to reflect the different time periods when restrictions were in place in health care settings in Sydney, Australia. 17
Place of residence was classified using the remoteness structure of the Australian Statistical Geography Standard, which is derived from the Accessibility/Remoteness Index of Australia (ARIA+). 18 Area level socio-economic status (SES) was using the Index of Relative Socio-economic Advantage and Disadvantage, Distribution of Statistical Area Level 1 Deciles, 2021, 19 that were then summarised into quintiles. Country of birth was divided into a dichotomous group of those born in core Englsh-speaking Anglosphere countries (Australia, New Zealand, Canada, the United Kingdom or the United States) and those born in other countries. 20
For primary tumour type, these were classified into regions of primary tumours that reflected medical practitioner sub-specialities at each site. This included: central nervous system, head and neck, breast, lung, upper gastrointestinal, lower gastrointestinal, prostate, other genitourinary, gynaecological, haematological, skin, unknown primary, and other.
To estimate the proportion of patients who were on active treatment requiring attendance at the cancer centre, any patient who had a clinic appointment within six months of a treatment appointment were classified as being on active treatment. Patients were identified as clinical trial patients if they were flagged on the EMR as enrolled on a clinical trial at the time of their consultation.
The association between characteristics of the post-COVID population and the use of telehealth was analysed using multivariable generalised estimating equation models. Cluster was defined by patient as patients had multiple appointments during the study period. A logit link with binary distribution was specified. The outcome was use of telehealth (yes/no) for an appointment and predictor variables were consultation type, gender, ARIA+, SES, martial status, need for an interpreter, country of birth, enrolled in clinical trial or not, tumour group, stage group, treatment within six months and type of specialist consulted, and time period (during/post-COVID). Interaction terms between time period, and all other predictor variables were considered to determine whether the effect of these variables varied between time periods. Interaction terms with p < .05 were included in the final model. This population were not restricted by pandemic-era restrictions, and patients and clinicians often had the option to choose to have a telehealth consultation. This population was thought to be most representative of assessing potential future populations that may continue to use telehealth even when social distancing mandates do not exist but telehealth consultations are still reimbursed.
The Radiation Oncology Virtual Clinical Quality Data Registry platform has approval from the SWSLHD research ethics board (Approval No. HREC/16/LPOOL/603). Patient consent was waived as the project was approved under the low and negligible risk pathway.
Results
Patient and appointment characteristics
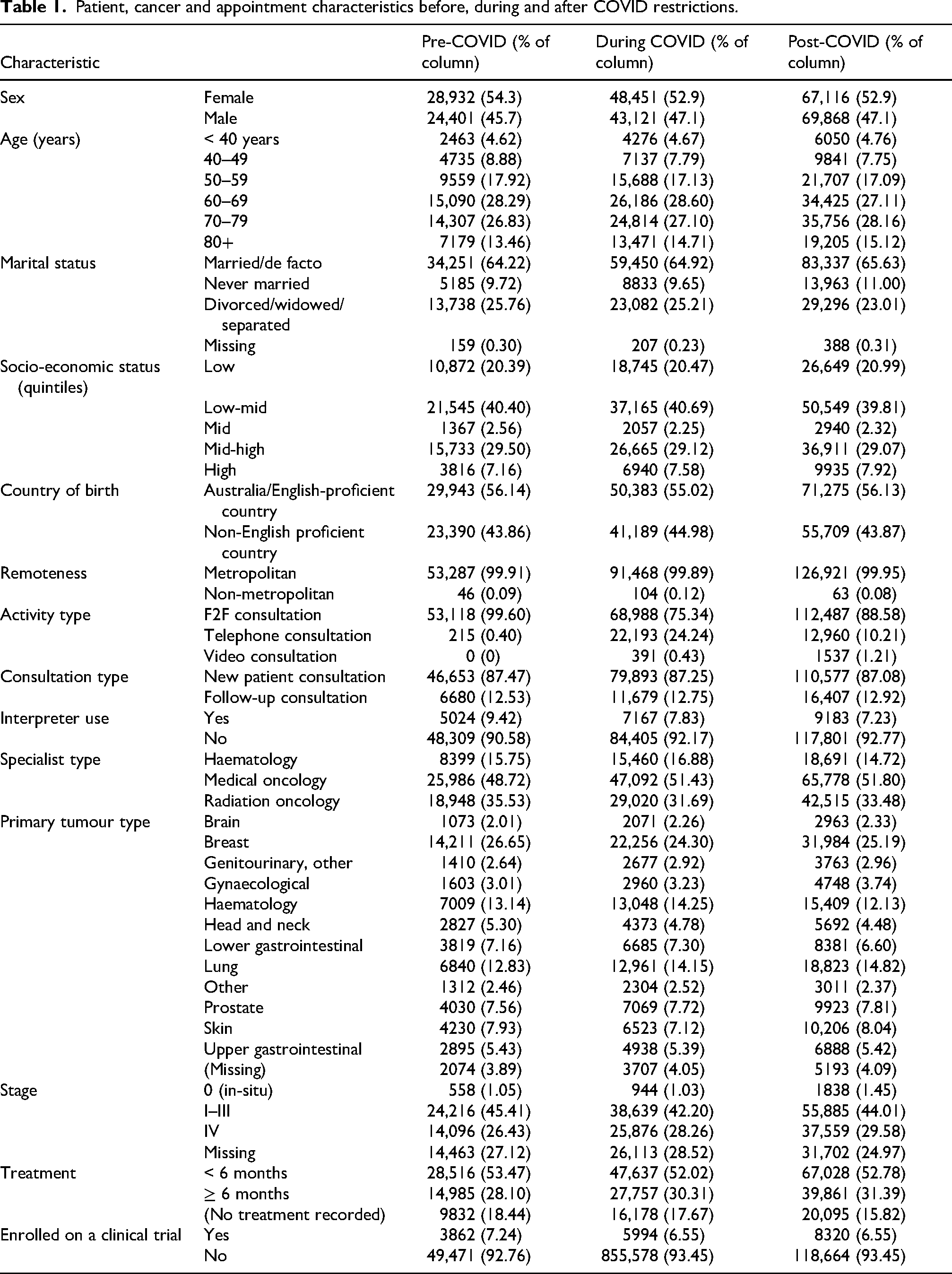
From the 1st of January 2019 to the 30th of June 2024 complete data was available for 271,889 consultations conducted with 21,125 individual patients (Table 1). The majority of consultations were follow-up consultations (87.2%, n = 238,146) with patients who were known to the oncologist and cancer service. A large proportion of patient consultations (60.6%, n = 165,525) were with patients who resided in a postcode in the bottom two quintiles of SES per the SEIFA classification. A minority of consultations (7.86% of consultations, n = 21,374) required an interpreter.
Patient, cancer and appointment characteristics before, during and after COVID restrictions.
Cancer and treatment characteristics
Of all consultations, the most common tumour type was breast cancer (25.18%, n = 68,451). About half of all consultations (52.6%, n = 143,181) were with patients on active treatment at the cancer centre (i.e. received systemic anti-neoplastic therapy or radiotherapy within 6 months of their appointment).
Summary of telehealth utilisation
The overall telehealth utilisation rate during the entire study period was 13.7%. Telehealth usage was minimal prior to the pandemic (0.4% of consultations), peaked during the COVID-19 restriction period (24.7% of consultations) and fell to 11.42% in the post-COVID-19 restriction period (Figure 1).
Comparison of during-pandemic and post-pandemic subgroups
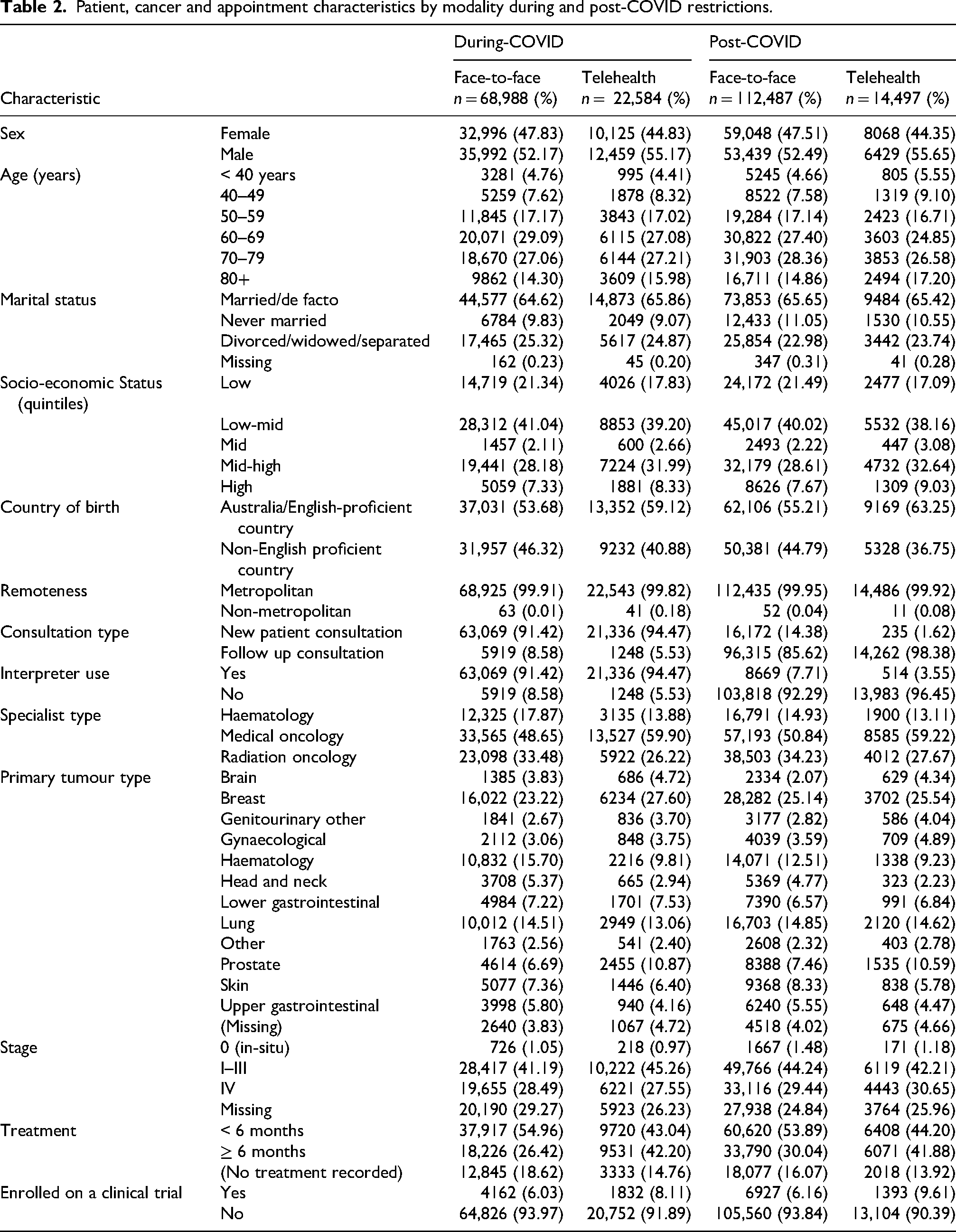
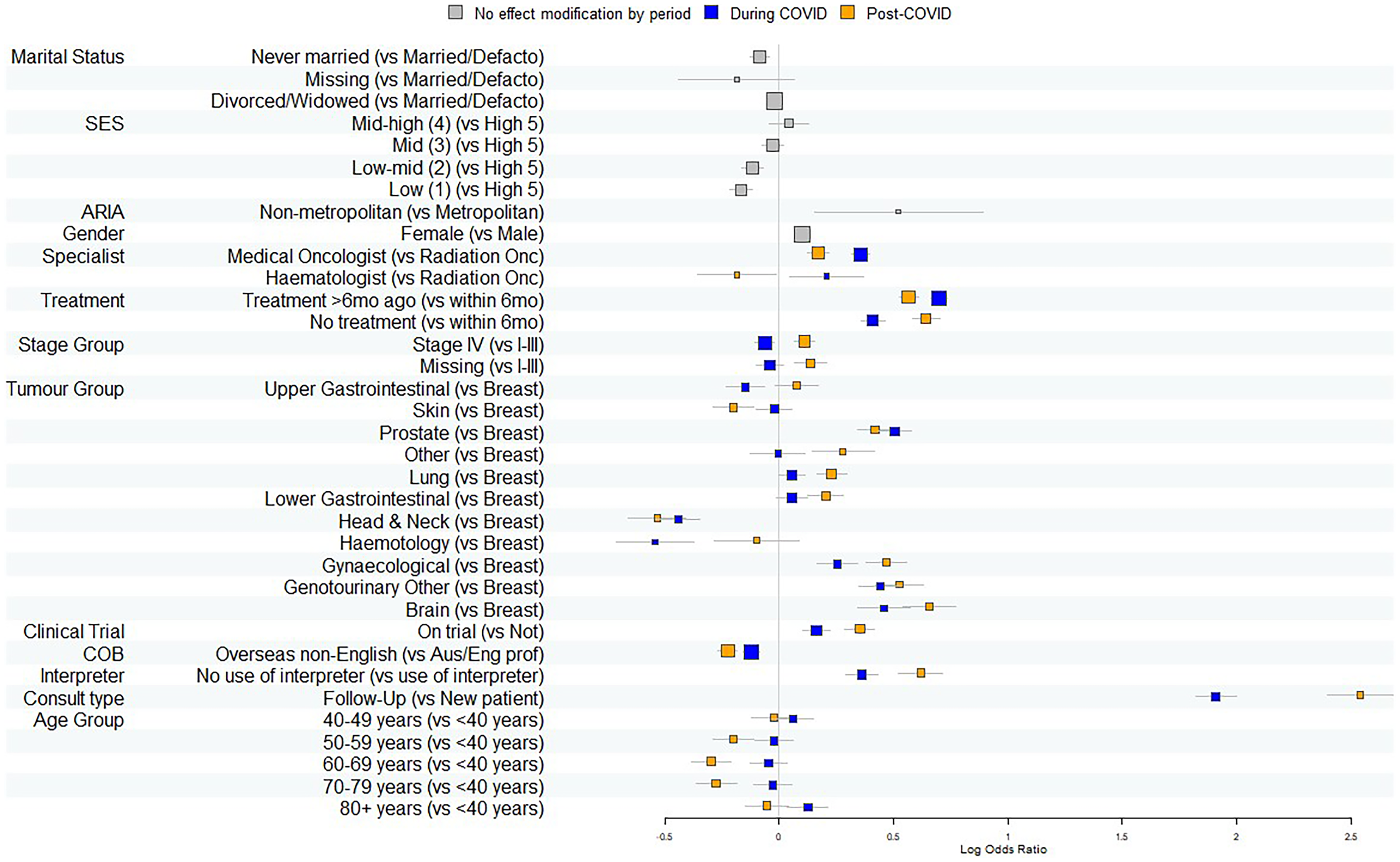
The breakdown of face-to-face consultations and telehealth consultations in the during- and post-pandemic subgroup was summarised separately (Table 2). Multivariable generalised estimated equations were applied to this subgroup to evaluate the likelihood of telehealth consultations both during and after the COVID-19 pandemic restrictions (Figure 2).
Patient, cancer and appointment characteristics by modality during and post-COVID restrictions.
For the post-COVID-19 period, on multivariable analysis, females were more likely to utilise telehealth (OR 1.10, 95% CI [1.07–1.14], p < .0001). Compared with those in the highest socio-economic quintile, those in the lowest (OR 0.85, 95% CI [0.80–0.89], p < .0001) and second lowest quintiles (OR 0.89, [0.85–0.93], p < .0001) were less likely to use telehealth (Table 3).
Multivariable generalised estimating equation model for use of telehealth during and post-COVID restrictions.
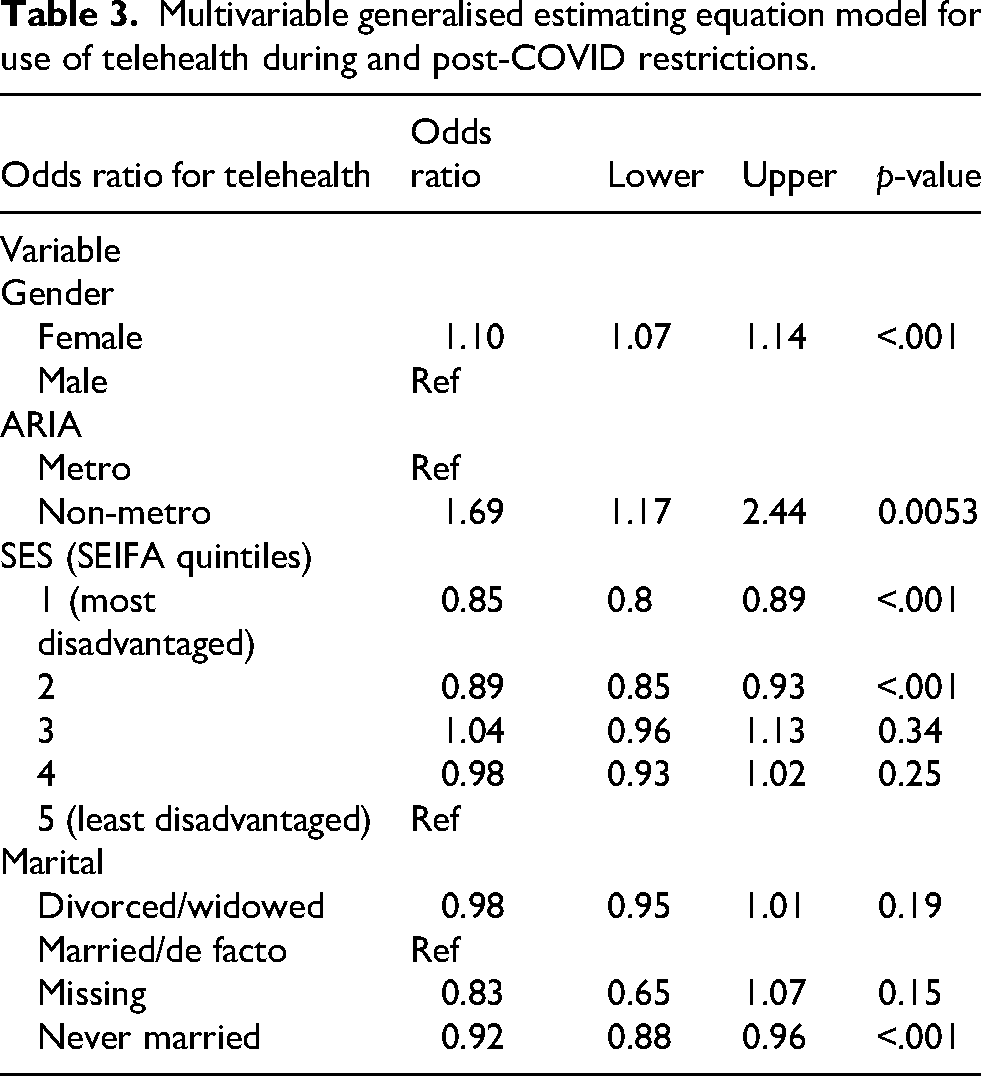
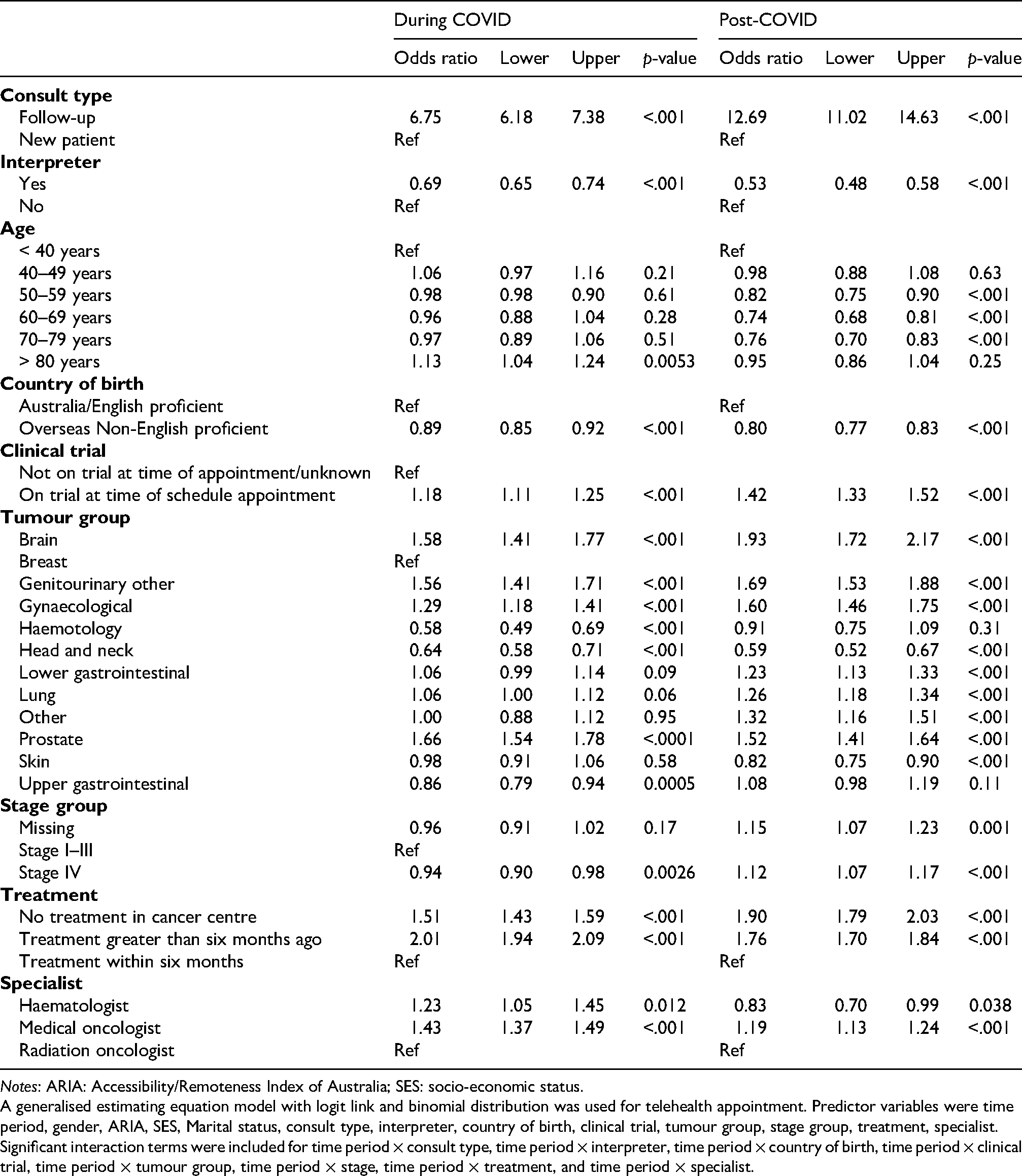
Notes: ARIA: Accessibility/Remoteness Index of Australia; SES: socio-economic status.
A generalised estimating equation model with logit link and binomial distribution was used for telehealth appointment. Predictor variables were time period, gender, ARIA, SES, Marital status, consult type, interpreter, country of birth, clinical trial, tumour group, stage group, treatment, specialist. Significant interaction terms were included for time period × consult type, time period × interpreter, time period × country of birth, time period × clinical trial, time period × tumour group, time period × stage, time period × treatment, and time period × specialist.
Consultations that required the use of an interpreter were less likely to use telehealth than those that did during the COVID-19 restrictions and this trend persisted beyond the COVID-19 restrictions (OR 0.53, 95% CI [0.48–0.58], p < .0001). Patients who were born overseas in a non-English proficient country were less likely to use telehealth than those born in Australia or an English-proficient country and this phenomenon was seen both during and after COVID-19 restrictions (OR 0.80, 95% CI [0.77–0.83], p < .0001). Using breast cancer as a reference, consultations involving patients diagnosed with certain primary tumours were more likely to use telehealth, including brain (OR 1.93, 95% CI [1.72–2.17], p < .0001, prostate cancer (OR 1.52, 95% CI [1.41–1.64], p < .0001), other genitourinary tumours (OR 1.69, 95% CI [1.53–1.88], p < .0001) and gynaecological tumours (OR 1.60, 95% CI [1.46–1.75], p < .0001). Consultations involving patients diagnosed with tumour types that were less likely to utilise telehealth included Head and Neck (OR 0.59, 95% CI [0.52–0.67], p < .0001) and skin cancers (OR 0.82, 95% CI [0.75–0.90], p < .0001).
Compared to patients currently on active treatment at the cancer centre, there was greater use of telehealth for consultations with patients that had treatment at the cancer centre greater than six months ago (OR 1.76, 95% CI [1.70–1.84], p < .0001) and those who never had treatment in the centre (OR 1.90, 95% CI [1.79–2.03], p < .0001). Compared to new patient consultations, there was a far higher proportion of follow-up telehealth consultations with a greater difference after the COVID-19 pandemic (OR 12.69, 95% CI [11.02–14.63], p < .001). Compared to Radiation Oncologists, consultations with medical oncologists were more likely to utilise telehealth (OR 1.19, 95% CI [1.13–1.24], p < .0001). Patients enrolled on clinical trials were more likely to utilise telehealth than those not enrolled at the time of their consultation (OR 1.42, 95% CI [1.33–1.52], p < .0001).
Notably, the direction and magnitude of these associations were largely similar both during and after COVID-19 pandemic restrictions.
Discussion
Prior to the COVID-19 pandemic, there was minimal use of telehealth for cancer care in Australia, with government reimbursement limited to patients living outside of metropolitan areas having consultations with medical specialists. As a part of its initial response to the COVID-19 pandemic, the Australian government rolled out temporary telehealth item numbers under the Medicare Benefits Schedule (MBS) to encourage the use of telehealth and reduce the risk of viral transmission in all patients, including those residing in metropolitan areas. 21 The Australian Government then introduced permanent telehealth MBS item numbers from 1 January 2022 to build on the temporary telehealth item numbers that were introduced as part of the COVID-19 pandemic response. These item numbers have allowed clinicians to use telehealth consultations to deliver clinical services.
Our study demonstrated that as expected, telehealth use peaked during the COVID-19 pandemic, but continued at a reduced level after restrictions were lifted. Telehealth is often cited as having many people-centric advantages including eliminating the need for travel and parking costs, reduced financial and time toxicity and reducing pressure on caregivers.22,23 The ongoing use of telehealth worldwide beyond the COVID-19 pandemic reflects a partial shift in the modality to deliver care, providing a convenient option for appropriate patients which mitigates disruption to activities of daily living.24,25
The American Society of Clinical Oncology (ASCO) has provided standards and guidance for which patient consultations in oncology may be suitable for telehealth. 15 The patterns of telehealth utilisation in our study often reflected these guidelines recommendations. In-person consultations are preferred for certain situations such as new patient consultations, often before rapport is established between a clinician and a patient. The ASCO guidelines also recognise that situations such as the initial delivery of antineoplastic treatment, delivery of key information and consultations that involve complex needs may be more suited to in-person consultations. There were more increased telehealth consultations in our study for established patients as well as follow-up and survivorship care, compared to patients who were on active treatment. While our study supported this hybrid model in the predominantly metropolitan setting, there remain clinical scenarios and geographical contexts where a fully telehealth model of care including new patient consultations effectively maintains high-quality specialist cancer services for patients in remote settings. 6
Our study also demonstrated differences in telehealth utilisation between different tumour groups. There is a higher need for physical examination in certain tumour groups (such as assessing response to treatment in-person for skin cancer or head and neck cancers) and physical examination being less routine in others (such as an appointment to follow up on a PSA blood test in a patient with prostate cancer) that may explain the divergence in telehealth utilisation between different cancer types.26,27 The benefit of virtual consultations is also greater in patients in whom travel is more burdensome, such as those with primary CNS tumours and limited mobility. 28 Some treatment modalities are also more amenable to telehealth utilisation than others, such as patients receiving oral antineoplastic therapies, compared to those requiring in-person interventions (radiation or infusions).15,29 There was a higher proportion of telehealth use amongst Stage IV cancer patients in the post-COVID period, likely due to greater symptom severity and when functional decline made travel to the clinic more challenging.30,31
Although government policy for telehealth in Australia encourages the use of video consultation over phone consultations, phone was the predominant modality utilised in our study both during and after the COVID-19 restrictions. Reasons for the lack of uptake of video conferencing may be from patient and/or clinician unfamiliarity, workflow disruption, the lack of appropriate technology infrastructure and time constraints for setup and troubleshooting in the clinic.32,33 A scoping review of telehealth barriers across specialities found that inadequate internet access, insufficient device availability and low digital literacy particularly amongst older and socioeconomically disadvantaged patients were major factors limiting video consultation adoption in cancer care, resulting in greater reliance on telephone consultations. 34 This mirrors the wider Australian reimbursements for MBS specialist telehealth item numbers (across all medical specialities); when temporary item numbers were introduced during the COVID-19 pandemic, 15% of all consultations were delivered via phone while video consultations accounted for only 4%. 35
Our study also demonstrated a lower uptake of telehealth in patients residing in lower socio-economic areas, including in the post-pandemic restriction period. Other studies have demonstrated reduced access to telehealth for groups in lower socio-economic areas due to lack of access to technology and poor digital literacy.36–38 An equity-focused framework with targeted interventions such as subsidised devices, digital training and community outreach may be required to ensure that the ongoing use of telehealth does not perpetuate existing inequities in accessing cancer care. 39
Similarly, our study also identified lower proportional use of telehealth for consultations with those born in non-English proficient countries and those that required an interpreter. Patients from culturally and linguistically diverse (CALD) backgrounds already experience significant disparities in accessing healthcare and cultural or language barriers may be amplified when trying to access virtual care or communicating through telehealth.40,41 CALD patients may also be less likely to be offered telehealth due to challenges such as integrating interpreters into workflows, resulting in poorer patient and carer satisfaction and outcomes. 42 It is vital to ensure provisions are made for underserved groups to also have the optionality of choosing to use telehealth if desired, to ensure equity and access to care for these groups of patients through culturally appropriate and competent virtual care services, including seamless access to interpreters.
Finally, an area where there is increasing potential for the use of telehealth is in oncology clinical trials. There is now increased acceptance of decentralised clinical trials (DCTs) in oncology, in which one or more components of a clinical trial (such as telehealth consultation with a doctor) is done away from the central research site. 43 This uptake was accelerated by the COVID-19 pandemic, during which the majority of clinical trial sponsors incorporated telehealth as a DCT element, reflecting strong uptake of virtual consultations to ensure uninterrupted trial recruitment and participation. 44 The telehealth frameworks established during the COVID-19 pandemic have allowed ongoing growth of DCTs in oncology, enabling remote patient screening, assessment and follow-up outside of traditional clinical trial sites. The appeal of telehealth is amplified in clinical trials as trial sites are often situated far away from patients, especially those living in regional and remote areas, compared to standard oncology care that often can be accessed at a local hospital. Although clinical research has many benefits, trial participation often poses a time, cost and logistical burden onto patients who not only need to travel to a study centre for treatment administration, but also for additional monitoring, biospecimen collection and survey completion. 45 The increasing use and acceptance of decentralised elements including telehealth in oncology clinical trials beyond the COVID-19 pandemic will help patients access more clinical research in the future. 44
Strengths and limitations
The large sample size and the long duration of the study timeframe encompassing different time periods before, during and after the COVID-19 pandemic are major strengths of the study. The study also extracts specific patient, cancer and treatment level data beyond what can be extracted from MBS reimbursement data alone. Limitations of this study include the possibility of an underestimation of the number of consultations due to a reliance on oncology information systems data and a lack of further details regarding the consultations such as length of time taken. The data is also limited to a specific region in Sydney, Australia that may not be widely generalisable at a national or international level.
Conclusion
Our study demonstrated reduced but sustained use of telehealth in oncology beyond the COVID-19 pandemic, in line with national and international trends. The trends in subgroups more likely to use telehealth remained similar in both during and after COVID-19 pandemic restriction periods. Although telehealth is a useful adjunct to in-person modes of care delivery in the metropolitan setting, it remains comparatively underutilised in disadvantaged populations. Initiatives and policies to help reduce disparate use of telehealth in cancer care are required. The ongoing use of telehealth needs to be particularly available for patients who typically require excessive travel, such as those needing to access specialised clinical trial sites. As alternative virtual models of care emerge across subgroups in oncology, strategic implementation of telehealth is central to ensuring patient-centred care.
Quarterly trends in oncology outpatient consultations by modality and type 2019–2024. Forest plot of adjusted odds ratios for telehealth use by key covariates in during and post-COVID-19 restriction periods.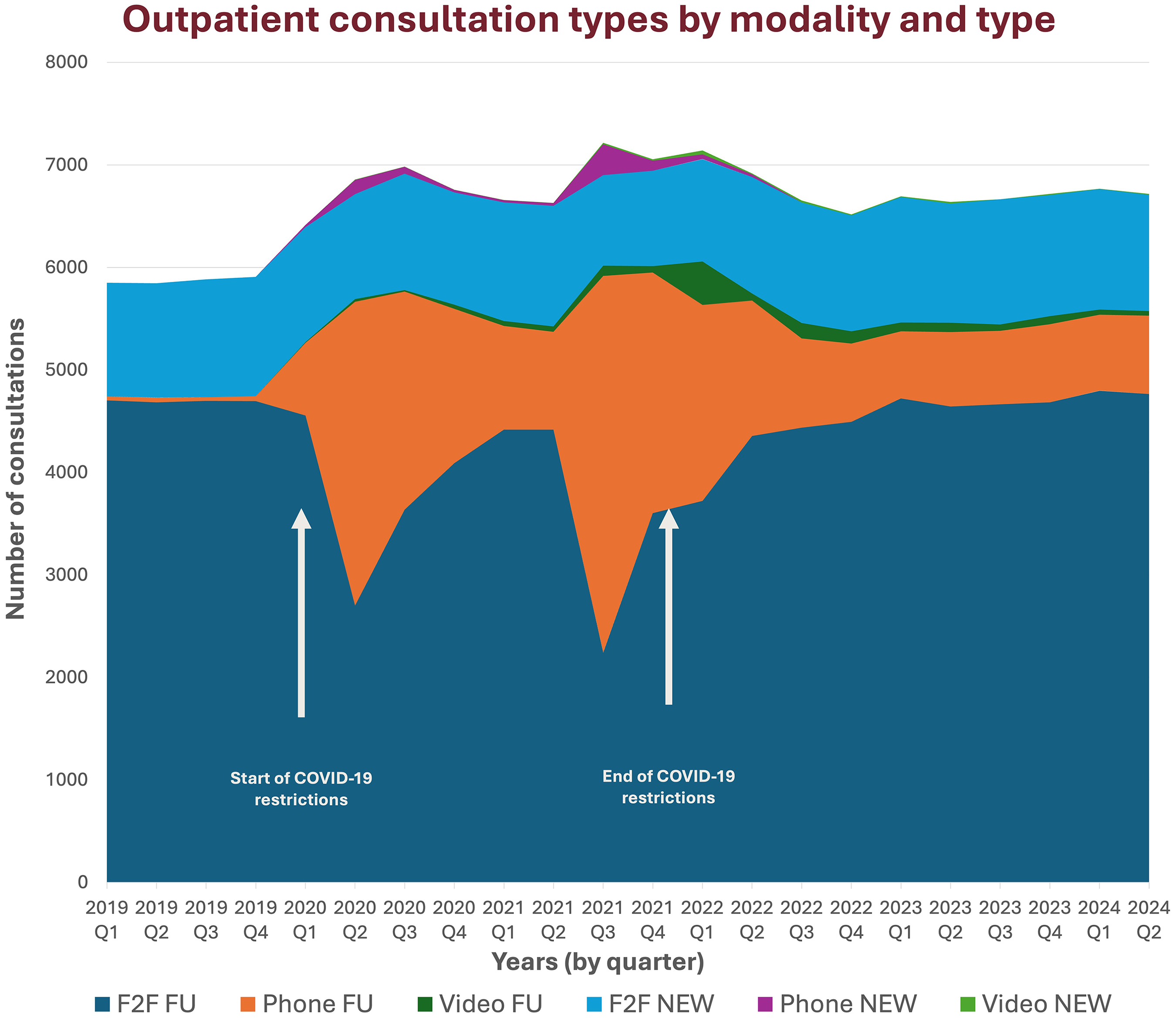
Footnotes
Author contributions
Andrew Parsonson: conception or design of the work, data collection, data analysis and interpretation, drafting the article, critical revision of the article and final approval of the version to be published; Jiawang Cao: data collection, data analysis and interpretation, critical revision of the article, and final approval of the version to be published; Joseph Descallar: data analysis and interpretation, drafting the article, critical revision of the article, and final approval of the version to be published; Gui Xiong: conception or design of the work, data collection, data analysis and interpretation, critical revision of the article, and final approval of the version to be published; Deme Karikios: conception or design of the work, drafting the article, critical revision of the article, and final approval of the version to be published; Frances Boyle: conception or design of the work, drafting the article, critical revision of the article, final approval of the version to be published; Annie YS Lau: conception or design of the work, drafting the article, critical revision of the article, final approval of the version to be published; Mei Ling Yap: conception or design of the work, data collection, data analysis and interpretation, drafting the article, critical revision of the article, and final approval of the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from The Radiation Oncology Virtual Clinical Quality Data Registry platform but restrictions apply to the availability of these data, which were used under licence for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of The Radiation Oncology Virtual Clinical Quality Data Registry platform.